Adult and children dose of phenetoin
Reading File
Finding Sources
Searching the Web
phenytoin adult pediatric dosing loading maintenance 2024
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Now I have comprehensive data from the Harriet Lane Handbook, FDA labeling, and the Family Medicine textbook. Here is the full, detailed answer:
Phenytoin Dosing
ADULTS
Status Epilepticus (IV)
| Parameter | Dose |
|---|---|
| Loading dose | 10-20 mg/kg IV (usual 15-20 mg/kg) |
| Max infusion rate | 50 mg/min (slower if elderly or cardiac risk) |
| Maintenance dose | 100 mg IV/oral every 6-8 hours |
Non-emergent Loading & Maintenance (IV/Oral)
| Parameter | Dose |
|---|---|
| Loading dose (oral, hospitalized) | 1000 mg divided as 400 mg, then 300 mg, then 300 mg q2h |
| Loading dose (IV) | 10-15 mg/kg IV at max 50 mg/min |
| Maintenance (oral capsules) | 100 mg 3 times daily (300 mg/day) or 300 mg once daily |
| Maintenance (IV) | 100 mg IV every 6-8 hours |
| Range | 200-500 mg/day, adjusted by levels |
Oral Maintenance by Weight
- 4-7 mg/kg/day in 1-3 divided doses (adjusted to therapeutic level)
CHILDREN (Pediatric)
Status Epilepticus (IV)
| Age | Loading Dose | Max Infusion Rate |
|---|---|---|
| All pediatric ages | 15-20 mg/kg IV | 1-3 mg/kg/min or 50 mg/min (whichever is slower) |
Maintenance Dose (Oral or IV)
| Age Group | Dose |
|---|---|
| Neonates | 5 mg/kg/day divided q12h |
| Infants/Children < 6 years | 5 mg/kg/day in 2-3 divided doses (max 300 mg/day) |
| Children > 6 years | 7.5-9 mg/kg/day in 2-3 divided doses |
| Adolescents | 300 mg/day (same as adult) |
Children generally require higher mg/kg doses than adults due to faster hepatic metabolism.
NEONATAL DOSING (from Harriet Lane Handbook)
- Loading dose: 15-20 mg/kg IV
- Maintenance: 5 mg/kg/day divided every 12 hours
- Rate: not to exceed 1-3 mg/kg/min
Therapeutic Drug Monitoring
| Level | Target |
|---|---|
| Total phenytoin | 10-20 mcg/mL (mg/L) |
| Free (unbound) phenytoin | 1-2 mcg/mL |
Monitor free levels in: hypoalbuminemia, renal failure, pregnancy, elderly patients (reduced protein binding)
Key Practical Points
- Non-linear (Michaelis-Menten) kinetics: Small dose increases near the therapeutic range can cause disproportionately large rises in serum levels - dose changes should be small (25-50 mg increments)
- IV rate warning: Rapid IV infusion causes hypotension, bradycardia, and cardiac arrhythmias - always monitor ECG and BP
- IM route: NOT recommended (painful, erratic absorption, crystal precipitation)
- Oral bioavailability: Capsules (sodium salt) and tablets/suspension (acid form) are NOT interchangeable mg-for-mg - 100 mg capsule ≈ 92 mg free acid
- Drug interactions: Numerous - enzyme inducer (CYP2C9, CYP3A4); levels altered by carbamazepine, valproate, fluconazole, and many others
- Fosphenytoin (prodrug): Dosed in phenytoin sodium equivalents (PE); can be given faster IV (150 mg PE/min in adults) and can be given IM
Sources
- The Harriet Lane Handbook, 23rd ed., p. 1888-1904 (pediatric/neonatal dosing)
- Textbook of Family Medicine, 9th ed., Table 41-12
- FDA Dilantin Label
- Drugs.com Phenytoin Dosage Guide (reviewed Mar 2026)
Status epilepticus
Finding Sources
Searching the Web
status epilepticus management guidelines 2024 2025
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete, evidence-based overview of Status Epilepticus:
Status Epilepticus
Definition
A seizure lasting ≥5 minutes OR two or more seizures without recovery of consciousness between them. After 5 minutes, seizures are unlikely to self-terminate, are harder to control with antiepileptics, and begin causing neuronal damage. This is a neurological emergency - treatment should begin immediately.
After 20 minutes: hypotension, hypoxia, metabolic acidosis, hyperthermia, hypoglycemia, cardiac dysrhythmias, and pulmonary edema commonly develop.
