History and Examiation of Oropharynx Diseases + including use of a tongue depressor
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have excellent content from multiple authoritative sources. Let me compile the comprehensive answer.
History and Examination of Oropharynx Diseases
Anatomy of the Oropharynx (Overview)
The oropharynx extends from the soft palate superiorly to the level of the hyoid bone inferiorly. It includes four key subsites:
- Posterior pharyngeal wall
- Soft palate and uvula
- Palatine tonsils and tonsillar pillars (palatoglossal and palatopharyngeal folds)
- Base of tongue (posterior one-third) - including lingual tonsils and valleculae
The oropharynx is part of Waldeyer's ring of lymphoid tissue, comprising the nasopharyngeal (adenoid), tubal, palatine, and lingual tonsils.
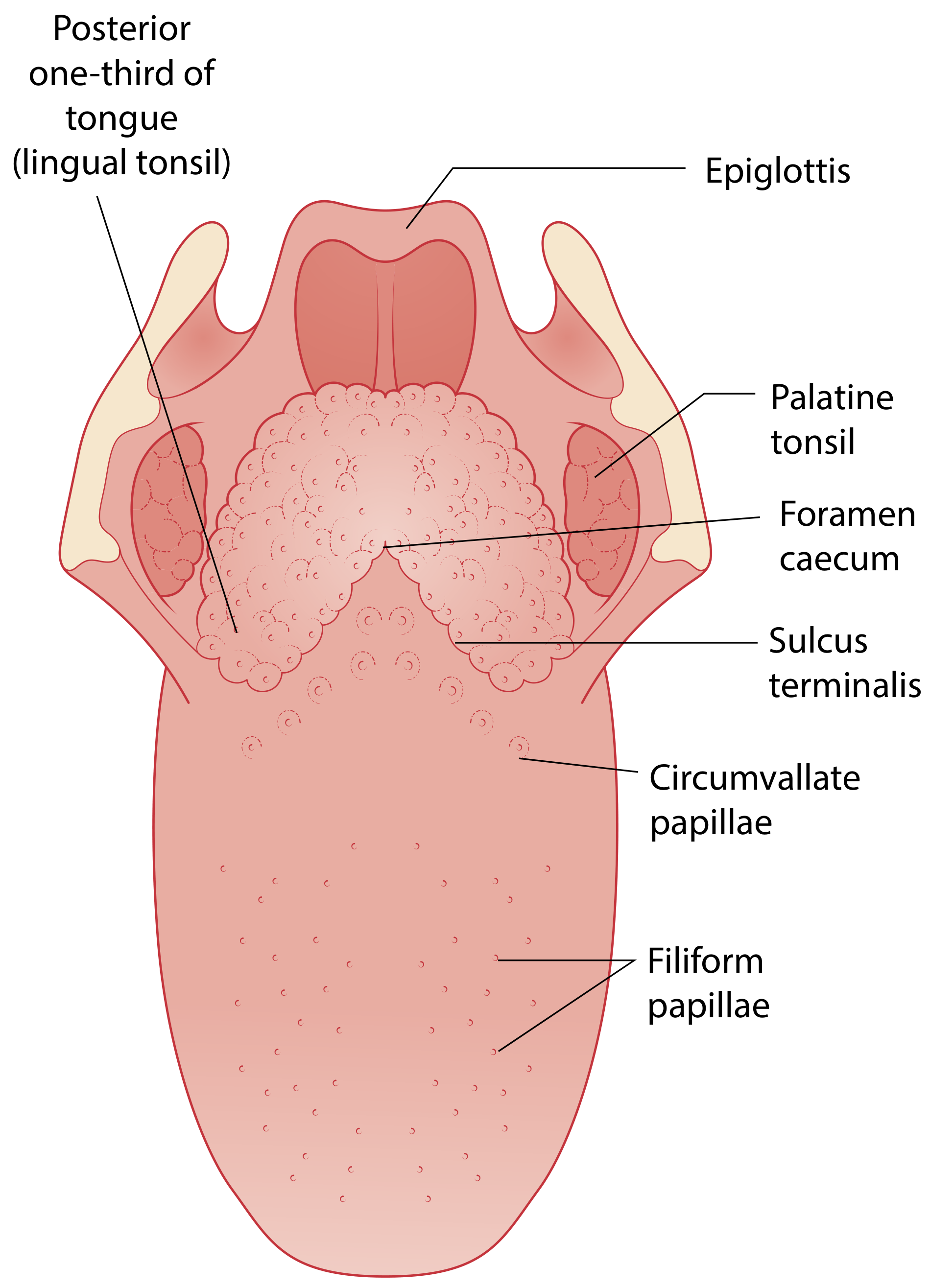
Anatomy of the tongue. The posterior third belongs to the oropharynx. - Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Nerve supply: The valleculae and tongue base are innervated by the internal laryngeal nerve (branch of vagus). The remainder of the oropharyngeal mucosa is supplied predominantly by the glossopharyngeal nerve (CN IX) and to a lesser degree the lesser palatine nerve.
