All about leprosy in short note for microbiology 6 marks question
Leprosy (Hansen's Disease) - Short Note
Definition
Causative Organism - Mycobacterium leprae
- Obligate intracellular, rod-shaped, acid-fast bacillus (AFB)
- Dimensions: 1-8 µm length, 0.3 µm diameter
- Weakly acid-fast - best visualized with the Fite stain (not standard Ziehl-Neelsen)
- Cannot be cultured in vitro (no artificial medium supports growth)
- Slow-growing - doubling time ~12-14 days (longest of any known bacterium)
- Infects Schwann cells of peripheral nerves and macrophages
- Grows best in cooler tissues (skin, superficial nerves, nasal mucosa)
- Organisms arranged in parallel arrays within macrophages called globi (lepra cells)
- A second species, M. lepromatosis, causes diffuse lepromatous leprosy (mainly Mexico/Central America)
Epidemiology
- Neglected tropical disease; 174,087 new cases from 182 countries reported in 2022
- India accounts for ~78% of global burden; other endemic countries: Brazil, Nepal, Mozambique, Myanmar
- Non-human reservoir: 9-banded armadillo (Dasypus novemcinctus) in the southern USA
- People with HIV do not appear to have increased susceptibility to M. leprae
- Source: Bailey & Love's Short Practice of Surgery 28E; Red Book 2021
Transmission
- Spread via respiratory droplets/nasal secretions from untreated lepromatous patients
- Requires prolonged close contact (years); not highly contagious
- Household contacts of untreated patients are at increased (but still low) risk
- Incubation period: 2-5 years (can range up to 20 years)
Classification
Ridley-Jopling Classification (1962)
| Type | Abbreviation | Immunity | Bacilli | Granuloma |
|---|---|---|---|---|
