Pyloric stenosis, IHPS, duodenal stenosis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Here is the full structured answer:
Infantile Hypertrophic Pyloric Stenosis (IHPS) and Duodenal Stenosis
PART 1: Infantile Hypertrophic Pyloric Stenosis (IHPS)
Epidemiology
- Incidence: ~1 in 300-900 live births; the most common surgical cause of vomiting in infants
- M:F ratio = 4-5:1 (boys far more commonly affected)
- Presents between 3rd and 6th weeks of life (range 2-10 weeks); rare after 12 weeks
- Associated with: first-born children, prematurity, young maternal age, monozygotic twins (high concordance)
- Risk increased in siblings (~6% vs ~0.2% general population)
- Associated syndromes: Turner syndrome, trisomy 18
- Erythromycin or azithromycin exposure (orally or via breast milk) in the first 2 weeks of life increases risk
Pathology
Hypertrophy and hyperplasia of the pyloric muscularis propria (circular > longitudinal muscles) causes progressive gastric outlet obstruction. This is NOT a congenital anomaly - the muscle grows after birth. Mucosal and submucosal edema and inflammation may also contribute. The hypertrophied pylorus forms a firm, palpable "olive."
Clinical Features
| Feature | Details |
|---|---|
| Vomiting | Forceful, projectile, non-bilious (proximal to bile duct entry) |
| Timing | Typically starts ~3-6 weeks; worsens progressively |
| Feeding | Infant remains hungry after vomiting ("hungry vomiter") |
| Peristaltic waves | Visible left-to-right waves across upper abdomen just before vomiting |
| Palpable mass | Firm, olive-shaped, 1-2 cm epigastric mass - nearly pathognomonic; found in up to 90% if stomach decompressed first (now found in <30% in contemporary practice due to early presentation) |