Taking a History in Oropharyngeal Disease
A thorough history should cover the following areas:
Presenting Symptoms
| Symptom | Significance |
|---|---|
| Sore throat / odynophagia | Infection (pharyngitis, tonsillitis, peritonsillar abscess), malignancy |
| Dysphagia | Progressive dysphagia suggests malignancy; sudden onset suggests abscess/foreign body |
| Trismus (difficulty opening mouth) | Peritonsillar abscess (PTA), masticator space infection |
| Voice change | "Hot potato" muffled voice = PTA; hoarseness = laryngopharyngeal involvement |
| Otalgia (referred ear pain) | Via Jacobson's nerve (CN IX) - important red flag for malignancy |
| Neck mass | Lymphadenopathy - infection vs. metastatic disease |
| Snoring / sleep apnoea | Tonsillar hypertrophy, soft palate pathology |
| Weight loss / anorexia | Red flag for malignancy |
| Regurgitation of food | Pharyngeal pouch (Zenker's diverticulum) |
Red Flags in the History
- Unilateral sore throat with localized pain to one side
- Unilateral otalgia (unexplained referred ear pain)
- Progressive dysphagia
- Weight loss
- Hoarseness persisting > 3 weeks
- Neck lump
Aetiological History
- Smoking and alcohol (major risk factors for oropharyngeal carcinoma)
- HPV exposure (sexual history - HPV-associated oropharyngeal SCC is rising)
- Immunocompromised status (HIV, chemotherapy - risk of oral candidiasis, viral infections)
- Recurrent tonsillitis (relevant for PTA and tonsillectomy decisions)
- Drug history (some medications cause lichenoid reactions, mucosal ulceration)
- Occupational/industrial irritant exposure
- Post-nasal drip, acid reflux (causes of chronic pharyngitis)
- Dental hygiene
"Exclusion of malignancy is the most important aspect of managing these patients. This requires a careful history, in particular enquiring about localized pain to one side and earache, progressive dysphagia or weight loss." - Scott-Brown's Otorhinolaryngology
Clinical Examination of the Oropharynx
Equipment Required
- Good light source (headlight or hand-held torch)
- Tongue depressor (wooden or metal Lack's tongue depressor)
- Gloves for palpation
- Nasendoscope (for complete assessment when indicated)
Use of the Tongue Depressor
The tongue depressor is the most basic and essential instrument for oropharyngeal examination. Technique:
- Position the patient: Seated upright, facing the examiner, with the mouth wide open and head slightly extended.
- Ask the patient to say "aah" - this elevates the soft palate and opens the oropharynx.
- Place the tongue depressor on the anterior two-thirds of the tongue (not the posterior third, which triggers the gag reflex). Press firmly downward and slightly forward to depress the tongue.
- Illuminate the oropharynx using a light source aimed directly into the mouth.
