Acl rehab 10 marks pg orthopaedics answer with flow chart and images
ACL rehabilitation protocol phases orthopaedics 10 marks answer
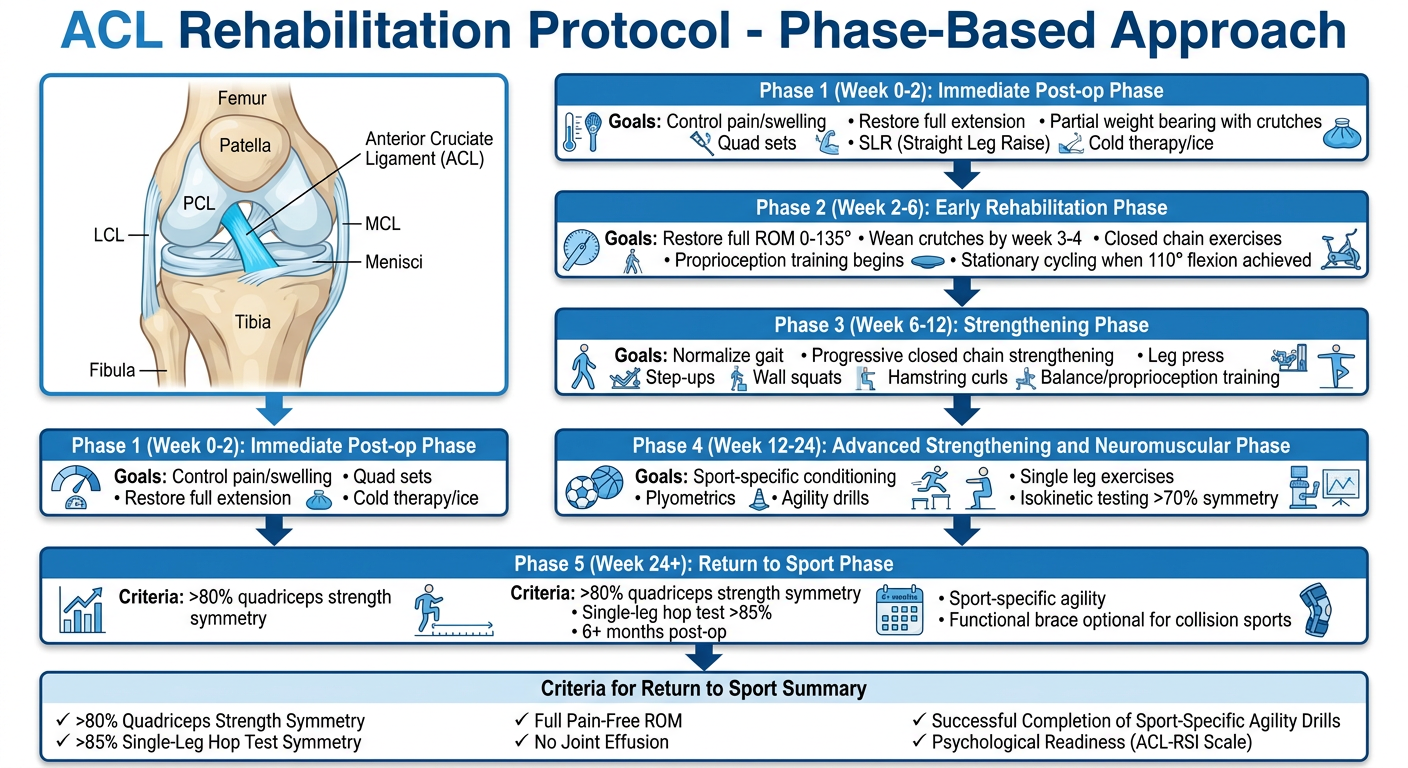
A detailed medical flowchart titled "ACL Rehabilitation Protocol - Phase-Based Approach" showing 5 phases in a vertical flowchart with downward arrows connecting each phase. Phase 1 (Week 0-2): "Immediate Post-op Phase" - goals: control pain/swelling, restore full extension, partial weight bearing with crutches, quad sets, SLR, cold therapy/ice. Phase 2 (Week 2-6): "Early Rehabilitation Phase" - goals: restore full ROM 0-135°, wean crutches by week 3-4, closed chain exercises, proprioception training begins, stationary cycling when 110° flexion achieved. Phase 3 (Week 6-12): "Strengthening Phase" - goals: normalize gait, progressive closed chain strengthening, leg press, step-ups, wall squats, hamstring curls, balance/proprioception training. Phase 4 (Week 12-24): "Advanced Strengthening and Neuromuscular Phase" - goals: sport-specific conditioning, plyometrics, agility drills, single leg exercises, isokinetic testing >70% symmetry. Phase 5 (Week 24+): "Return to Sport Phase" - criteria: >80% quadriceps strength symmetry, single-leg hop test >85%, 6+ months post-op, sport-specific agility, functional brace optional for collision sports. Include a box at top with ACL anatomy showing the ligament, and at the bottom a "Criteria for Return to Sport" summary box. Use clinical blue and white color scheme with clear medical diagram styling.
