Anatomy radiological represention pelvis and clinical of pelvic injury
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have rich, comprehensive content from multiple authoritative textbooks. Let me compile the full detailed response:
Pelvis: Anatomy, Radiological Representation, and Clinical Aspects of Pelvic Injury
Part 1: Surgical and Radiographic Anatomy of the Pelvis
Bony Architecture
The pelvis is a ring-shaped bony structure formed by three paired bones - the ilium, ischium, and pubis - which fuse to form the innominate (hip) bone on each side, connected posteriorly to the sacrum and coccyx. Key bony landmarks include:
- Iliac crest - superior border of the ilium
- Anterior superior iliac spine (ASIS) and Anterior inferior iliac spine (AIIS)
- Symphysis pubis - the anterior midline articulation
- Superior and inferior pubic rami
- Ischial tuberosity and ischial spine
- Obturator foramen - largest foramen in the skeleton
- Acetabulum - formed by contributions of all three bones (with anterior and posterior columns)
- Sacroiliac (SI) joints - the posterior articulations
- Sacrum (with anterior foramina S1-S4) and coccyx
The pelvic inlet is formed by the arcuate line of the ilium, the pubic pecten, and the sacral promontory. The pelvic outlet is bounded anteriorly by the pubic symphysis, laterally by the inferior pubic rami, ischial tuberosities, and sacrotuberous ligaments, and posteriorly by the coccyx.
Fig. 46.1 - Bony Pelvic Anatomy (Anterior and Lateral views):