| Tuberculoid | TT | Strong | Few (paucibacillary) | Epithelioid + giant cells |
| Borderline Tuberculoid | BT | Good | Few | Epithelioid |
| Mid-Borderline | BB | Unstable | Moderate | Mixed |
| Borderline Lepromatous | BL | Weak | Many | Macrophage |
| Lepromatous | LL | Absent | Abundant (multibacillary) | Macrophage/globi |
WHO Simplified Classification
- Paucibacillary (PB): 1-5 skin lesions, negative slit-skin smear
- Multibacillary (MB): 6+ skin lesions and/or >1 peripheral nerve involved, positive smear
Clinical Features
- Skin: Hypopigmented or erythematous macules/patches with loss of sensation; nodules (lepromas) in LL
- Nerve involvement: Thickened, palpable peripheral nerves - ulnar, median, radial, lateral popliteal, posterior tibial; cranial nerves (trigeminal, facial)
- Anesthesia leading to painless injuries, ulcers, bone resorption, and deformity
- Leonine facies, madarosis (loss of lateral eyebrows), saddle-nose deformity in LL
- Eye: corneal scarring, lagophthalmos, iridocyclitis
- Leprosy is the leading cause of permanent physical disability among infectious diseases
Leprosy Reactions (Acute Exacerbations)
- Type 1 - Reversal Reaction (LR-1): Seen in borderline (BT/BB/BL) types; sudden increase in cell-mediated immunity; acute swelling and tenderness of skin/nerve lesions
- Type 2 - Erythema Nodosum Leprosum (ENL/LR-2): Seen in BL/LL; systemic immune complex-mediated inflammation; tender red nodules, fever, polyarthralgia, lymphadenopathy, iridocyclitis
Diagnosis
- Clinical: Hypesthetic/anesthetic skin patch + nerve thickening + AFB on smear = triad
- Slit-skin smear (SSS): AFB stained with Fite stain; Bacteriological Index (BI) = log-scale 0 to 6+ for bacillary density; Morphological Index (MI) = % viable solid-staining bacilli