ACL anatomy diagram knee ligament image rehabilitation
ACL Rehabilitation - PG Orthopaedics (10 Marks)
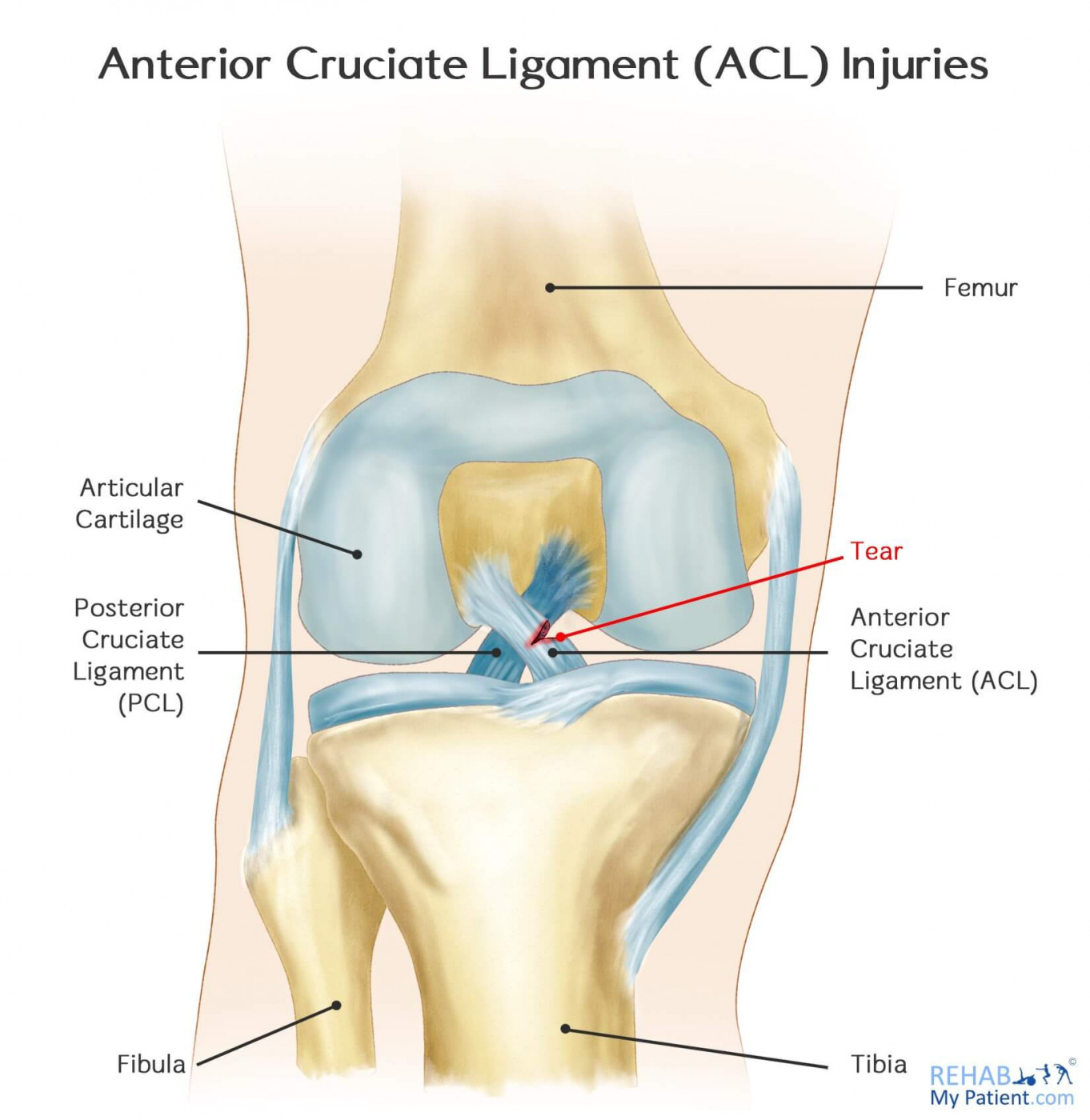
Anatomy Recall
ACL Rehabilitation - Phase-Based Protocol
FLOWCHART
Phase-by-Phase Details
PHASE 1: Immediate Post-op (Week 0-2)
| Component | Details |
|---|---|
| Extension | Active and passive knee extension with heel elevated, knee supported posteriorly |
| Brace | Knee immobilized in fully extended brace immediately post-op - prevents flexion contracture and protects weakened quadriceps; flexion allowed immediately |
| Weight bearing | Partial weight bearing with crutches allowed immediately after isolated ACL reconstruction |
| Cold therapy | Ice bags used liberally (note: efficacy in reducing swelling/hospital stay not strongly demonstrated in literature) |
| Exercises | Quad sets, straight-leg raises (SLR), ankle pumps |
| Electrical stimulation | Can be used sparingly for muscle re-education if poor quadriceps contraction; does NOT decrease atrophy long term |
| BFR (Blood Flow Restriction) | Proximal air tourniquet during PT; low-intensity exercise with vascular occlusion promotes muscular hypertrophy and attenuates atrophy |
PHASE 2: Early Rehabilitation (Week 2-6)
| Component | Details |
|---|---|
| ROM | Progress to full flexion 0-135°; maintain full extension |
| Crutches | Discontinued by 3-4 weeks postoperatively |
| Cycling | Stationary cycling may begin when 110° flexion is achieved |
| Strengthening | Closed kinetic chain exercises (CKC) preferred - leg press, mini squats, wall slides |
| CPM machines | NOT recommended routinely - literature does not support added benefit |
| Proprioception | Begin proprioceptive training in first 2 weeks |
Key principle - Open vs Closed Chain:
- Open chain exercises (resisted quad extensions) - place strain on ACL, especially in last few degrees of extension; worrisome early
- Closed chain exercises (standing) - load knee axially, joint contours stabilize knee and protect graft; associated with less patellofemoral pain, lower KT-1000 side-to-side differences, and higher patient satisfaction
PHASE 3: Strengthening Phase (Week 6-12)
- Progress closed chain program: single-leg leg press, step-ups/step-downs, lateral lunges, wall squats, hamstring curls
- Begin isolated hamstring curls (hamstrings act in concert with ACL to prevent anterior tibial translation)
- Multi-plane hip strengthening
- Balance board, proprioceptive neuromuscular facilitation (PNF)
- Stationary cycling with resistance
- Running on treadmill when normal gait is restored
PHASE 4: Advanced Neuromuscular Phase (Week 12-24)
- Progressive plyometrics: double-leg jumps → single-leg jumps → depth jumps
- Agility drills: shuttle runs, figure-8, lateral cuts
- Isokinetic strength testing (Cybex) - target >70% symmetry with uninvolved limb
- Sport-specific drills in a non-contact environment