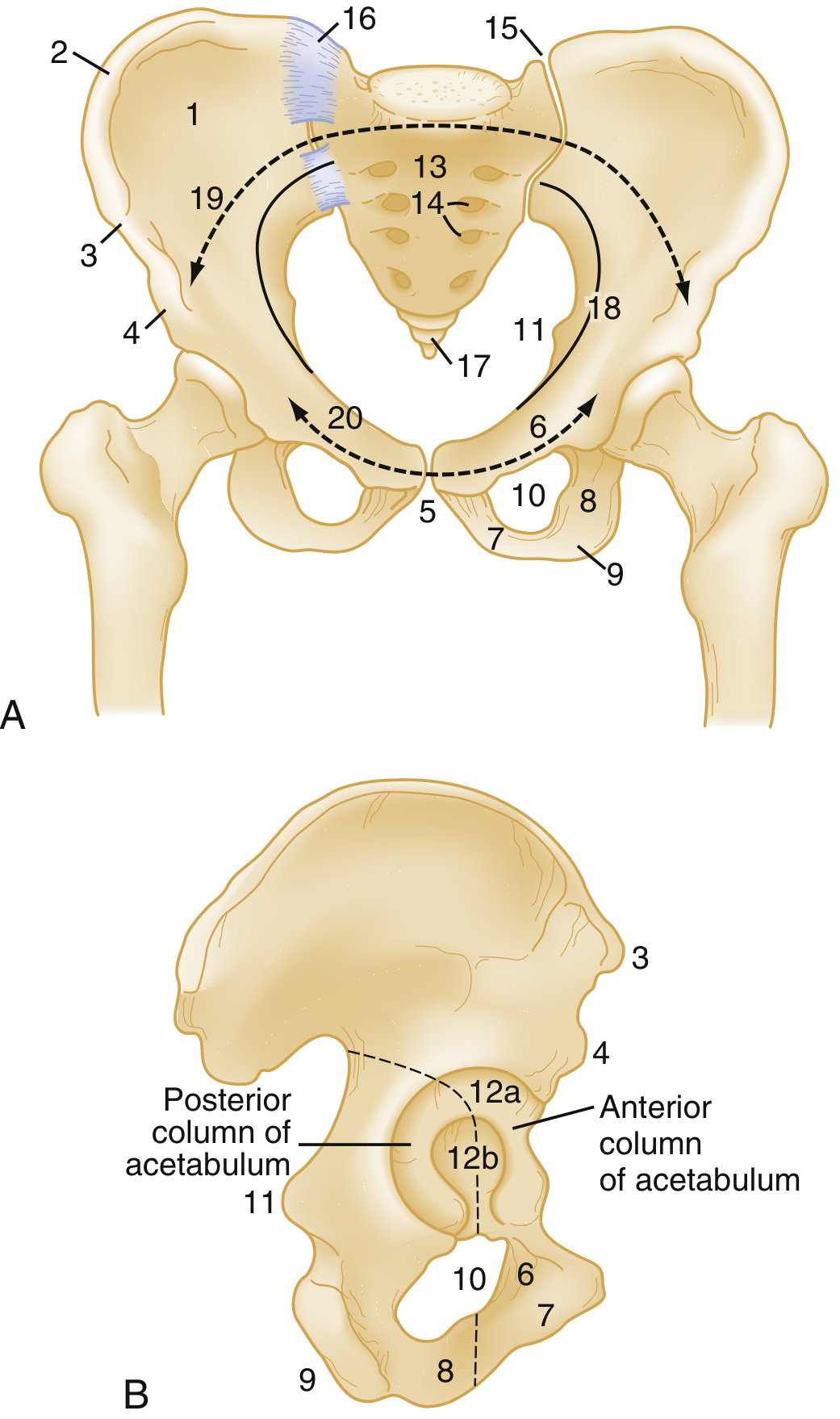
Anterior view (A) showing the pelvic ring with weight-bearing arch (19-20, dashed line), sacroiliac joints (15), sacrum (13), anterior sacral foramina (14), symphysis pubis (5), obturator foramina (10), ASIS (3), AIIS (4). Lateral view (B) showing anterior and posterior columns of the acetabulum.
- Rosen's Emergency Medicine, p. 667
Ligamentous Anatomy (Critical for Stability)
The pelvic ring is held together by a powerful ligamentous complex. Understanding this is essential to interpreting radiological instability.
Anterior stabilizers:
- Symphysis pubis fibrocartilaginous disc - the primary anterior mechanical stabilizer
Posterior stabilizers (the "posterior tension band"):
- Anterior sacroiliac ligament - thinner, less strong
- Posterior sacroiliac (interosseous) ligament - the strongest ligament in the body, running deep between sacrum and ilium
- Iliolumbar ligament - connects L5 transverse process to iliac crest
- Sacrospinous ligament - triangular, from lateral sacrum to ischial spine; limits external rotation
- Sacrotuberous ligament - strong broad band, from dorsal sacrum to ischial tuberosity; resists vertical shear
Disruption of the posterior ligaments is the primary cause of a mechanically unstable pelvic fracture.
Fig. 46.2 - Pelvic Ligaments (Anterior view):
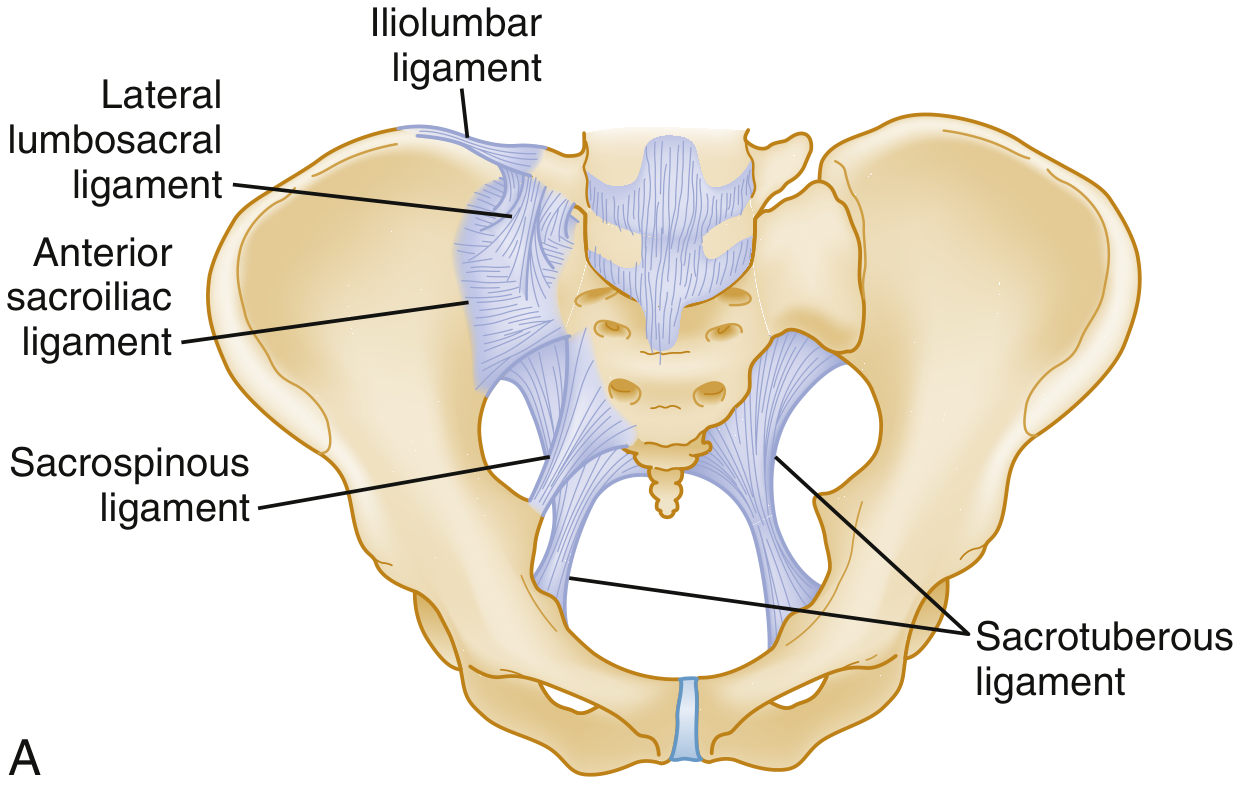
The sacrospinous ligament lies anterior to the sacrotuberous ligament. Together with the posterior sacroiliac and iliolumbar ligaments, these form the posterior tension band of the pelvis.
