In which types of brain bleed, mannitol is contraindicated
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
mannitol contraindicated types of intracranial hemorrhage brain bleed
Finding Sources
Finding Sources
Finding Sources
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK470392
Here is a thorough answer on when mannitol is contraindicated in the setting of brain bleeds:
Mannitol Contraindications in Intracranial Hemorrhage
The Core Contraindication: Active Intracranial Bleeding
Mannitol is formally contraindicated in active intracranial bleeding - this is an FDA-labeled contraindication. The one exception is during craniotomy (when the skull is open and the bleeding can be directly controlled surgically).
This applies to the following types of active brain bleeds:
| Type of Bleed | Mannitol Status |
|---|---|
| Active intracerebral hemorrhage (ICH) | Contraindicated |
| Active subarachnoid hemorrhage (SAH) | Contraindicated |
| Active subdural hematoma (SDH) | Contraindicated |
| Active epidural hematoma (EDH) | Contraindicated |
| Any active intracranial bleed (except during craniotomy) | Contraindicated |
Why Mannitol Is Dangerous in These Settings
The reason is mechanistic and important:
-
Disrupted blood-brain barrier (BBB): Mannitol's ICP-lowering effect depends on an intact BBB. It works by creating an osmotic gradient that draws water out of healthy brain tissue into the bloodstream. In hemorrhage, the BBB is disrupted around the bleed.
-
Reverse osmotic effect: When the BBB is injured (as in hemorrhage), mannitol crosses the damaged vessels more easily and accumulates in the brain tissue. This reverses the osmotic gradient - drawing water into the brain instead of out, worsening cerebral edema. This is called rebound cerebral edema (StatPearls, NCBI Bookshelf NBK470392).
-
Hematoma expansion: The reduction in brain volume from osmotic diuresis can cause shifts in brain compartments and potentially expand hematomas.
-
Subdural hematoma risk from mannitol itself: Rapid osmotic diuresis caused by mannitol can actually cause subdural hematoma in elderly patients by rupturing fragile bridging veins as the brain shrinks away from the skull - Morgan & Mikhail's Clinical Anesthesiology notes this as a recognized complication.
Special Note on Chronic/Stable Bleeds
The contraindication specifically targets active bleeding. In some clinical scenarios (e.g., established hematoma with surrounding edema and mass effect), mannitol may still be used cautiously as a bridge to surgery - this is a clinical judgment call rather than a blanket rule.
Summary
Mannitol is contraindicated in ALL types of active intracranial hemorrhage (ICH, SAH, SDH, EDH) - except during craniotomy - because it crosses the damaged blood-brain barrier and can worsen edema rather than reduce it.
The key phrase in the FDA labeling is: "Active intracranial bleeding except during craniotomy."
How to identify whether the bleed is active or not
Finding Sources
Finding Sources
Searching the Web
how to identify active vs non-active intracranial hemorrhage CT scan spot sign hematoma expansion
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a thorough breakdown of how to identify whether an intracranial bleed is active or not:
Identifying Active vs. Inactive Intracranial Hemorrhage
1. Clinical Clues (Bedside Assessment)
| Feature | Suggests Active Bleeding | Suggests Stable/Old Bleed |
|---|---|---|
| Time since onset | < 6 hours ("hyperacute") | > 24-48 hours |
| Neurological status | Rapidly worsening, declining GCS | Stable or improving |
| Blood pressure | Severely elevated (ongoing driving pressure) | Controlled or normalized |
| Coagulopathy present | Yes (warfarin, DOAC, thrombocytopenia) | Corrected or absent |
| Symptom onset | Sudden, maximal at onset (SAH), or stepwise progression | Plateau or improving |
2. CT Angiography (CTA) - The Spot Sign (Most Important Radiological Marker)
The CT angiography spot sign is the key imaging marker of active/ongoing bleeding.
Definition: Tiny enhancing foci (dots of contrast extravasation) seen within the hematoma on CTA - representing active contrast leaking from a ruptured vessel into the clot.
