Pemphigus vulgaris
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pemphigus vulgaris"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative dermatology textbooks. Here is the full review:
Pemphigus Vulgaris
Pemphigus vulgaris (PV) is the most common and most severe form of pemphigus - a group of organ-specific autoimmune blistering diseases affecting skin and mucous membranes, characterized by intraepidermal blistering due to acantholysis.
Pathogenesis
PV is caused by IgG autoantibodies directed against desmoglein 3 (Dsg3), a desmosomal transmembrane cadherin adhesion molecule. Dsmogleins are components of desmosomes, the intercellular adhesion junctions that hold keratinocytes together. Anti-Dsg3 antibodies disrupt desmosomal adhesion, causing acantholysis (separation of epidermal cells from each other) and blister formation.
- Mucosal-dominant PV: antibodies to Dsg3 alone (mucosal erosions, minimal skin disease - because Dsg1 compensates on the skin but mucosa lacks Dsg1)
- Mucocutaneous PV: antibodies to both Dsg1 and Dsg3 (extensive skin blistering in addition to mucosal erosions)
This "desmoglein compensation theory" explains why Dsg3-only antibodies preferentially produce oral lesions: in skin, Dsg1 can compensate for loss of Dsg3 function, but in mucosa, which lacks Dsg1, no such compensation occurs. When both dsmogleins are targeted, widespread skin and mucosal disease results.
(Fitzpatrick's Dermatology, Vol. 1-2; Dermatology 2-Volume Set 5e)
Epidemiology
- Affects men and women equally
- Most common in the 5th and 6th decades of life; rare in children
- Higher incidence in Ashkenazi Jewish populations and those of Mediterranean descent (Middle East, North Africa, South Asia)
- In Turkey, Saudi Arabia, Tunisia, and Iran, mean age of onset ~40 years; in the US and Europe, 50-70 years
- Before corticosteroids, PV was frequently fatal within 2-5 years; today patients more often suffer from treatment-related morbidity
Clinical Features
PV is divided into two subtypes:
| Feature | Mucosal-Dominant PV | Mucocutaneous PV |
|---|---|---|
| Antibodies | Anti-Dsg3 only | Anti-Dsg3 + Anti-Dsg1 |
| Oral lesions | Always present | Always present |
| Skin lesions | Absent/minimal | Extensive |
Mucosal Lesions
- Oral mucosa is involved in virtually all cases (~60% present here first
- Painful erosions on buccal and palatine mucosae; intact blisters are rare (too fragile)
- Erosions have an irregular, ill-defined border; may cause decreased oral intake
- Extension onto the vermilion lip produces thick, fissured hemorrhagic crusts
- Throat involvement: hoarseness, dysphagia
- Esophageal involvement: "esophagitis dissecans superficialis" (sloughing of the entire esophageal lining as a cast) - can occur even when skin disease is controlled, because mucosa lacks Dsg1
- Other mucosae affected: conjunctivae, nasal mucosa, vagina, labia, penis, anus
Cutaneous Lesions
- Primary lesion: flaccid, thin-walled blisters on normal-appearing or erythematous skin
- Blisters arise anywhere except palms and soles
- Fluid initially clear, may become hemorrhagic, turbid, or seropurulent
- Blisters rupture easily into painful, oozing erosions that spread peripherally and attain large size
- Erosions may become generalized (as in image below)
- Healing leaves post-inflammatory hyperpigmentation without scarring
- Some lesions develop papillomatosis and crusting ("vegetating lesions"), especially in intertriginous areas (pemphigus vegetans variant - generally better prognosis)


Clinical Signs
| Sign | Description |
|---|---|
| Nikolsky sign | Lateral pressure on skin slides the epidermis away from dermis; also elicited by rubbing apparently normal skin distant from lesions |
| Asboe-Hansen sign (Nikolsky II / bulla-spread phenomenon) | Gentle pressure on an intact bulla spreads the fluid laterally under adjacent skin |
Both signs reflect loss of intraepidermal cohesion. Note: Nikolsky sign is not specific to PV - also positive in SSSS, SJS, and TEN.