- Rosen's Emergency Medicine, p. 667
Vascular Anatomy (Critical for Hemorrhage Risk)
Most pelvic blood supply derives from the internal iliac (hypogastric) arteries, which course at the level of the sacroiliac joints and give off:
- Superior gluteal artery - largest branch; most commonly injured in posterior arch fractures
- Internal pudendal artery - injured in pubic rami fractures
- Obturator artery
- Superior and inferior vesical arteries
- Inferior gluteal artery
The venous plexus is valveless and thin-walled (cannot contract after injury), accounting for the massive hemorrhage potential in pelvic fractures.
Fig. 46.3 - Internal Iliac Plexus of Arteries and Veins:
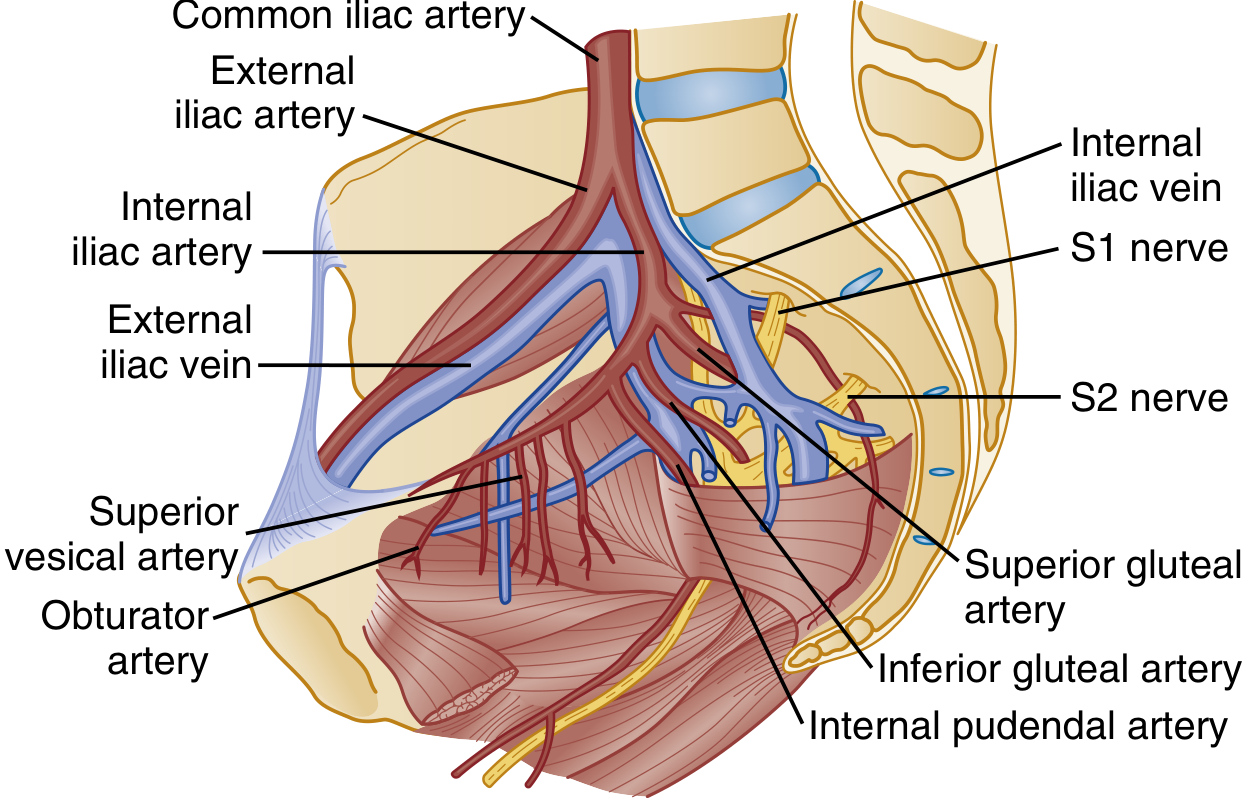
Note the common iliac bifurcation into internal and external iliac vessels, with key branches (superior gluteal, obturator, internal pudendal, superior vesical, inferior gluteal arteries) and their relationship to the S1 and S2 nerve roots.
- Rosen's Emergency Medicine, p. 668
Neurological Anatomy
The cauda equina travels through the sacral canal and exits through sacral foramina to form the lumbosacral plexus. Injury to the posterior pelvis and sacrum can cause:
- Lower extremity neurological deficits (L4-S3)
- Autonomic dysfunction affecting bowel, bladder, and genitalia
- Sciatic nerve injury (particularly with posterior fracture-dislocations)
- Rosen's Emergency Medicine, p. 667