- Systematic inspection follows (see below).
- Test palatal movement: Ask the patient to say "aah" while the depressor is in place - observe symmetrical palate elevation.
- Test gag reflex if indicated: touching the posterior pharyngeal wall or tonsillar pillars.
A metal (Lack) tongue depressor is also used for nasal patency testing: "Nasal airflow and patency should be subjectively assessed... using the palmar surface of the thumb or a shiny Lack tongue depressor." - Scott-Brown's Otorhinolaryngology
Caution: Avoid pressing on the posterior third of the tongue - this provokes the gag reflex. In patients with trismus (e.g., peritonsillar abscess), forced mouth opening is difficult and forceful instrumentation should be avoided.
Systematic Inspection (What to Look For)
1. Lips and Oral Commissures
- Ulcers, angular cheilitis, herpes labialis, leukoplakia
2. Oral Cavity Proper (before oropharynx)
- Teeth and gums: caries, gingivitis
- Buccal mucosa: ulcers, white patches (leukoplakia, candidiasis), lichenoid lesions
- Hard palate: torus palatinus, ulceration
- Floor of mouth: Wharton's duct openings either side of the frenulum; check for ranulae, sublingual masses, and lymphadenopathy
- Tongue (anterior two-thirds): coating, ulcers, atrophy of papillae (iron/B12 deficiency), leukoplakia, macroglossia
3. Soft Palate and Uvula
- Symmetry and movement on phonation ("aah")
- Deviation of uvula away from the side of a peritonsillar abscess
- Bifid uvula (submucosal cleft palate)
- Petechiae (infectious mononucleosis)
4. Palatine Tonsils
- Size (graded I-IV: Grade I = tonsil within pillars; Grade IV = "kissing tonsils")
- Surface: smooth vs. cryptic, exudate, membrane (mononucleosis, diphtheria)
- Symmetry: asymmetric tonsils are a red flag - may indicate deep space infection or malignancy
- Colour: erythema, tonsillar pillar oedema
- Peritonsillar region: swelling, fullness in the soft palate and anterior pillar area suggests PTA
"True asymmetry [of the palatine tonsils] is uncommon and should raise concerns about potential malignancy or parapharyngeal masses pushing the tonsil medially." - Scott-Brown's Otorhinolaryngology
5. Posterior Pharyngeal Wall
- Granular lymphoid tissue (lymphoid follicles = chronic pharyngitis - "cobblestoning")
- Posterior pharyngeal abscess (bulge, tracking pus)
- Lateral pharyngeal bands: prominent in chronic pharyngitis
- Post-nasal drip: mucus streaming down the posterior wall
6. Tongue Base (Posterior Third)
- Assess by pressing the tongue depressor more firmly or asking the patient to protrude the tongue
- Lingual tonsil hypertrophy
- Valleculae - best seen with nasendoscopy
Neurological Examination Component (Cummings Otolaryngology)
When neurological dysfunction is suspected, a structured examination includes:
| Test | What it assesses |
|---|---|
| Observe tongue at rest | Fasciculations (ALS), athetoid movement (tardive dyskinesia), tongue thrusting (oromandibular dystonia) |
| "Protrude tongue and move side to side" | CN XII (hypoglossal) integrity |
| Say "aah" | Palatal symmetry - CN IX/X (glossopharyngeal/vagus) |
| Rapid /pa/ repetition | Lip function (CN VII) |
| Rapid /ta/ repetition | Tongue tip (CN XII) |
| Rapid /ga/ repetition | Posterior tongue (CN X) |
| Push tongue against cheek | Tongue strength |
"Ask the patient to purse the lips, to protrude the tongue and move it from side to side, and to open the mouth and say the traditional 'aah' to test for palate motion and symmetry." - Cummings Otolaryngology
Palpation
After inspection, bimanual palpation of the tongue and floor of mouth is essential:
- Bimanual palpation: one gloved finger inside the mouth, one hand on the external neck
- Palpate the tongue base (submucous lesions may not be visible)
- Assess for induration (suggests malignancy)
- Palpate the tonsillar fossae gently
Cervical lymph nodes must always be examined systematically (levels I-VI) - critical for staging and detecting metastatic disease.