| Dehydration | Sunken fontanelles, dry mucous membranes, decreased urine output |
Metabolic Derangement
Persistent vomiting of gastric acid leads to:
Hypochloremic, hypokalemic metabolic alkalosis
- Loss of HCl → low Cl⁻, elevated HCO₃⁻
- Paradoxical aciduria (kidneys preferentially retain Na⁺ over H⁺ in severe alkalosis)
- Bicarbonate > 30 mEq/L = respiratory depression risk → must be corrected before anesthesia
Diagnosis
Ultrasound is the gold standard (sensitivity and specificity up to 98-100%):
| Ultrasound Criterion | Threshold |
|---|---|
| Pyloric muscle thickness | ≥ 4 mm |
| Pyloric canal length | ≥ 15-17 mm |
| Other signs | Shoulder sign (muscle bulging into antrum), nipple sign (hyperechoic mucosa protrudes into stomach), cervix sign |
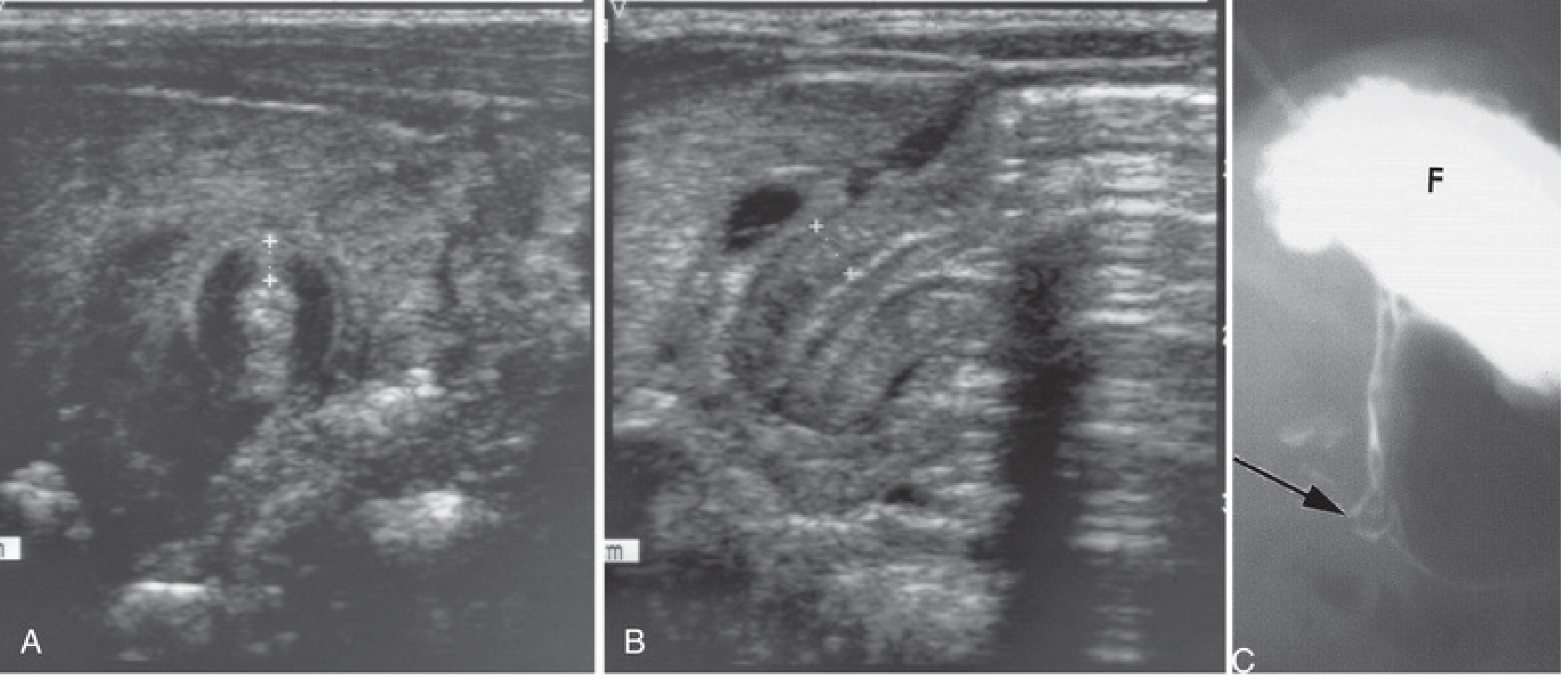
A: Ultrasound - pyloric muscle wall thickness >4mm. B: Pyloric channel length >14mm. C: Contrast study showing narrowed pyloric canal (arrow) with markedly distended fundus (F). From The Developing Human - Clinically Oriented Embryology.
Upper GI contrast series (UGI) is used when ultrasound is equivocal (can show elongated "string sign" of narrowed pyloric channel) and to evaluate for other causes (GERD, malrotation, antroduodenal webs).
Preoperative Resuscitation
Surgery is NEVER a true emergency. Resuscitate first:
- One to two boluses of normal saline 20 mL/kg
- D5/NS at 1.5x maintenance with electrolytes
- Check electrolytes every 6-12 hours
Endpoints for readiness for surgery:
- Wet diapers (adequate urine output)
- Chloride ≥ 90-100 mEq/L
- Bicarbonate ≤ 30 mEq/L
Do NOT proceed to anesthesia with bicarbonate > 30 mEq/L (risk of postoperative apnea/respiratory arrest).