Part 2: Radiological Representation
Plain Radiography
Indications for AP pelvis radiograph:
- Hemodynamic instability
- Pelvic tenderness or physical examination findings suggesting fracture
- Hip fracture/dislocation suspicion
- In unstable blunt trauma: early identification for rapid mobilization of angiography resources
Limitations:
- Sensitivity is only ≤85% for detecting pelvic fractures vs CT
- Sacral fractures are commonly missed due to osteoporosis and overlying bowel gas
- Inferior to CT for evaluating pelvic ring instability
Radiographic clues to fracture mechanism:
- Horizontal rami fractures → lateral compression injury
- Vertical rami fractures → vertical shear force
- Pubic symphysis diastasis → anteroposterior (open-book) injury
- Sacral fractures / SI joint widening → posterior arch disruption
Additional plain film views (when CT unavailable or for acetabular evaluation):
- Judet views (45° obliques) for acetabular columns
- Inlet view (40° caudad) - shows AP displacement of pelvic ring
- Outlet view (40° cephalad) - shows vertical displacement of sacrum/SI joints
CT Scan - Gold Standard
CT is the definitive imaging modality for pelvic injury:
- More sensitive than plain films for pelvic fractures
- Superior for evaluating pelvic ring instability
- Contrast-enhanced CT can detect: ligamentous injury, contrast extravasation (80-90% sensitive for arterial bleeding), pelvic hematoma, retroperitoneal bleeding