Classification
| Type | Description |
|---|---|
| Convulsive SE | Tonic-clonic motor activity with altered consciousness |
| Nonconvulsive SE (NCSE) | Comatose or fluctuating mental status, no overt seizures - diagnosed by EEG |
| Refractory SE | Persists despite adequate doses of two antiepileptic agents (>60 min) |
| Super-refractory SE | Continues or recurs ≥24h after general anaesthetic agent initiation |
Common Causes
- Subtherapeutic antiepileptic drug levels (most common in known epileptics)
- Acute stroke or CNS injury
- Anoxia / hypoxia
- Metabolic abnormalities (hypoglycemia, hyponatremia, hypocalcemia)
- Alcohol or drug intoxication / withdrawal
- CNS infections (meningitis, encephalitis)
- Preexisting neurologic conditions
Immediate Stabilization (0-5 min)
- Airway: Position to maximize ventilation, prevent aspiration; nasopharyngeal airway if needed; consider intubation if prolonged
- Breathing: O2 by mask/nasal cannula; bag-valve-mask if inadequate ventilation
- Circulation: Large-bore IV access; cardiac monitor, pulse oximetry, BP monitoring
- Glucose: Bedside glucose immediately; give IV dextrose if hypoglycemic
- Labs: Electrolytes, calcium, magnesium, glucose, renal/liver function, CBC, toxicology screen, antiepileptic drug levels, pregnancy test (if applicable)
- Temperature: Monitor continuously; treat hyperthermia with cooling
- Do NOT perform LP during active SE; delay CT scan until seizures controlled
Treatment Algorithm
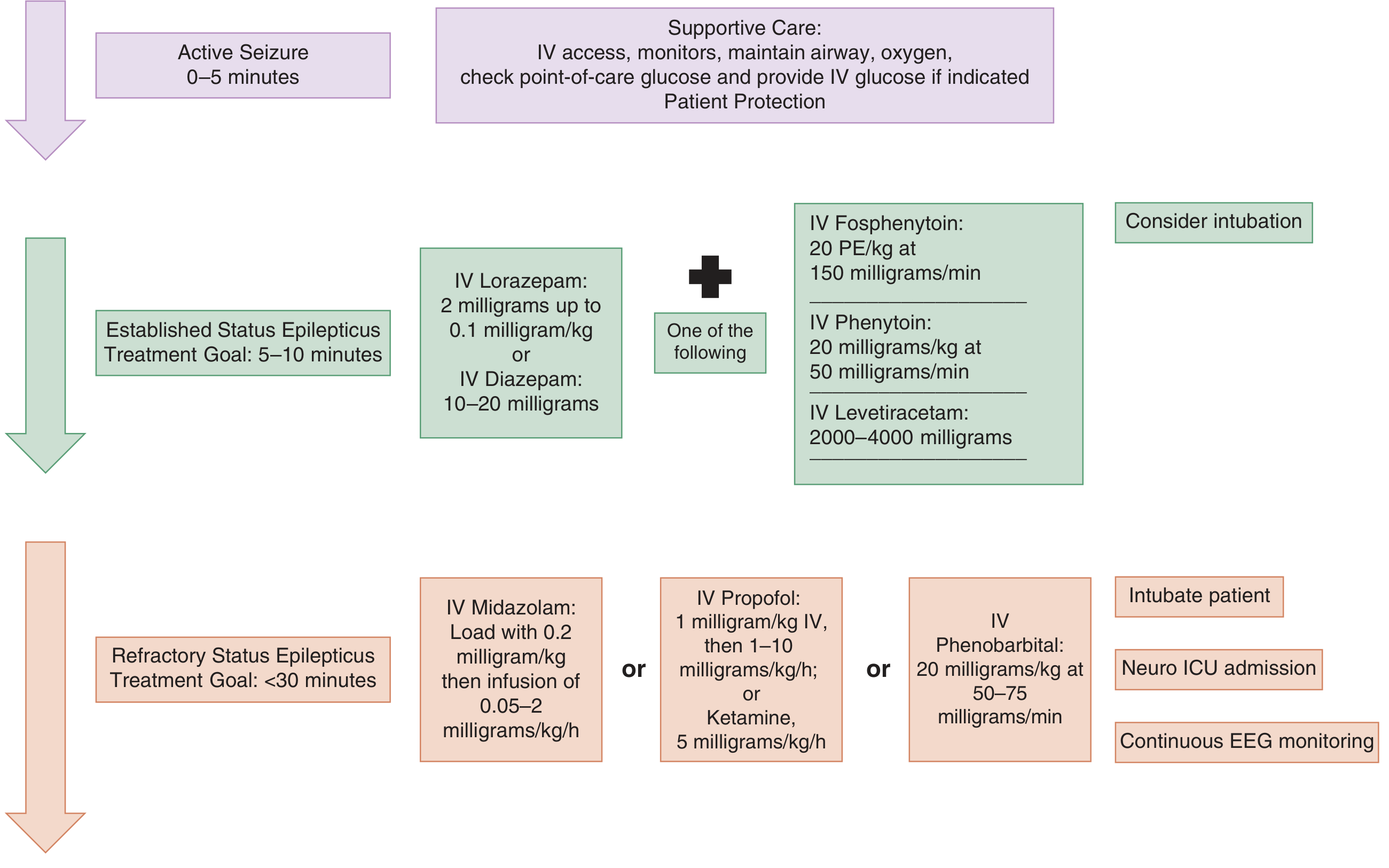
Phase 1 - First-Line: Benzodiazepines (0-10 min)
Terminate seizures 70% of the time. Give as early as possible - delays >10 min increase mortality, seizure duration, and complications.