Surgical Treatment: Fredet-Ramstedt Pyloromyotomy
The operation of choice - open (umbilical or RUQ incision) or laparoscopic (now standard at most children's hospitals):
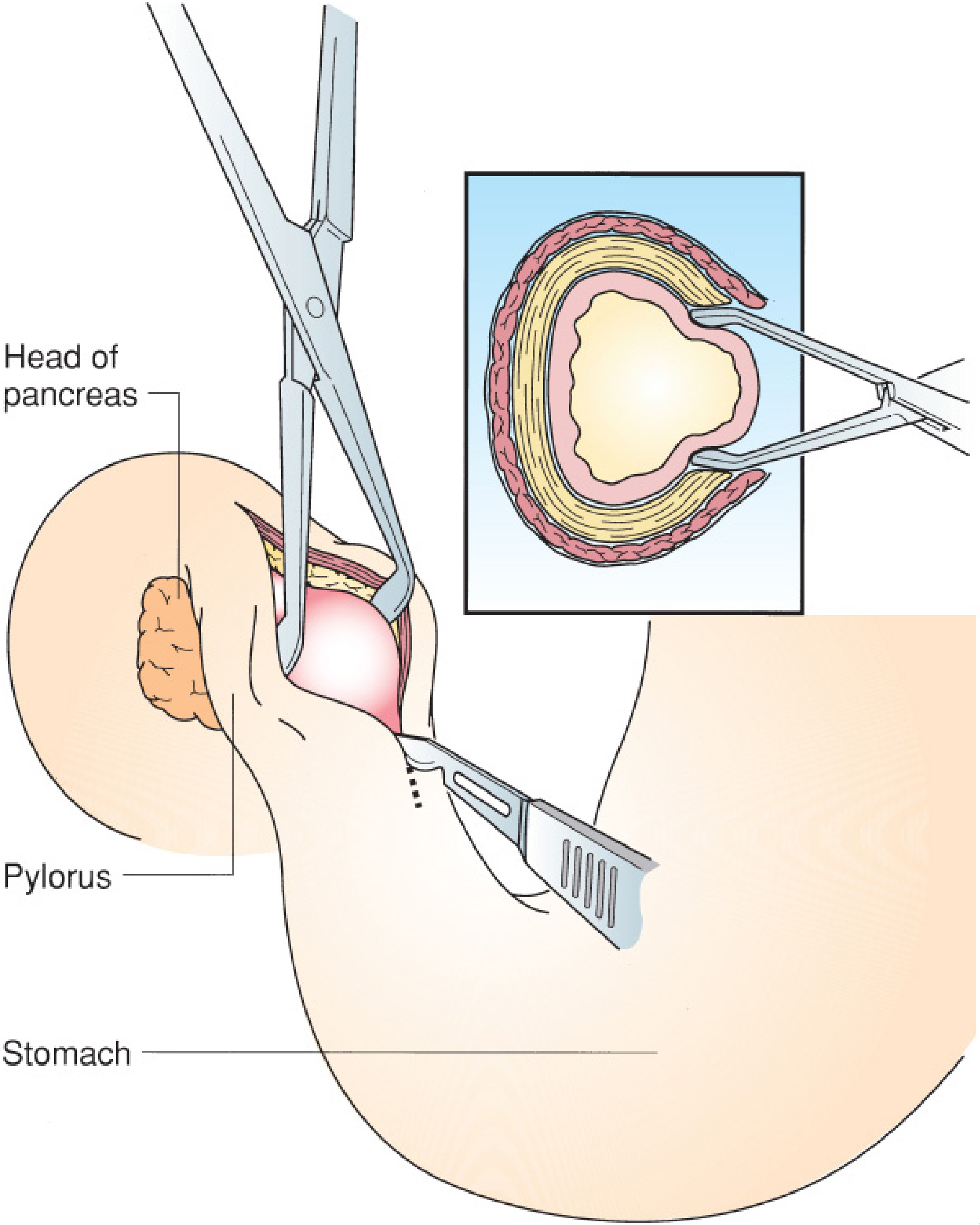
Ramstedt pyloromyotomy. The hypertrophied pyloric muscle is incised longitudinally. The inset shows submucosal herniation into the myotomy site, confirming adequate division. From Mulholland & Greenfield's Surgery.
- A single longitudinal incision through the anterior wall of the pyloric canal, from stomach to duodenal junction
- Muscle is spread until submucosa bulges up freely = complete myotomy
- A leak test (30-60 mL air via orogastric tube) confirms no mucosal perforation
- Laparoscopic approach: 3 ports (umbilical + two 3-mm stab incisions)
Complications:
- Incomplete myotomy - ongoing projectile vomiting; requires return to OR
- Mucosal perforation - repair + buttress with omentum, or rotate pylorus 180° and re-myotomize
- Both are rare; mortality is distinctly unusual
Postoperative feeding: Start at 6-8 hours; ad lib with 60-mL limit; discharge usually within 24-36 hours.
Acquired Pyloric Stenosis (Adults)
Occurs due to antral gastritis, peptic ulcers near the pylorus, or carcinoma of the distal stomach/pancreas causing fibrosis or malignant infiltration.
PART 2: Duodenal Stenosis (and Atresia)
Embryology & Etiology
The duodenum develops in the 4th week. During weeks 5-6, luminal obliteration occurs due to mucosal proliferation, followed by gradual recanalisation over subsequent weeks. Duodenal atresia (DA) and stenosis result from failure of this recanalisation process.