- Up to 50% of elderly patients with plain-film-only pubic ramus fractures have associated posterior ring disruption visible only on CT
- Sacral fractures frequently require CT (plain films miss them due to bowel gas and degenerative changes)
- Tintinalli's Emergency Medicine, p. 1879
FAST Examination
- Used in hemodynamically unstable trauma patients to detect intraperitoneal blood
- Overall sensitivity 81%, specificity 87% for free peritoneal fluid in major pelvic injury
- False-positive rate up to 30% - pelvic hematoma, retroperitoneal blood, or urine from ruptured bladder can mimic free fluid
- A negative FAST does not exclude visceral injury when significant mechanism is present
- Tintinalli's Emergency Medicine, p. 1882
Part 3: Classification of Pelvic Fractures
Tile Classification (Stability-Based)
| Type | Stability | Description |
|---|---|---|
| A | Stable | Posterior arch intact; avulsion fractures, isolated iliac wing, pubic rami, minimally displaced ring, transverse sacrum/coccyx |
| B | Partially stable | Incomplete posterior arch disruption; "open-book" (AP compression) and lateral compression; rotationally unstable but vertically stable |
| C | Unstable | Complete posterior arch disruption; vertical shear injuries; both rotationally and vertically unstable |
- Rosen's Emergency Medicine, p. 668
Young-Burgess Classification (Mechanism-Based)
| Pattern | Mechanism | Subtypes | Instability |
|---|---|---|---|