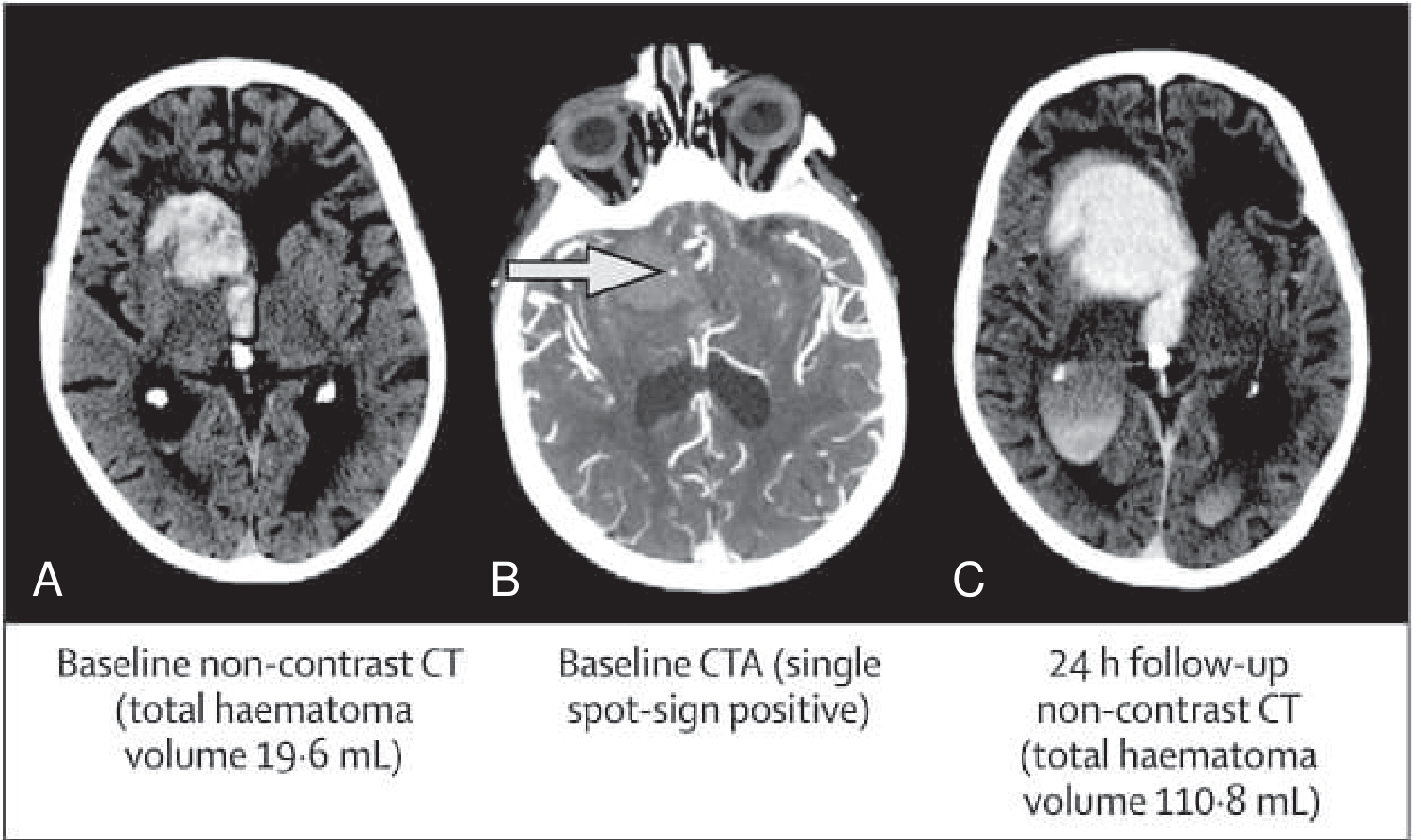
Significance of spot sign:
- Predicts hematoma expansion (validated by the multicenter PREDICT study)
- Associated with increased 30-day mortality and poor functional outcome
- Spot sign frequency decreases over time: ~39% within 2 hours of onset, dropping to ~13% beyond 8 hours
- Venous phase CTA is slightly more sensitive than arterial phase (sensitivity 55% arterial vs. 64% with 90-second delayed acquisition)
3. Non-Contrast CT (NCCT) Signs of Active/Evolving Hemorrhage
These NCCT features predict high risk of hematoma expansion (a surrogate for active/ongoing bleeding):
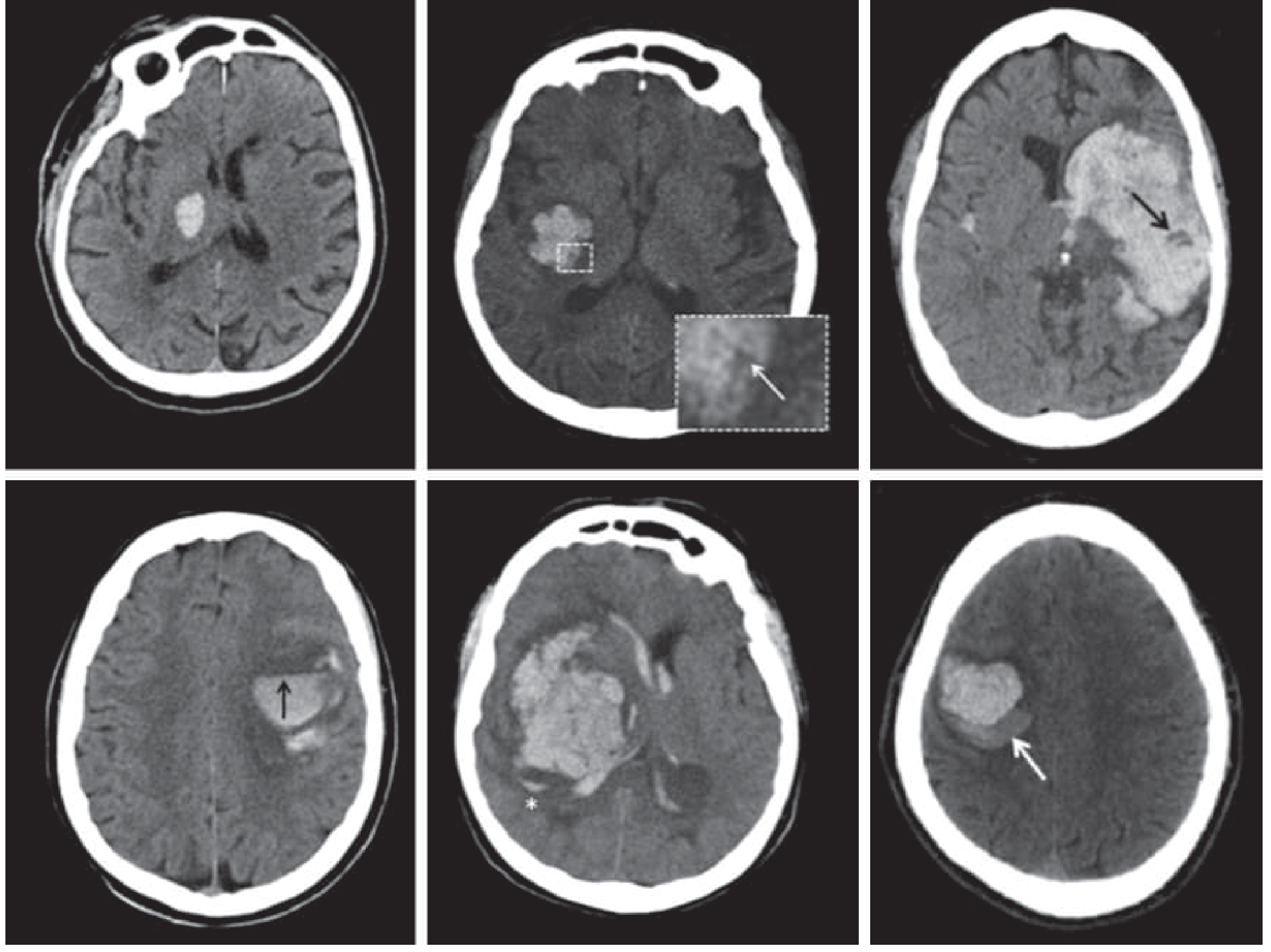
| NCCT Sign | Appearance | Significance |
|---|---|---|
| Swirl sign | Dark (hypodense) swirling areas within bright clot | Active bleeding mixing with clot; high-risk |
| Fluid-blood level | Horizontal line separating hyperdense clot from hypodense fluid | Suggests ongoing/recent bleeding |
| Satellite sign | Small separate hematoma foci adjacent to main hematoma | High expansion risk |
| Blend sign | Two adjacent regions of different density within hematoma | High expansion risk |
| Irregular/heterogeneous shape | Non-round, lobulated hematoma margins | Expansion risk |
| Regular, homogeneous, round shape | Uniform density throughout | Lower expansion risk, more likely stable |
4. MRI - Temporal Staging of Hemorrhage
MRI signal intensity changes allow precise aging of a hemorrhage:
| Stage | Time | Hemoglobin Form | T1 Signal | T2 Signal | Interpretation |
|---|---|---|---|---|---|