Diagnosis
Histopathology (H&E)
- Suprabasal acantholysis: loss of cohesion above the basal layer, with basal cells remaining attached to the basement membrane ("tombstone" appearance)
- Blister cavity contains few inflammatory cells (mainly eosinophils)
- Dermal perivascular mononuclear infiltrate with eosinophils
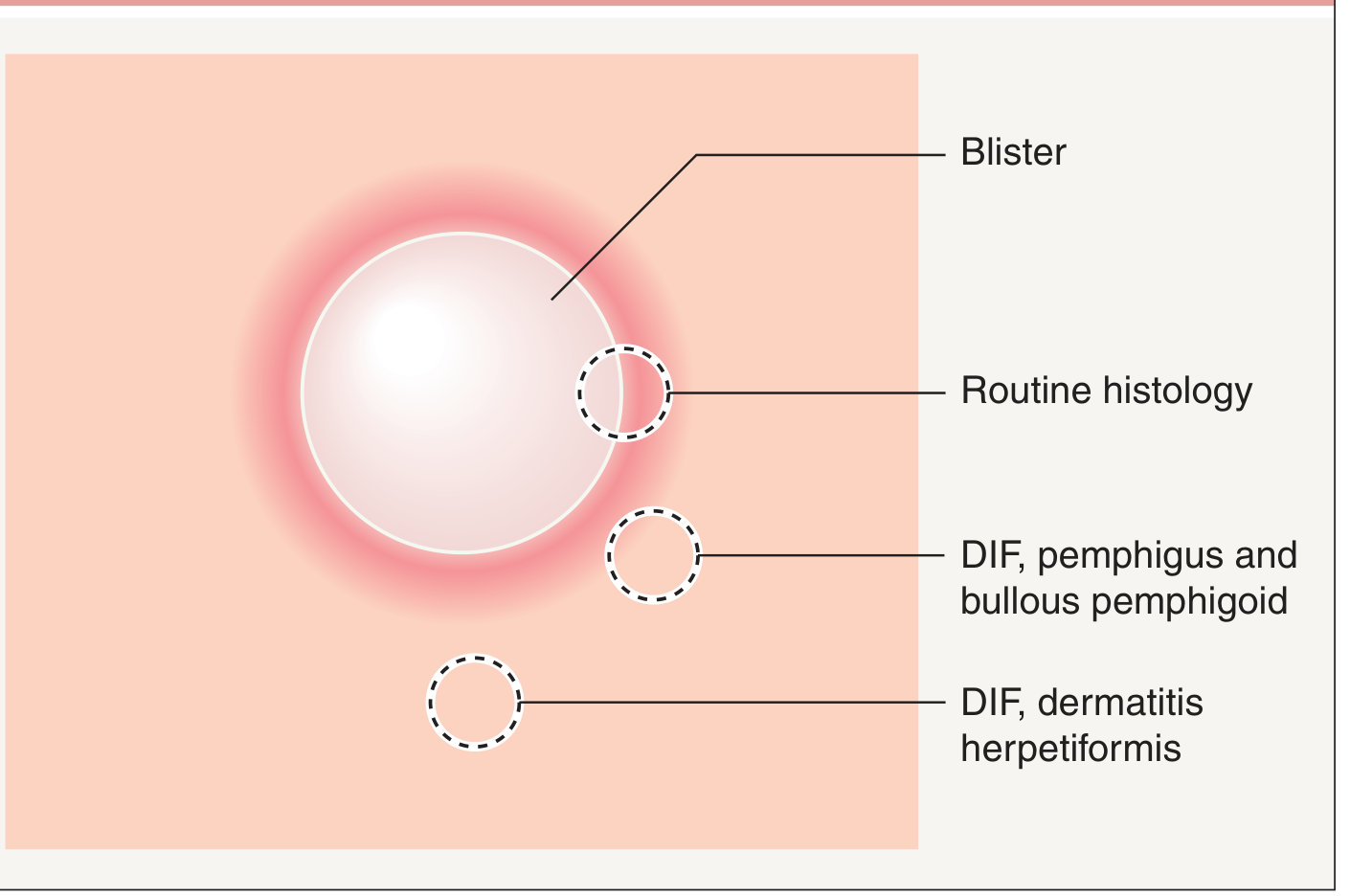
- Biopsy site: edge of a fresh vesicle/bulla plus the inflammatory rim
Immunofluorescence
- Direct immunofluorescence (DIF) on perilesional skin: IgG (and often C3) deposits in a net-like/chicken-wire pattern on the surface of keratinocytes throughout the epidermis (intercellular pattern)
- Indirect immunofluorescence (IIF) on serum: circulating IgG anti-cell surface antibodies; best substrate is monkey esophagus
ELISA
- Anti-Dsg3 antibodies (present in all PV)
- Anti-Dsg1 antibodies (present in mucocutaneous subtype; levels correlate with disease activity)
Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|---|
| Bullous pemphigoid | Subepidermal blisters; tense (not flaccid) blisters; Nikolsky negative; anti-BP180/BP230 |
| Pemphigus foliaceus | Subcorneal acantholysis; no mucosal involvement; anti-Dsg1 only |
| Paraneoplastic pemphigus | Associated malignancy; polymorphic lesions; anti-envoplakin/periplakin |
| Stevens-Johnson syndrome | History of drug/infection trigger; target lesions; epidermal necrolysis |
| Mucous membrane pemphigoid | Scarring mucosal lesions; subepithelial blisters; anti-BP180/laminin-332 |
| Herpetic stomatitis | Grouped vesicles; HSV positive; no skin blisters |
| Erythema multiforme | Target lesions; acral distribution |
Treatment
Standard First-Line
Oral prednisone (1 mg/kg/day, typically 60 mg/day) is the initial treatment. Since 2017, rituximab (anti-CD20 monoclonal antibody) has emerged as a major advance and is increasingly used as first-line alongside or instead of high-dose steroids based on the Ritux 3 trial (Joly et al., Lancet 2017), which showed rituximab + short-term prednisone was superior to prednisone alone.