| Lateral Compression (LC) | Side impact (broadsided MVC, pedestrian struck from side) | LC I: sacral crush ipsilateral; LC II: sacral crush + posterior SI disruption/crescent fracture; LC III: "windswept pelvis" (internal + contralateral external rotation) | Rotationally unstable |
| Anteroposterior Compression (APC) / Open-Book | Head-on MVC, motorcycle crash | APC I: symphysis diastasis <2.5 cm; APC II: diastasis >2.5 cm + anterior SI disruption; APC III: complete SI joint disruption | Rotationally + vertically unstable (APC III) |
| Vertical Shear (VS) | Fall from height, jump | Vertical displacement of symphysis and SI joints | Rotationally + vertically unstable |
| Combined Mechanism (CM) | Mixed force vectors | Combination of above | Variable |
Complications by Pattern (Young-Burgess):
| Category | Severe Hemorrhage | Bladder Rupture | Urethral Injury |
|---|---|---|---|
| Lateral Compression | 60% | 20% | 20% |
| AP Compression (APC I) | 1% | 8% | 12% |
| Vertical Shear | 53% | 14% | 36% |
| Mixed Patterns | 58% | 16% | 21% |
- Tintinalli's Emergency Medicine, p. 1880
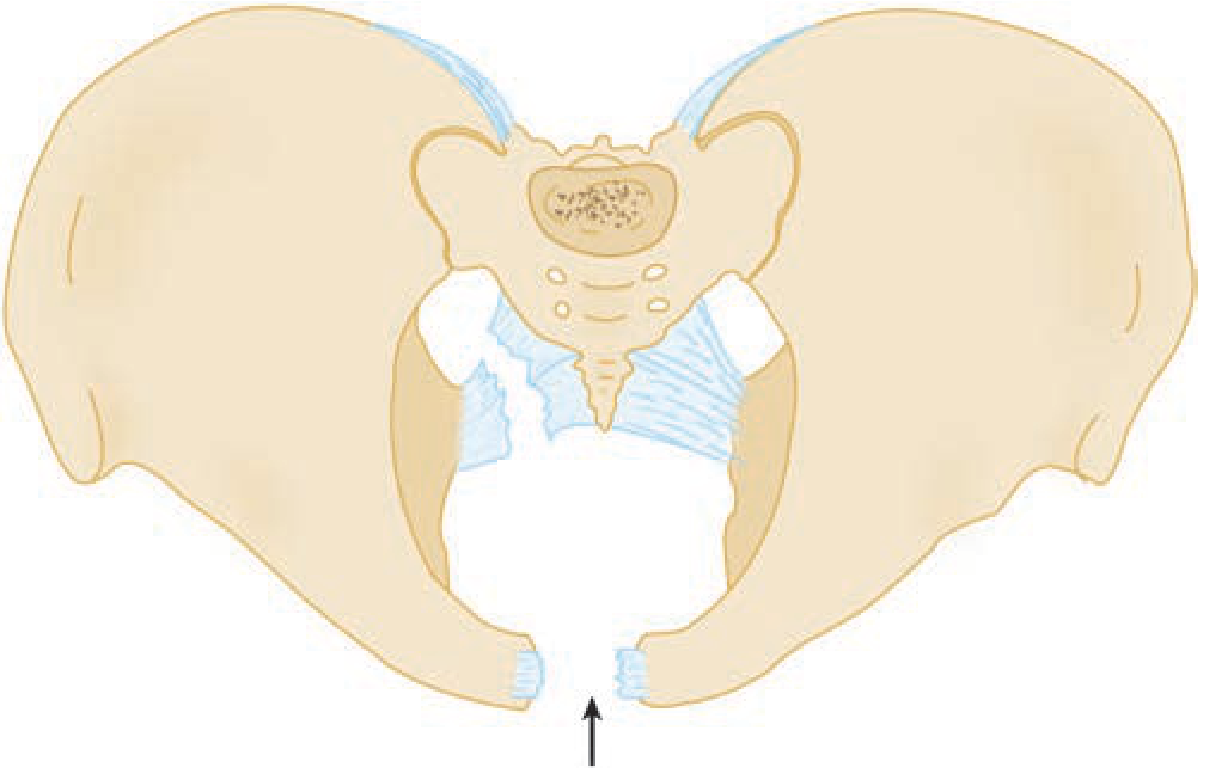
Fracture Pattern Illustrations
Lateral Compression Fracture:
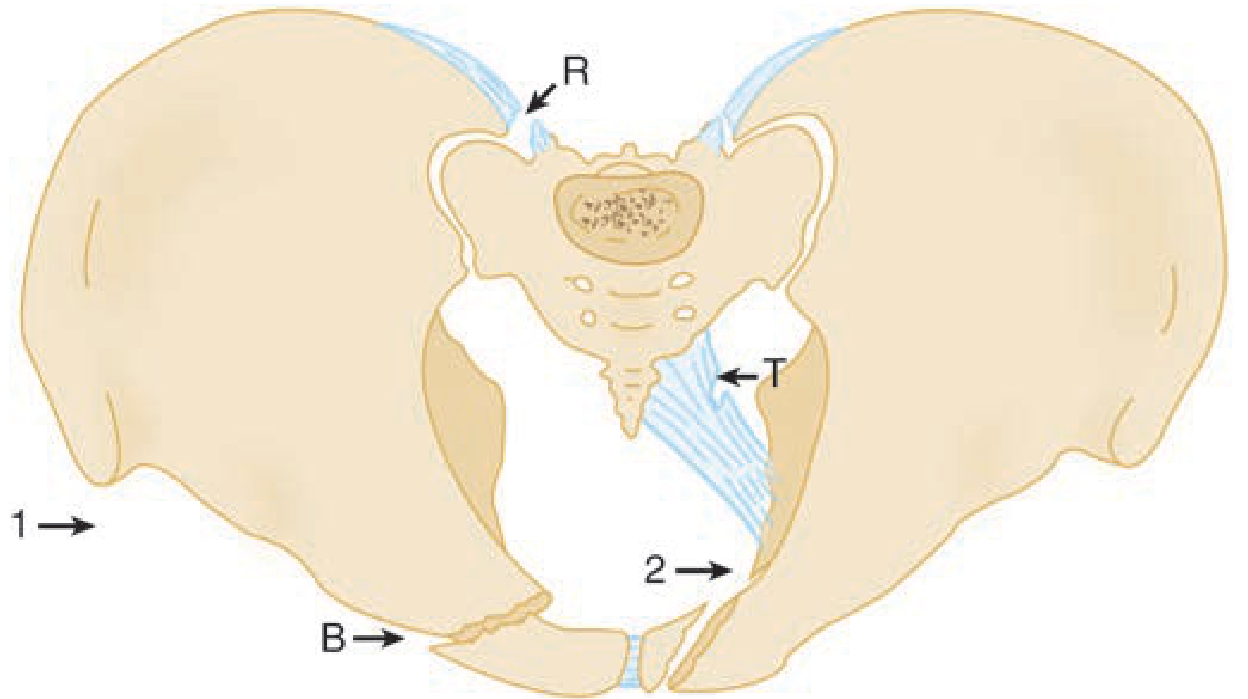
Arrows 1 and 2 indicate the compression forces. R = ruptured posterior sacroiliac ligaments, T = sacrospinous/sacrotuberous complex disruption, B = pubic ramus fracture.
Open-Book (APC) Fracture:
Arrow shows AP force "opening" the pelvis. The symphysis splays wide, and posterior sacral ligaments rupture bilaterally.
