5H and 5Ts in hypotension Mayocardial infraction etc
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive textbook content. Here is the full answer:
The 5 H's and 5 T's - Reversible Causes of Cardiac Arrest / Hypotension
The 5 H's and 5 T's are a mnemonic taught in ACLS to rapidly identify and correct treatable causes of cardiac arrest (especially PEA/asystole) and hemodynamic instability. Every resuscitation should include a systematic search for these.
The 5 H's
| Cause | Key Clues | Treatment |
|---|---|---|
| Hypovolemia / Hemorrhage | Blood/fluid loss, FAST positive, GI bleeding | IV fluids, blood products, hemostasis |
| Hypoxia | Incorrect airway placement, misplaced ETT, low SpO2 | Verify airway position, oxygenation, assisted ventilation |
| Hydrogen ion (Acidosis) | Prolonged arrest, poor CPR quality, ABG showing low pH | Hyperventilation, NaHCO3 1-1.5 mEq/kg for severe cases, optimize CPR |
| Hypo/Hyperkalemia | Renal failure, dialysis patient, AV fistula, ECG changes | Hyperkalemia: CaCl2, NaHCO3, insulin/glucose; Hypokalemia: IV KCl replacement |
| Hypothermia | Low core temperature (rectal temp), cold exposure | Warm blankets, warm IV fluids, peritoneal/thoracic lavage, VA-ECMO |
Note on Acidosis: Sodium bicarbonate is NOT routinely given - current evidence does not support routine use. It is only considered for severe, prolonged metabolic acidosis. Giving it increases CO2 production, so ventilation must be increased.
The 5 T's
| Cause | Key Clues | Treatment |
|---|---|---|
| Tablets (Drug Overdose) | History of ingestion, wide QRS (TCA), bradycardia (beta-blocker) | TCA: IV NaHCO3; beta-blocker/CCB: high-dose insulin + lipid emulsion; Local anesthetic: lipid emulsion |
| Cardiac Tamponade | Jugular venous distension, muffled heart sounds, JVD, bedside echo (fluid around heart) | Pericardiocentesis (emergent); thoracotomy/pericardiotomy (definitive) |
| Tension Pneumothorax | Unequal breath sounds, tracheal deviation, worsening after intubation | Immediate needle thoracostomy, then tube thoracostomy |
| Coronary Thrombosis (Acute MI) | Ischemic ECG changes, STEMI, hyperdynamic LV on echo | PCI, thrombolytics if PCI unavailable (especially in peri-arrest STEMI) |
| Thrombosis (Pulmonary Embolism) | Risk factors for DVT/PE, right heart strain on echo, massive PE | Thrombolytics (tPA), VA-ECMO bridge, surgical embolectomy |
PEA Management Algorithm
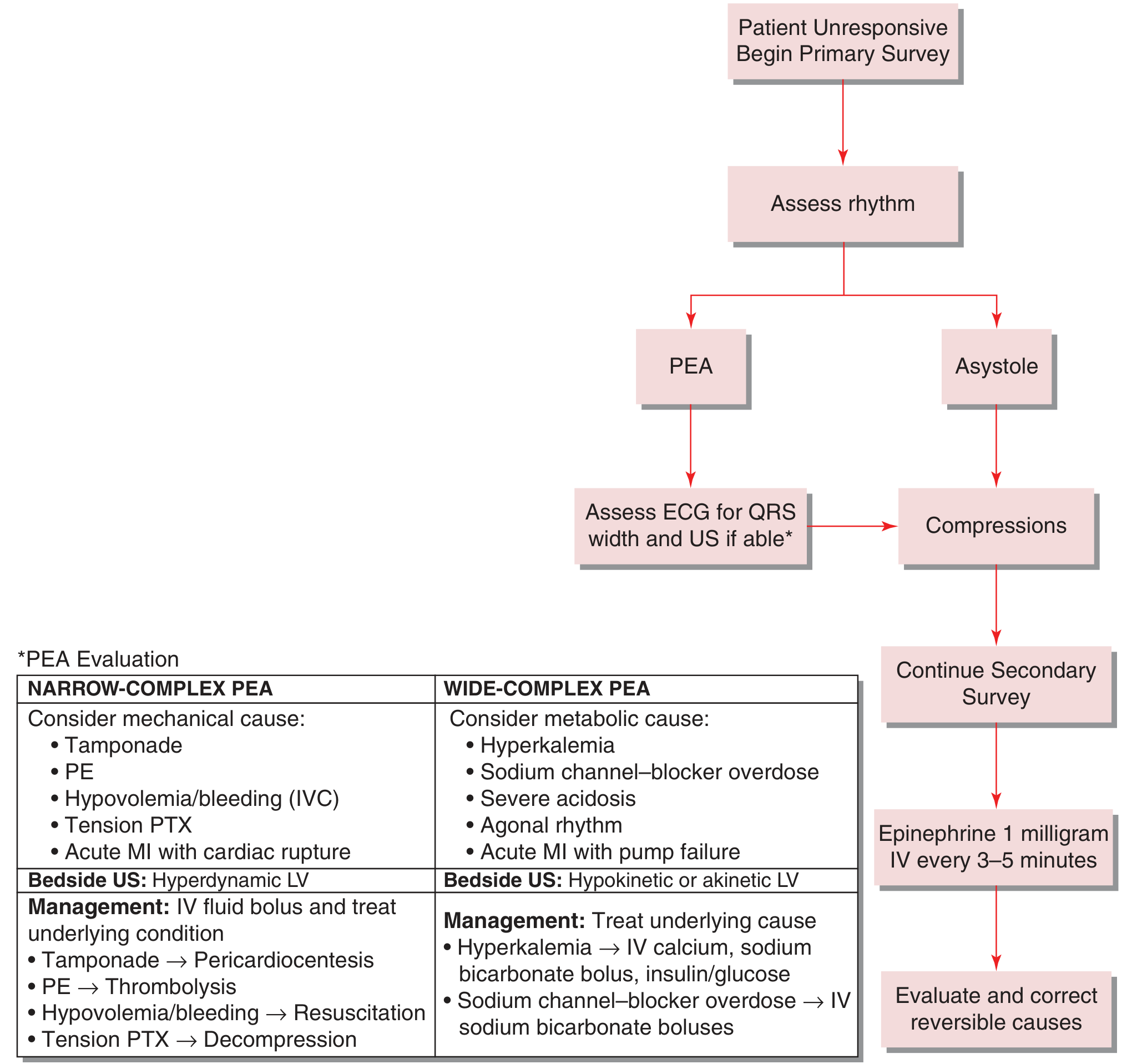
From Tintinalli's Emergency Medicine - PEA/Asystole management algorithm
A key bedside skill is using QRS width on ECG + point-of-care ultrasound to narrow your differential:
- Narrow-complex PEA - think mechanical causes: tamponade, PE, hypovolemia/bleeding (collapsed IVC), tension pneumothorax, acute MI with cardiac rupture. Echo shows a hyperdynamic LV.