| Hyperacute | First few hours | Oxyhemoglobin | Iso/low | High | Very fresh bleed |
| Acute | Hours - days | Deoxyhemoglobin | Low | Low | Active/recent |
| Early subacute | Days 2-7 | Methemoglobin (intracellular) | High | Low | Days old |
| Late subacute | Days 7-14 | Methemoglobin (extracellular) | High | High | 1-2 weeks old |
| Chronic | Weeks-months | Hemosiderin | Low | Low ("blooming") | Old bleed |
A bleed showing oxyhemoglobin or deoxyhemoglobin signal on MRI is recent and likely still active or at high risk of re-bleeding.
5. Serial Imaging (Gold Standard for Confirming Expansion)
Per Harrison's Principles of Internal Medicine: in ~30-40% of ICH cases, the hemorrhage enlarges in the first 6-12 hours. A repeat NCCT at 6-24 hours showing increased hematoma volume (>33% increase or >6 mL absolute growth is the standard definition of hematoma expansion) confirms active/continued bleeding.
Practical Summary
- Spot sign on CTA = strongest single marker of active bleeding
- Hyperacute presentation (< 6 hours) + worsening neurology = assume active
- NCCT heterogeneity signs (swirl, blend, satellite, fluid level) = high expansion risk
- MRI staging gives temporal context but isn't used in emergencies
- Serial CT confirming growth = definitive proof of expansion
In clinical practice, the absence of the spot sign on CTA, a homogeneous/round hematoma on NCCT, neurological stability, and symptom onset > 24 hours are collectively reassuring that the bleed has stabilized.
This is a shared conversation. Sign in to Orris to start your own chat.