Vertical Shear Fracture:
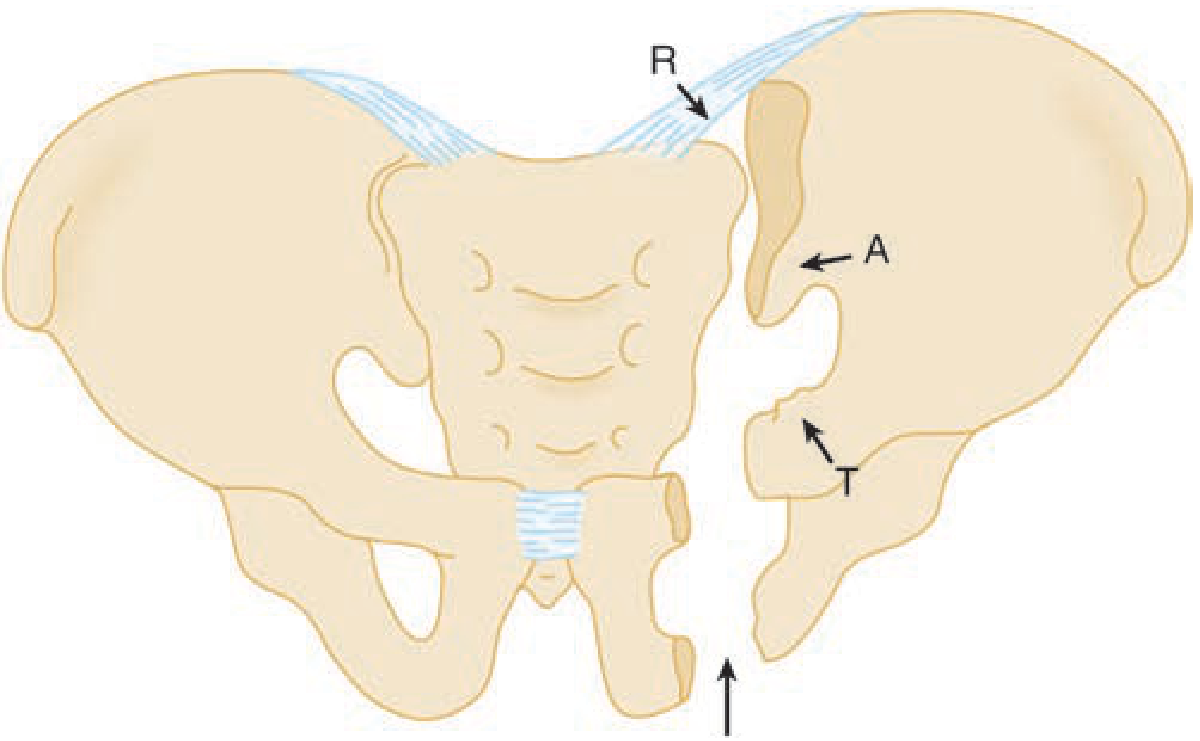
Arrow shows vertical force vector. R = posterior SI ligaments, A = anterior SI ligaments, T = sacrospinous/sacrotuberous complex. The entire hemipelvis displaces superiorly.
Avulsion and Single-Bone Fractures (Pelvic Ring Intact)
These are more common than pelvic ring disruption:
| Fracture | Mechanism | Key Clinical Points |
|---|---|---|
| Iliac wing (Duverney) | Direct lateral-to-medial trauma | Swelling/tenderness over iliac crest; rarely requires surgery |
| Pubic ramus (single) | Fall in elderly; exercise-induced stress in young | Most common pelvic ring fracture; usually stable |
| Ischial tuberosity avulsion | Sudden hamstring contraction (young athletes) | Pain on sitting, hamstring movement |
| ASIS avulsion | Sartorius pull | Running athletes |
| AIIS avulsion | Rectus femoris pull | Kicking athletes |
| Sacral fracture | Direct AP trauma or fall | Zone 1-3; neurological risk in Zones 2-3; often missed on plain films |
| Coccyx fracture | Fall in sitting position | More common in women; treated conservatively |
| Straddle fracture | Direct blow with straddle mechanism | Both rami on BOTH sides - butterfly segment; GU injury common |
- Tintinalli's Emergency Medicine, p. 1880-1881
Acetabular Fractures
Usually result from motor vehicle collisions via two mechanisms:
- Lateral force through the hip (dashboard or direct impact)
- Posterior force through the femur (knee-versus-dashboard)
Associated injuries include femur, hip, and knee injuries. Judet oblique views (45°) are used for plain film evaluation; CT is essential for classification and surgical planning.