- Skin biopsy: Granuloma type helps classify on Ridley-Jopling scale
- Lepromin test (Mitsuda test): Tests cell-mediated immunity - positive in TT (strong immunity), negative in LL; NOT diagnostic, used for classification only
- M. leprae cannot be cultured; molecular PCR available in reference labs
- Demonstration of AFB in peripheral nerves is pathognomonic
Treatment - WHO Multidrug Therapy (MDT)
| Drug | Paucibacillary (PB) | Multibacillary (MB) |
|---|---|---|
| Dapsone | 100 mg/day | 100 mg/day |
| Rifampicin | 600 mg/month (supervised) | 600 mg/month (supervised) |
| Clofazimine | Not included | 50 mg/day + 300 mg/month |
| Duration | 6 months | 12 months |
- WHO provides MDT free of charge worldwide via blister packs
- Treatment failure rates are very low when therapy is completed
- Source: Harrison's 22E, p.1454 (WHO MDT Table)
Key Points for Exam
- Only bacterium known to infect Schwann cells - explains nerve damage
- Cannot be cultured in vitro - diagnosis is clinical/histological
- Tissue damage is inversely proportional to immune response (more damage in TT despite fewer bacilli)
- Lepromin test - not diagnostic; used for prognosis/classification
- India accounts for majority of global burden
- MDT has made leprosy curable; WHO target for elimination (<1 case/10,000 population)
Give flow charts of it
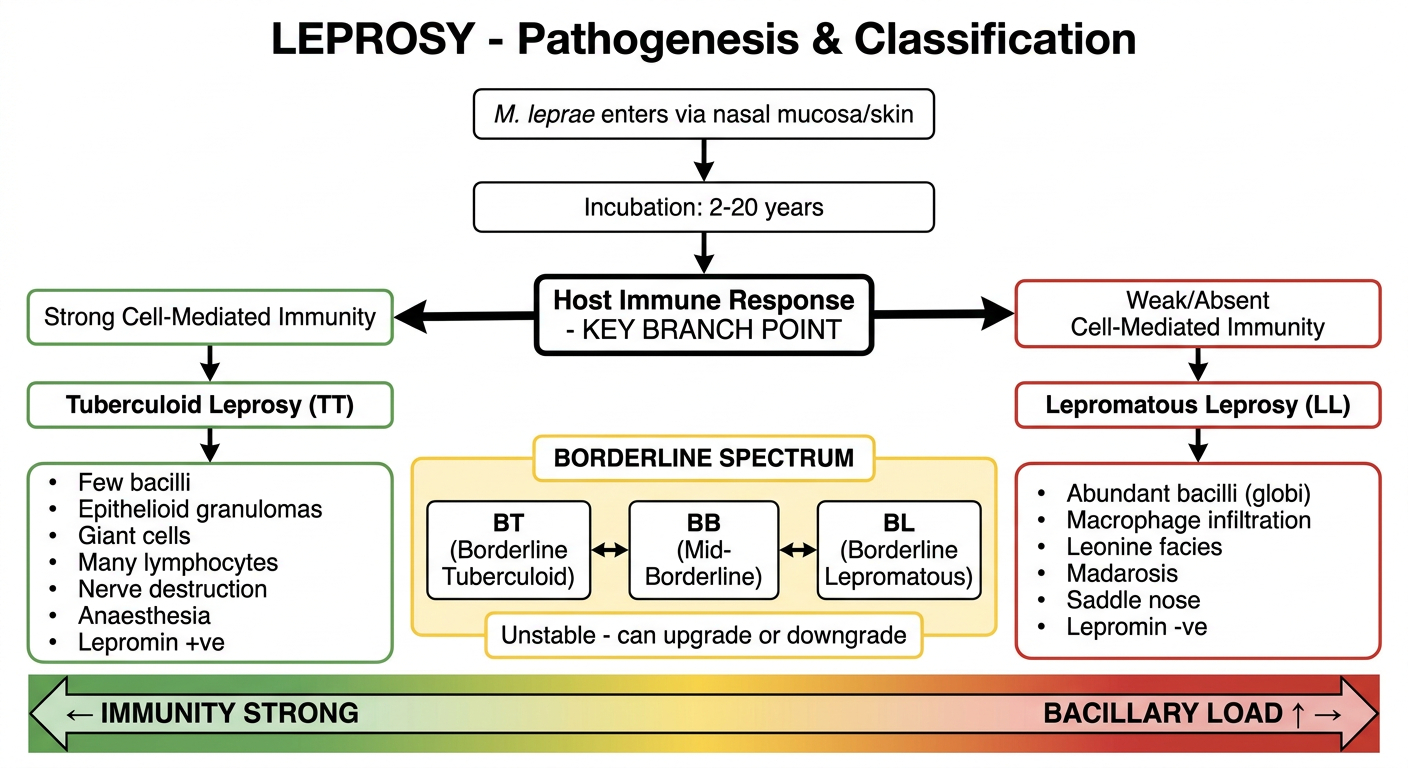
Medical flowchart titled "LEPROSY - Pathogenesis & Classification" on white background. Clean, professional medical diagram style with boxes and arrows. Flow starts at top: [M. leprae enters via nasal mucosa/skin] → [Incubation: 2-20 years] → [Host Immune Response - KEY BRANCH POINT] Then splits into TWO main branches: