Precious puberty
Reading File
Finding Sources
Searching PubMed
"precocious puberty"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Precocious Puberty
(You likely meant "precocious puberty" - puberty that begins abnormally early.)
Definition
Precocious puberty is the appearance of secondary sexual characteristics before the normal age thresholds:
- Girls: before 8 years of age (some societies use 7 for white girls, 6 for Black girls as the cutoff for evaluation)
- Boys: before 9 years of age
The Lawson Wilkins Pediatric Endocrine Society guidelines specify that breast development or pubic hair in white girls before age 7, in Black girls before age 6, and in boys of all races before age 9 warrants evaluation. - Textbook of Family Medicine 9e
Classification
1. Central (Gonadotropin-Dependent) Precocious Puberty (CPP)
- Results from premature activation of the hypothalamic-pituitary-gonadal (HPG) axis
- LH and FSH are elevated (pulsatile GnRH secretion begins prematurely)
- Also called "true precocious puberty" or "isosexual precocity"
2. Peripheral (Gonadotropin-Independent) Precocious Puberty (PPP)
- Sex steroid secretion occurs independent of LH and FSH stimulation
- Also called "pseudo-precocious puberty"
- Low/suppressed LH with elevated sex steroids
3. Incomplete / Benign Variants
These do not require treatment and often resolve spontaneously:
- Isolated premature thelarche - breast development only, no other signs; usually self-limited, especially in girls under 2 years
- Isolated premature pubarche/adrenarche - pubic hair only; usually self-limited
- Isolated premature menarche
Causes
Central Precocious Puberty (Gonadotropin-Dependent)
| Cause | Notes |
|---|---|
| Idiopathic | 90% of girls; only 10% of boys |
| CNS tumors | Hypothalamic hamartoma, optic glioma, astrocytoma, ependymoma, arachnoid cysts, tuberous sclerosis |
| Inflammatory/infectious lesions | Meningitis, encephalitis |
| Genetic mutations | KISS1 (kisspeptin), KISS1R (kisspeptin receptor), MKRN3 (makorin ring finger protein 3) |
| hCG-secreting tumors | Germinomas (hypothalamic or pineal) |
In boys with CPP, CNS disease accounts for ~two-thirds of cases. - Goldman-Cecil Medicine
Peripheral Precocious Puberty (Gonadotropin-Independent)
| Cause | Sex |
|---|---|
| Congenital adrenal hyperplasia (CAH) | Both (especially virilizing forms) |
| McCune-Albright syndrome | Mostly girls |
| Activating LH receptor mutations ("testotoxicosis") | Boys |
| Activating Gα subunit mutations | Both |
| Androgen/estrogen-secreting adrenal or gonadal tumors | Both |
| Exogenous sex steroids | Both |
| Primary hypothyroidism (Van Wyk-Grumbach) | Girls |
Epidemiology
- Precocious puberty is 20 times more common in girls than boys
- In girls, 90% of cases are idiopathic (central)
- In boys, ~10% are idiopathic; the majority have an identifiable organic cause (especially CNS)
- A secular trend toward earlier puberty onset has continued over the past century, partly due to improved nutrition and rising obesity rates - Harrison's 22E