Part 4: Clinical Presentation and Physical Examination
History
- High-energy mechanisms: MVC (especially head-on, side-impact, motorcycle), pedestrian-vs-vehicle, fall from height
- Low-energy mechanisms: Ground-level fall (elderly, osteoporosis), sport injuries (avulsions in young athletes)
Physical Examination
- Inspection: Perineal ecchymosis, scrotal/labial hematoma, leg length discrepancy, abnormal limb rotation, open wounds
- Palpation: Pelvic instability (gently press on iliac wings - anteroposterior and lateral compression) - perform ONCE only to avoid dislodging clot
- Urethral evaluation: Blood at urethral meatus, inability to void, "high-riding prostate" on rectal exam → suggests urethral disruption (do NOT insert Foley without retrograde urethrogram)
- Rectal examination: Sphincter tone, high-riding prostate, bone fragments
- Vaginal examination: Lacerations indicating open fracture
- Neurological assessment: Lower extremity motor/sensory, perineal sensation, sphincter function
Red Flags for Unstable Pelvic Fracture
- Hemodynamic instability (SBP <90 mmHg)
- Leg length discrepancy or rotational deformity
- Palpable posterior pelvic instability
- High-riding prostate or blood at urethral meatus
- Perineal hematoma
Part 5: Emergency Management
Initial Stabilization
- Primary survey (ABCDE) - hemorrhage control is priority
- Pelvic binder - wrap tightly at level of greater trochanters:
- Reduces pelvic volume, stabilizes fracture ends, tamponades venous hemorrhage
- Effective for open-book and vertical shear fractures
- Contraindicated/harmful in lateral compression fractures (already internally rotated - further compression worsens injury)
- Hemostatic resuscitation - massive transfusion protocol, crystalloids, blood products
- Up to 4 liters of blood can accumulate in the pelvis before tamponade occurs
Indications for ICU Admission
- Initial hematocrit <30%
- Pelvic hematoma on CT scan
- SBP <90 mmHg on arrival
- Base deficit <6 mmol/L or worsening base deficit >2 mmol/L
- Tintinalli's Emergency Medicine, p. 1882
Hemorrhage Control Algorithm
| Hemodynamic Status | FAST Result | Next Step |
|---|---|---|
| Unstable | Positive | Emergency laparotomy (possible intraperitoneal source) |
| Unstable | Negative | CT + pelvic angioembolization OR extraperitoneal packing in OR |
| Stable | Any | CT scan for full evaluation, then definitive management |
Definitive Hemorrhage Control Options
- Pelvic angiography and embolization - for arterial bleeding (contrast extravasation on CT)
- Preperitoneal (extraperitoneal) pelvic packing - for venous/bony bleeding
- External fixator - emergent frame to reduce pelvic volume in open-book fractures
- Internal fixation (ORIF) - definitive surgical management for unstable fractures
Part 6: Associated Injuries and Complications
| System | Injury | Association |
|---|---|---|
| Vascular | Retroperitoneal hemorrhage (venous >arterial) | All unstable patterns; especially APC and VS |
| Urological | Bladder rupture (intraperitoneal or extraperitoneal) | LC: 20%; VS: 14%; open-book: 8% |
| Urethral | Posterior urethral disruption | VS: 36%; LC: 20%; all severe pelvic ring injuries |
| Neurological | Lumbosacral plexus injury, sciatic nerve | Posterior fractures, vertical shear |
| Gynecological | Vaginal laceration (open fracture), uterine/ovarian injury | Straddle fracture, APC III |
| Rectal/GI | Rectal perforation | Open pelvic fracture |
| Orthopedic | Femur fracture, hip dislocation, acetabular fracture | APC, dashboard injuries |
Summary: Radiological Signs by Fracture Type
| Radiographic Finding | Fracture Type |
|---|---|
| Pubic symphysis diastasis >2.5 cm | APC II/III (open-book) |
| Horizontal pubic rami fractures | Lateral compression |
| Vertical pubic rami fractures | Vertical shear |
| Superior hemipelvis displacement | Vertical shear |
| Sacral fractures (ipsilateral sacral crush) | LC I/II |
| SI joint widening | APC II/III, VS |
| Unilateral "crescent" iliac fracture with SI disruption | LC II |
| Bilateral SI + pubic symphysis disruption | APC III, LC III ("windswept") |
Sources:
- Tintinalli's Emergency Medicine: A Comprehensive Study, pp. 1879-1882
- Rosen's Emergency Medicine: Concepts and Clinical Practice, pp. 667-670
- Gray's Anatomy for Students, pp. 618-620
This is a shared conversation. Sign in to Orris to start your own chat.