| Drug | Adult Dose | Pediatric Dose | Route |
|---|---|---|---|
| Lorazepam (preferred if IV available) | 2-4 mg IV (0.1 mg/kg); repeat once in 5 min | 0.05-0.1 mg/kg IV | IV |
| Midazolam (preferred if no IV access) | 10 mg IM/IN | 0.2 mg/kg IM; 0.3 mg/kg IN | IM, IN, IV |
| Diazepam | 5-10 mg IV; repeat q5 min (max 30 mg) | 0.2-0.5 mg/kg IV (max 10 mg) or 0.5 mg/kg rectal | IV, rectal |
- Lorazepam: onset 3 min, duration 12-24 hours (preferred IV agent)
- Diazepam: onset 2 min, duration only 15-60 min (shorter - seizures may recur)
- IM midazolam = as effective as IV lorazepam in pre-hospital trials; preferred when no IV access
- Give second benzodiazepine dose only after 5 min of continued seizure activity after first dose
Phase 2 - Second-Line Antiepileptics (start within 20 min)
Start simultaneously with or immediately after benzodiazepines. No single agent is definitively superior.
| Drug | Adult Dose | Infusion Rate | Notes |
|---|---|---|---|
| Fosphenytoin (preferred over phenytoin) | 20 mg PE/kg IV | up to 150 mg PE/min | Can give IM; fewer cardiac/infusion side effects |
| Phenytoin | 20 mg/kg IV | max 50 mg/min (25 mg/min safer) | Not in glucose solutions; cardiac monitor mandatory |
| Levetiracetam | 20-60 mg/kg IV (typically 2000-4500 mg) | over 15 min | Fewest side effects, no interactions; rapidly gaining favor |
| Valproic acid | 20-40 mg/kg IV | 3-6 mg/kg/min | Contraindicated in liver disease, thrombocytopenia, suspected metabolic disease; not with phenytoin |
| Lacosamide | 200-400 mg IV | over 15 min | Alternative with limited data |
Phase 3 - Refractory SE: Anesthetic Infusions (<30-60 min target)
Requires intubation, Neuro ICU admission, and continuous EEG monitoring.
| Drug | Loading Dose | Infusion Rate |
|---|---|---|
| Midazolam | 0.2 mg/kg IV | 0.05-2 mg/kg/h, titrate to seizure cessation |
| Propofol | 1 mg/kg IV | 1-10 mg/kg/h (risk of propofol infusion syndrome at >40 mg/kg/h) |
| Phenobarbital | 20 mg/kg IV | 50-75 mg/min |
| Ketamine | - | 5 mg/kg/h infusion (emerging evidence) |
| Pentobarbital | 5-15 mg/kg | 0.5-5 mg/kg/h |
Pediatric-Specific Notes (Harriet Lane Handbook)
- Diazepam IV: Neonate: 0.1-0.3 mg/kg q15-30 min (max 2 mg); Child <5 yr: 0.2-0.5 mg/dose q2-5 min (max 5 mg); Child ≥5 yr: 1 mg/dose q2-5 min (max 10 mg)
- Rectal diazepam: 0.5 mg/kg; widely used by EMS in children
- Buccal midazolam: 0.5 mg/kg (max 10 mg) - more effective than rectal diazepam in children
- Children metabolize antiepileptics faster - weight-based dosing is essential
Nonconvulsive SE - Key Points
- Suspect in: prolonged postictal state, subtle motor signs (twitching, eye deviation, blinking), unexplained coma or confusion
- Diagnosis requires EEG
- Treat similarly to convulsive SE once diagnosed
Prognosis
Mortality increases with:
- Delayed diagnosis/treatment
- Age >60 years
- No prior seizure history
- Nonconvulsive SE (often missed)
- Underlying etiology severity
Sources:
- Tintinalli's Emergency Medicine, 9th ed., Ch. 171 (primary)
- Rosen's Emergency Medicine, 9th ed., Ch. 169
- Harriet Lane Handbook, 23rd ed. (pediatric dosing)
- 2025 Surgical Critical Care SE Management Guidelines
- ENLS Status Epilepticus Protocol v6.0, July 2024
This is a shared conversation. Sign in to Orris to start your own chat.