- Rituximab: 375 mg/m² once weekly x 4 weeks, or 1 g initially then at 2 weeks (may need repeating every 3-6 months)
Adjuvant/Steroid-Sparing Agents (combined with prednisone)
| Drug | Dose |
|---|---|
| Azathioprine | 2-4 mg/kg/day (usually 100-300 mg/day) |
| Mycophenolate mofetil | 2-3 g/day |
| Cyclophosphamide | 1-3 mg/kg/day |
| Cyclosporine | 3-5 mg/kg/day |
| Methotrexate | 7.5-20 mg/week |
Refractory/Severe Disease
- Pulse methylprednisolone: 1 g/day IV x 3-5 days
- Pulse cyclophosphamide: 500-1000 mg/m² every 4 weeks
- IVIg (intravenous immunoglobulin): 400 mg/kg/day x 5 days (may repeat monthly)
- Plasmapheresis: 1-2 times/week at onset (rapid removal of circulating antibodies)
- Extracorporeal photopheresis
Topical
- Superpotent topical corticosteroids (e.g., clobetasol) for limited lesions
- Topical tacrolimus for oral erosions
(Dermatology 2-Volume Set 5e; Andrews' Diseases of the Skin)
Monitoring Disease Activity
Several validated scoring tools are used in clinical trials:
- ABSIS (Autoimmune Bullous Skin Disorder Intensity Score)
- PVAS (Pemphigus Vulgaris Activity Score)
- PDAI (Pemphigus Disease Area Index)
Anti-Dsg antibody titers (by ELISA) generally correlate with disease activity and can be used to monitor treatment response and predict relapse.
Prognosis
- Before corticosteroids: usually fatal within 2-5 years (large skin barrier loss → fluid loss, electrolyte imbalance, sepsis)
- With modern treatment: prognosis greatly improved, but morbidity from immunosuppression (infections, osteoporosis, Cushing's syndrome, diabetes) remains significant
- Widespread cutaneous disease can still be fatal from sepsis or fluid/electrolyte imbalance without appropriate treatment
- Mucosal-dominant subtype has a generally milder course
Sources: Fitzpatrick's Dermatology Vol. 1-2; Dermatology 2-Volume Set 5e (Bolognia et al.); Andrews' Diseases of the Skin (Clinical Dermatology)
This is a shared conversation. Sign in to Orris to start your own chat.