- Neuromuscular and strength training combined (knee function and pain reduction better with neuromuscular training; hamstring strength better with strength training alone - best outcomes with combination)
PHASE 5: Return to Sport (Week 24+, criteria-based)
| Criterion | Target |
|---|---|
| Time since surgery | Minimum 6 months (graft maturation continues to 18 months) |
| Quadriceps strength symmetry | >80% vs contralateral limb |
| Single-leg hop test (distance) | >85% limb symmetry index (LSI) |
| Single-leg triple hop | >85% LSI |
| Single-leg timed hop | >85% LSI |
| Single-leg crossover hop | >85% LSI |
| Sport-specific agility | Completed without pain/instability |
| ROM | Full, pain-free |
| Effusion | Absent |
| Psychological readiness | ACL-RSI scale |
Only 44% of patients return to competitive sport despite 90% having normal outcome scores (meta-analysis data from Campbell's 2026)
Key Rehabilitation Principles (Examinable Points)
1. Graft Protection
- Some stress to graft is desirable for healing and remodeling, but excessive load must be avoided
- Graft undergoes "ligamentization" (necrosis → revascularization → remodeling) - most vulnerable at 6-12 weeks
2. Quadriceps Recovery
- Thigh muscles atrophy rapidly post-operatively
- Tourniquet use during surgery reduces quad strength recovery at 12 weeks (equalizes by 52 weeks)
- Adductor canal block (purely sensory) preferred over femoral nerve block - provides equivalent pain relief with faster quad strength recovery
- Quad tendon autograft patients show significantly more quad weakness at 7 months vs patellar tendon or hamstring autografts
3. Blood Flow Restriction Training (BFR)
- Proximal tourniquet + low-intensity exercise
- Mechanism: recruits fast-twitch fibers in hypoxia, increases growth hormone and catecholamines, stimulates tissue growth
- Reduces post-op muscle atrophy
4. Accelerated vs Delayed Rehabilitation
- Accelerated rehabilitation (early weight bearing, early ROM) helps prevent arthrofibrosis and restores strength earlier
- Current evidence favors accelerated protocol for isolated ACL reconstruction
- Home-based programs are equally effective to supervised PT for recreational athletes
5. Functional Bracing
- Use of functional brace after ACL surgery is controversial
- Some data suggest benefit for in vivo knee kinematics
- No robust evidence supports routine brace use to decrease re-injury rate
- Can be used for collision sports - decision is individualized
Important Notes for Examination
| Point | Detail |
|---|---|
| Early return to sport is a significant risk factor for ACL reconstruction failure | |
| Graft maturation continues beyond 6 months and possibly up to 18 months | |
| Only 44% return to competitive sport (meta-analysis) | |
| Home-based rehab is as effective as supervised PT for recreational athletes | |
| Combination of neuromuscular training + strength training gives best results | |
| CPM machines not routinely recommended | |
| Electrical stimulation does NOT prevent muscle atrophy |