Clinical Features
- Early development of secondary sexual characteristics (breasts, pubic/axillary hair, genital development)
- Accelerated linear growth and advanced bone age
- Risk of early epiphyseal closure leading to reduced adult height
- Psychosocial consequences (emotional immaturity combined with physical development)
- Long-term risks: increased risk of breast and endometrial cancer, cardiovascular disease, hypertension, type 2 diabetes, shorter life span
Diagnostic Evaluation
Step 1: History and physical examination
- Family and birth history; timing and tempo of pubertal development
- Neurologic symptoms; abdominal masses; skin lesions (cafe-au-lait spots suggest McCune-Albright)
- Assign Tanner stage
Step 2: Initial labs and imaging
- Bone age (plain X-ray of left hand/wrist)
- Basal LH, FSH, and sex steroids (testosterone or estradiol)
- Thyroid function (TSH, T4)
Step 3: Branch based on lab results (see diagnostic flowchart below)
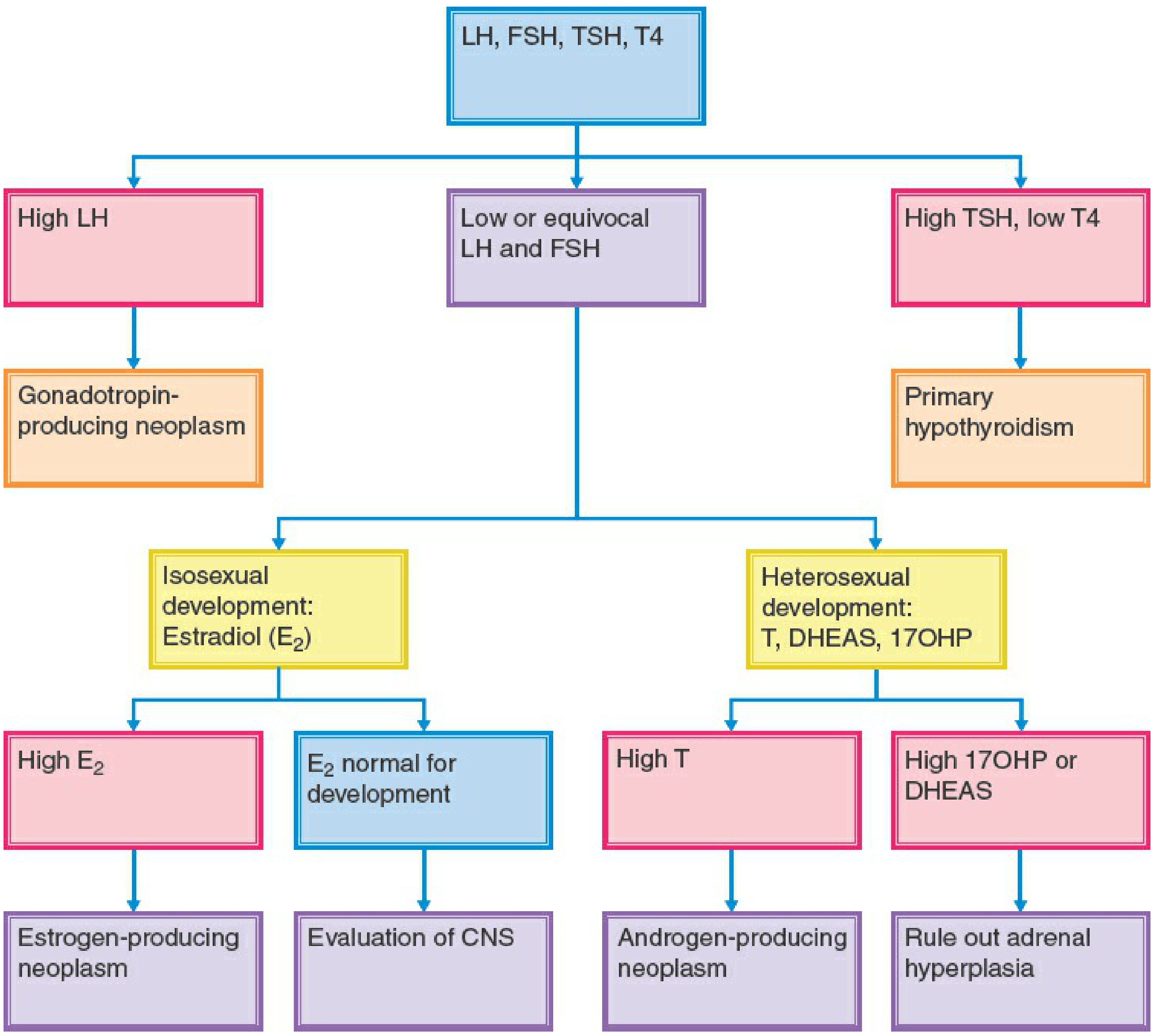
If gonadotropin-dependent (high LH/FSH):
- MRI of brain/head to exclude CNS lesion
- If no lesion found → idiopathic CPP
If gonadotropin-independent (high sex steroids, suppressed LH):
- Measure DHEAS and 17α-hydroxyprogesterone
- High 17-OHP → CAH (21-hydroxylase or 11β-hydroxylase deficiency)
- High DHEAS → adrenal tumor (CT adrenals)
- High testosterone without 17-OHP/DHEAS elevation → testicular palpation and ultrasound (Leydig cell tumor)
- Consider activating LH receptor or Gα mutations if above excluded
Treatment
Central (Gonadotropin-Dependent) Precocious Puberty
Goal: Suppress premature HPG axis activation, protect final adult height, reduce psychosocial impact
GnRH analogues (first-line):
- Leuprolide acetate - 3-month depot 11.25 mg or 30 mg; or 6-month depot 22.5 mg
- Triptorelin - 22.5 mg every 6 months (6-month depot)
- Suppress LH/FSH and sex steroids
- Halt pubertal progression, delay bone maturation, prevent early epiphyseal closure
- Most effective for height if initiated before age 6
- Puberty resumes after discontinuation
- No consensus on optimal age to stop; commonly around age 11-11.5 years
If an underlying CNS lesion is found: surgery or radiation therapy directed at the cause.
Peripheral (Gonadotropin-Independent) Precocious Puberty
| Cause | Treatment |
|---|---|
| CAH | Glucocorticoids (hydrocortisone 15 mg/m²/day) |
| Familial male-limited precocious puberty (testotoxicosis) | Ketoconazole (10-20 mg/kg/day) ± antiandrogen (spironolactone 5-7 mg/kg/day or bicalutamide 2 mg/kg/day) |
| McCune-Albright / aromatase excess | Aromatase inhibitors (testolactone, letrozole) |
| Adrenal/testicular tumors | Surgical resection |
| Primary hypothyroidism | Thyroid hormone replacement |
| Abiraterone | Newer testosterone synthesis inhibitor; not yet systematically evaluated in children |
Counseling is an important component of the overall management strategy for all types.