Key Oropharyngeal Diseases and Their Clinical Features
1. Acute Pharyngitis / Tonsillitis
- Sore throat, fever, dysphagia
- Bilateral tonsillar erythema and oedema, exudate (bacterial - Group A Strep or viral - EBV)
- Symmetric uvula (contrast with PTA)
- Cervical lymphadenopathy
2. Peritonsillar Abscess (Quinsy)
- Most common deep neck space infection in patients > 6 years
- Trismus, "hot potato" muffled voice, unilateral severe odynophagia, high fever
- Uvula deviated away from the abscess side
- Asymmetric swelling of the anterior pillar and soft palate
- Internal carotid artery lies ~2.5 cm posterolateral to the tonsil - important during drainage
- Treatment: needle aspiration, incision and drainage, or quinsy tonsillectomy + antibiotics
3. Infectious Mononucleosis (EBV)
- Pharyngotonsillar exudate, soft palate petechiae, splenomegaly, lymphadenopathy
- Grey-white membrane over tonsils
4. Oral Candidiasis
- White curd-like pseudomembrane over tongue, buccal mucosa, palate, oropharynx
- Can be scraped off with a tongue depressor (distinguishes from leukoplakia)
- Common in immunocompromised patients
5. Herpangina
- Self-limiting vesicular eruption confined to the oropharynx (distinguishes it from herpes simplex type 1)
- Caused by enteroviruses (30, 71) and coxsackievirus group A
6. Hand, Foot and Mouth Disease
- Vesicular eruption of oral cavity AND oropharynx with vesicles on hands and feet
- Caused by enterovirus 71, coxsackieviruses; mainly affects young children
7. Chronic Non-Specific Pharyngitis
- Long-standing throat discomfort, often little on examination apart from lymphoid tissue hypertrophy and lateral pharyngeal bands
- Causes: smoking, acid reflux, post-nasal drip, occupational irritants, stress
- Exclude malignancy: this is the most important step
8. Oropharyngeal Carcinoma
- SCC accounts for ~90% of oropharyngeal carcinomas
- HPV-positive carcinomas are rising (base of tongue, tonsils)
- Red flags: unilateral sore throat, referred otalgia, progressive dysphagia, neck mass, weight loss
- True tonsillar asymmetry must be biopsied
9. Syphilis
- Primary: painless chancre at lips, tongue, buccal mucosa, tonsil
- Secondary: fever, pharyngeal hyperaemia, mucocutaneous rash, generalized lymphadenopathy, oropharyngeal lesions
- "The great pretender" - consider in atypical oral/oropharyngeal ulceration
Summary: Examination Protocol
1. History (symptoms, red flags, risk factors)
2. Equipment: light source + tongue depressor
3. Inspect: lips → teeth/gums → buccal mucosa → hard palate → floor of mouth
4. Tongue depressor on anterior 2/3 tongue → inspect oropharynx:
- Soft palate symmetry (say "aah")
- Uvula position
- Palatine tonsils (size, surface, symmetry, colour, exudate)
- Posterior pharyngeal wall (cobblestoning, pus, drip)
5. Neurological: tongue protrusion, diadochokinesis (/pa/, /ta/, /ga/)
6. Palpation: tongue, floor of mouth, tonsils, bimanually
7. Neck: systematic lymph node examination (levels I-VI)
8. If needed: flexible nasendoscopy for tongue base and hypopharynx
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery (9781138094642)
- Cummings Otolaryngology Head and Neck Surgery (9780323612173)
- Roberts and Hedges' Clinical Procedures in Emergency Medicine (9780323354783)
- K.J. Lee's Essential Otolaryngology (9781260122237)
This is a shared conversation. Sign in to Orris to start your own chat.