LEFT BRANCH (Strong CMI): [Strong Cell-Mediated Immunity] → [Tuberculoid Leprosy (TT)] → Features box: "Few bacilli, Epithelioid granulomas, Giant cells, Many lymphocytes, Nerve destruction, Anaesthesia, Lepromin +ve" RIGHT BRANCH (Weak CMI): [Weak/Absent Cell-Mediated Immunity] → [Lepromatous Leprosy (LL)] → Features box: "Abundant bacilli (globi), Macrophage infiltration, Leonine facies, Madarosis, Saddle nose, Lepromin -ve" MIDDLE SPECTRUM (between the two branches): [BORDERLINE SPECTRUM] with three sub-boxes in a row: BT (Borderline Tuberculoid) | BB (Mid-Borderline) | BL (Borderline Lepromatous) Label under: "Unstable - can upgrade or downgrade" At bottom, a horizontal bar labeled: "← IMMUNITY STRONG | BACILLARY LOAD ↑ → " Color coding: Left side green, middle yellow, right side red
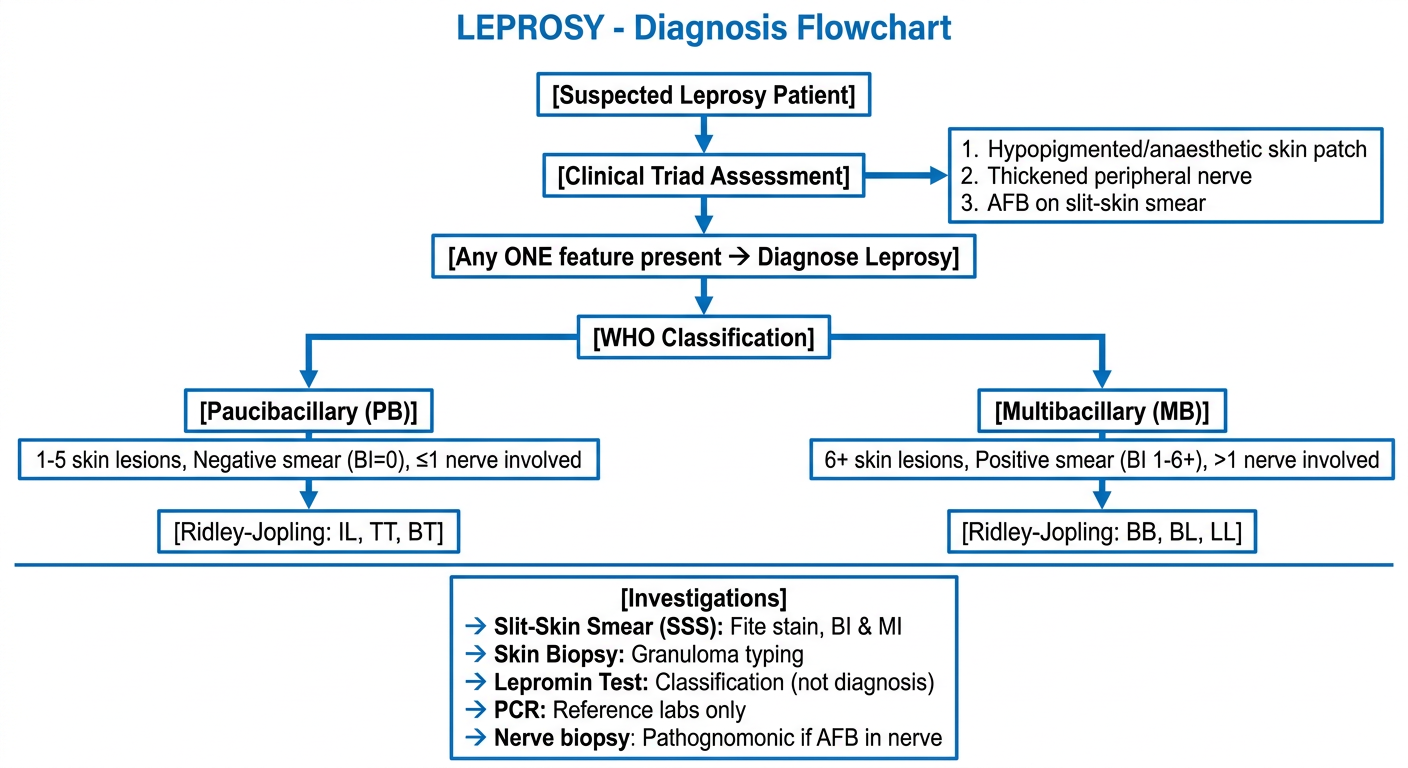
Medical flowchart titled "LEPROSY - Diagnosis Flowchart" on white background. Clean professional style. Start box at top center: [Suspected Leprosy Patient] ↓ [Clinical Triad Assessment] → box: "1. Hypopigmented/anaesthetic skin patch 2. Thickened peripheral nerve 3. AFB on slit-skin smear" ↓ [Any ONE feature present → Diagnose Leprosy] ↓ [WHO Classification] Splits into TWO branches: LEFT: [Paucibacillary (PB)] → "1-5 skin lesions, Negative smear (BI=0), ≤1 nerve involved" RIGHT: [Multibacillary (MB)] → "6+ skin lesions, Positive smear (BI 1-6+), >1 nerve involved" Below each branch, add: PB → [Ridley-Jopling: IL, TT, BT] MB → [Ridley-Jopling: BB, BL, LL] Bottom section - separate box: [Investigations] → Slit-Skin Smear (SSS): Fite stain, BI & MI → Skin Biopsy: Granuloma typing → Lepromin Test: Classification (not diagnosis) → PCR: Reference labs only → Nerve biopsy: Pathognomonic if AFB in nerve Use blue color scheme, arrows between all boxes