- Wide-complex PEA - think metabolic causes: hyperkalemia, sodium channel-blocker overdose, severe acidosis, acute MI with pump failure. Echo shows a hypokinetic/akinetic LV.
Myocardial Infarction as a Cause of Hypotension - Cardiogenic Shock
Acute MI is one of the most common reversible causes of cardiac arrest and is a major cause of cardiogenic shock. The key points:
Recognition
Patients present with hypotension, weak/rapid pulse, tachypnea, cool and clammy skin. Look for ST changes, Q waves, or new LBBB on ECG.
Management of Cardiogenic Shock from MI
1. Vasopressors (to maintain perfusion pressure)
- Norepinephrine (0.02-1.0 mcg/kg/min) - preferred first-line. Acts mainly as a vasoconstrictor with mild inotropy, increases coronary flow, and is superior to dopamine.
- Dopamine (inotrope at 3-10 mcg/kg/min; vasopressor at 10-20 mcg/kg/min) - second line; associated with more arrhythmias.
- Epinephrine (0.05-2 mcg/kg/min) - associated with more refractory shock and metabolic derangement vs. norepinephrine.
- Vasopressin (0.02-0.04 U/min) - for catecholamine-refractory shock.
2. Inotropes (if tissue perfusion inadequate despite vasopressors)
- Dobutamine (2.5-20 mcg/kg/min) - selective beta-1 agonist, improves contractility. First choice if SBP >90 mmHg, but may worsen hypotension.
- Milrinone (0.125-0.75 mcg/kg/min, no loading dose) - PDE inhibitor, fewer arrhythmias, long half-life, can cause hypotension. Equivalent to dobutamine in cardiogenic shock.
3. Revascularization - the cornerstone of therapy
- Rapid PCI is the only intervention consistently proven to reduce mortality in cardiogenic shock from MI.
- Best outcomes when PCI is within 6 hours of symptom onset, but benefit extends up to 18 hours after shock onset.
- In multivessel disease: stent the culprit lesion only (not immediate multivessel PCI).
- Thrombolytics can be used if PCI is not available.
4. Mechanical support
- IABP (Intra-aortic balloon pump): reduces afterload and augments diastolic pressure. Despite hemodynamic rationale, randomized trials show no mortality benefit with IABP in cardiogenic shock with early revascularization.
- LVAD/ECMO: for patients refractory to IABP and vasopressors.
Special consideration: Right Ventricular Infarction
RV infarction is an important cause of hypotension after MI that is easily missed. It causes hypotension in the absence of left heart failure. Treatment differs - these patients are preload dependent; give IV fluids, avoid diuretics and vasodilators. This is why nitroglycerin can precipitate severe hypotension in RV infarction.
Sources:
- Tintinalli's Emergency Medicine, Differential Diagnoses of Cardiac Arrest chapter
- Rosen's Emergency Medicine, Pulseless Electrical Activity chapter
- Goldman-Cecil Medicine, Cardiogenic Shock Complicating Acute MI chapter
- Fuster and Hurst's The Heart, 15th Ed., ACLS algorithm chapter
This is a shared conversation. Sign in to Orris to start your own chat.