Forms of obstruction:
- Complete membrane obstructing the lumen (most common)
- Blind-ending pouch with fibrous cord to distal duodenum
- Blind-ending pouch with no connection
- Perforate membranes / webs (cause partial stenosis)
- Extrinsic compression: annular pancreas or preduodenal portal vein
Location: In 80% of cases, obstruction is just distal to the ampulla of Vater → bilious vomiting
- Pre-ampullary obstruction (15-20%) → non-bilious vomiting
Incidence & Associated Anomalies
- ~1 per 200,000 live births (combined atresia, stenosis, web); slight female preponderance
- Associated anomalies present in >50% of patients:
| Association | Frequency |
|---|---|
| Down syndrome (Trisomy 21) | 25-30% (some series >50%) |
| Congenital heart disease | ~20% |
| Malrotation | 20-30% |
| VACTERL (incl. esophageal atresia) | OA in ~10% |
| Renal anomalies, imperforate anus, CNS lesions | Variable |
Any infant with Trisomy 21 and bilious vomiting must be evaluated for duodenal stenosis/atresia.
Clinical Features
Prenatal:
- Dilated stomach + duodenal cap on US (double bubble in utero)
- Polyhydramnios in 33-50% (fetus cannot swallow/absorb amniotic fluid)
- IUGR, prematurity
Postnatal:
- Early bilious vomiting (first day of life in atresia; may be delayed months to years in partial stenosis/web)
- Upper abdominal distension
- Duodenal stenosis/partial membrane may present at any age depending on degree - can even go undiagnosed until adulthood
Diagnosis
Plain X-ray - "Double Bubble" sign:

Classic "double-bubble" sign. Two dilated gas-filled structures (stomach + first part of duodenum). No distal gas confirms complete atresia. From Grainger & Allison's Diagnostic Radiology.
- Two air bubbles = dilated stomach + dilated proximal duodenum
- No distal gas = complete atresia; classic double bubble in a stable child does not require further imaging before surgery
- If distal gas is present = partial obstruction (stenosis, web) - warrants upper GI contrast study
Upper GI contrast study (for partial obstruction):
- Duodenal stenosis: narrowing in the second part of duodenum
- Duodenal web: thin filling defect extending across lumen with pre-stenotic dilatation
Ultrasound: Can demonstrate duodenal obstruction, especially with clear fluids given first to distend proximal gut.
Treatment
Surgical correction after stabilization:
- Duodenoduodenostomy (anastomosis of proximal to distal duodenum) - operation of choice for atresia
- Web excision / duodenoplasty for membranous obstruction
- Must evaluate for and address malrotation intraoperatively (present in 20-30%)
Comparison at a Glance
| Feature | IHPS | Duodenal Stenosis/Atresia |
|---|---|---|
| Cause | Post-natal muscle hypertrophy | Failed recanalisation of duodenum (failure of vacuolisation, 8-10 wks) |
| Onset | 3-6 weeks after birth | Day 1 (atresia) or any age (stenosis) |
| Vomiting | Non-bilious, projectile | Bilious (80%) or non-bilious (20% if pre-ampullary) |
| Key X-ray sign | Normal (US is gold standard) | Double bubble on plain film |
| Key US finding | Pyloric muscle ≥4 mm, length ≥15-17 mm | Dilated stomach + duodenum |
| Associated anomalies | Erythromycin exposure; rarely Turner/T18 | Down syndrome (25-50%), VACTERL |
| Metabolic disturbance | Hypochloremic hypokalemic alkalosis | Dehydration ± alkalosis (less specific) |
| Surgery | Fredet-Ramstedt pyloromyotomy | Duodenoduodenostomy |
| Emergency? | No - resuscitate first | No - stabilize first |
Sources: Current Surgical Therapy 14e; Robbins & Cotran Pathologic Basis of Disease; The Developing Human - Clinically Oriented Embryology; Grainger & Allison's Diagnostic Radiology; Mulholland & Greenfield's Surgery 7e; Sleisenger & Fordtran's Gastrointestinal and Liver Disease.
This is a shared conversation. Sign in to Orris to start your own chat.