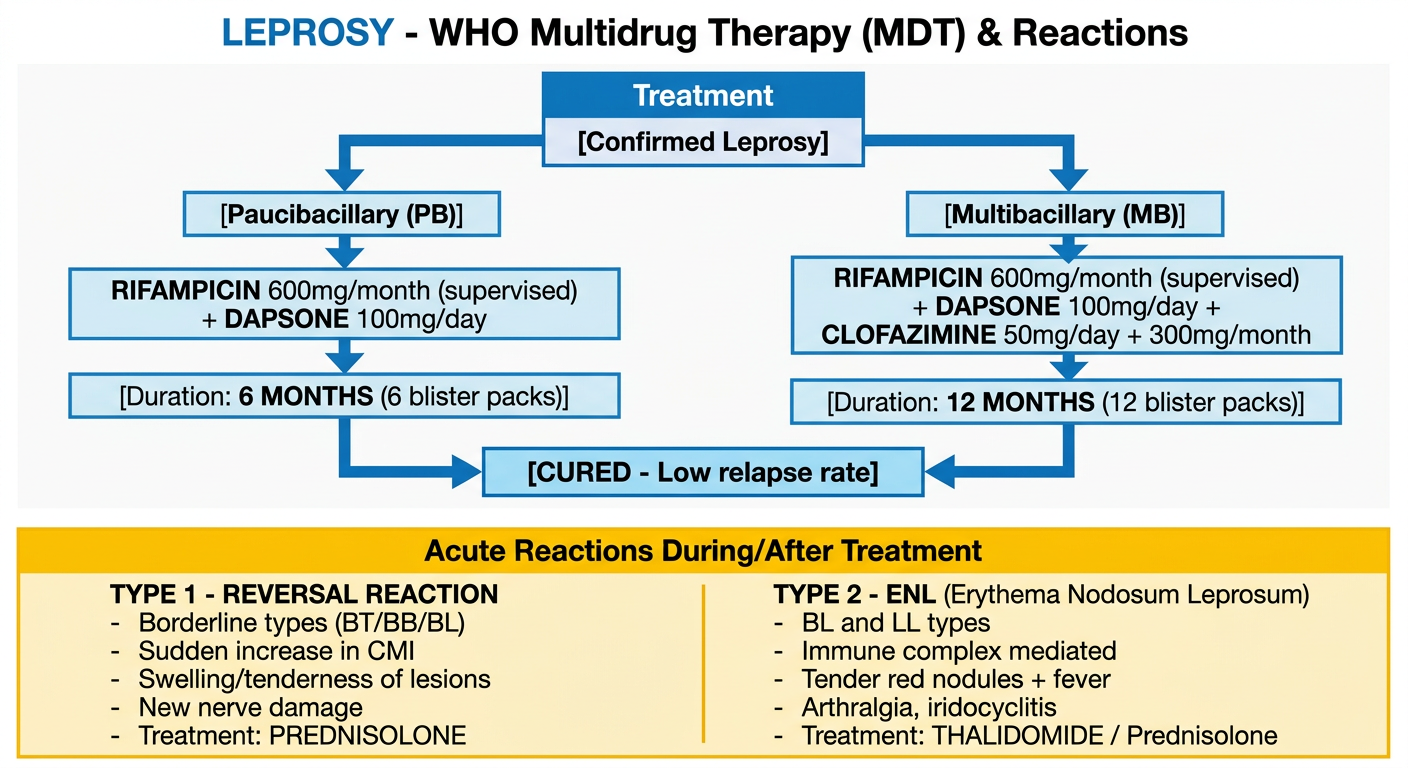
Medical flowchart titled "LEPROSY - WHO Multidrug Therapy (MDT) & Reactions" on white background. Two sections. TOP SECTION - Treatment: [Confirmed Leprosy] ↓ splits into two paths LEFT PATH - [Paucibacillary (PB)]: Box: "RIFAMPICIN 600mg/month (supervised) + DAPSONE 100mg/day" ↓ [Duration: 6 MONTHS (6 blister packs)] RIGHT PATH - [Multibacillary (MB)]: Box: "RIFAMPICIN 600mg/month (supervised) + DAPSONE 100mg/day + CLOFAZIMINE 50mg/day + 300mg/month" ↓ [Duration: 12 MONTHS (12 blister packs)] Both paths converge to: [CURED - Low relapse rate] BOTTOM SECTION - Leprosy Reactions (separate colored box, yellow background): Title: "Acute Reactions During/After Treatment" TWO COLUMNS: LEFT: TYPE 1 - REVERSAL REACTION - Borderline types (BT/BB/BL) - Sudden increase in CMI - Swelling/tenderness of lesions - New nerve damage - Treatment: PREDNISOLONE RIGHT: TYPE 2 - ENL (Erythema Nodosum Leprosum) - BL and LL types - Immune complex mediated - Tender red nodules + fever - Arthralgia, iridocyclitis - Treatment: THALIDOMIDE / Prednisolone Clean arrow design, color-coded boxes
Flowchart 1 - Pathogenesis & Classification (Ridley-Jopling Spectrum)
Flowchart 2 - Diagnosis Flowchart
Flowchart 3 - WHO MDT Treatment & Reactions
Quick Summary Table for Exam
| Feature | Tuberculoid (TT) | Lepromatous (LL) |
|---|---|---|
| Immunity | Strong | Absent |
| Bacilli | Few | Abundant (globi) |
| Skin lesions | Few, well-defined | Many, diffuse |
| Nerve damage | Severe, early | Mild, late |
| Lepromin test | Positive | Negative |
| Infectivity | Low | High |
| Treatment | PB regimen (6m) | MB regimen (12m) |