Key Points Summary
| Feature | Central (CPP) | Peripheral (PPP) |
|---|---|---|
| Gonadotropins | Elevated (high LH/FSH) | Suppressed |
| Mechanism | Premature HPG axis activation | Autonomous sex steroid production |
| Girls | 90% idiopathic | McCune-Albright, ovarian cysts/tumors |
| Boys | ~2/3 have CNS disease | CAH, testotoxicosis, adrenal tumors |
| Treatment | GnRH analogues | Treat underlying cause |
Sources: Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine International Edition; Berek & Novak's Gynecology; Textbook of Family Medicine 9e
Complications for this
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
I now have enough content from multiple textbooks to give a thorough, well-cited answer on complications.
Complications of Precocious Puberty
Complications fall into three broad categories: physical/growth, long-term metabolic and oncologic, and psychosocial.
1. Short Stature (Most Important Physical Complication)
Early sex steroid exposure causes premature epiphyseal (growth plate) closure, cutting short the window for longitudinal bone growth. Despite the initial growth acceleration that makes these children temporarily tall for their age, they often end up with a reduced final adult height.
- Skeletal (bone) age is advanced relative to chronologic age
- Bone age is more closely correlated with pubertal stage than chronologic age during puberty; it is used with the Bayley-Pinneau tables to predict final adult height
- Treatment with GnRH analogues is most effective at preserving height if started before age 6
- Medroxyprogesterone acetate does not always prevent premature epiphyseal closure and resultant short stature
- GnRH analogues that reversibly inhibit gonadotropin secretion can prevent secondary sexual development and early epiphyseal fusion - Textbook of Family Medicine 9e
2. Long-Term Metabolic and Oncologic Risks
Harrison's 22E explicitly lists these increased risks associated with earlier onset of puberty:
| Complication | Notes |
|---|---|
| Breast cancer | Longer lifetime estrogen exposure |
| Endometrial cancer | Early estrogen stimulation of endometrium |
| Cardiovascular disease | Linked to early hormonal changes and associated metabolic shifts |
| Hypertension | Part of the cardiometabolic risk cluster |
| Type 2 diabetes mellitus | Especially when precocious puberty is obesity-related |
| Shorter life span | Observed epidemiologically with earlier puberty onset |
| Hair pigmentation changes | Also documented in early-puberty cohorts |
Earlier onset of puberty is associated with increased risk of breast and endometrial cancer, cardiovascular disease, hypertension, type 2 diabetes, hair pigmentation, and shorter life span. - Harrison's Principles of Internal Medicine 22E
3. Psychosocial and Behavioral Complications
This is often underappreciated but is a major driver of treatment decisions:
- Emotional/behavioral immaturity - the child's psychological development does not match their physical appearance, creating significant internal and social conflict
- Social stigmatization - peers, strangers, and even family may treat the child according to their physical age rather than emotional age
- Depression and anxiety - documented consequence of premature physical development
- Sexual abuse vulnerability - physically developed girls are at higher risk
- Disrupted peer relationships - the child looks and is treated differently, leading to social isolation
- Prompt treatment can prevent or attenuate emotional consequences in the patient and her parents - Goldman-Cecil Medicine
4. Complications Specific to Underlying Causes
Since precocious puberty is often a sign of an underlying condition, complications may also arise from the causative pathology:
| Underlying Cause | Additional Complications |
|---|---|
| CNS tumors (hypothalamic hamartoma, glioma, etc.) | Visual field defects, raised intracranial pressure, seizures, neurologic deficits |
| McCune-Albright syndrome | Polyostotic fibrous dysplasia (bone fractures, deformity), cafe-au-lait skin lesions, hyperthyroidism, Cushing's syndrome |
| CAH | Adrenal crisis, salt-wasting, virilization, hypertension (11β-hydroxylase form) |
| Gonadal/adrenal tumors | Malignant potential, mass effects |
| Testotoxicosis | Infertility if untreated (Leydig cell hyperplasia) |
5. Reproductive Complications
- Menstrual irregularity in girls if the underlying axis is dysregulated - oligomenorrhea, dysfunctional uterine bleeding
- In the Robbins Pathology tables, precocious puberty (hypothalamic, pituitary, or ovarian origin) is listed as a cause of abnormal uterine bleeding in the prepubertal period - Robbins & Kumar Basic Pathology
Summary Table
| Category | Complication |
|---|---|
| Growth | Short final adult height (early epiphyseal closure) |
| Metabolic | Type 2 diabetes, hypertension, cardiovascular disease |
| Oncologic | Breast cancer, endometrial cancer |
| Psychosocial | Depression, stigmatization, behavioral issues, sexual abuse risk |
| Neurologic | From underlying CNS lesions |
| Reproductive | Menstrual irregularity, potential fertility issues |
| Disease-specific | Bone fractures (McCune-Albright), adrenal crisis (CAH), tumor-related |
Sources: Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine International Edition; Textbook of Family Medicine 9e; Berek & Novak's Gynecology; Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.