Teach me megaloblastic anemia in simple way for pathology University examin very simple language so I can score more
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I have everything needed. Here is a complete, exam-focused guide on megaloblastic anemia straight from Robbins Pathology:
Megaloblastic Anemia - Complete Exam Guide 🩸
Source: Robbins, Cotran & Kumar - Pathologic Basis of Disease
1. What IS Megaloblastic Anemia? (Start Here)
Think of it this way: "Big cells that can't divide properly."
The ONE core idea = DNA synthesis is impaired → cells grow in size but their nucleus cannot mature properly → you get abnormally LARGE blood cell precursors called megaloblasts.
Definition: An anemia (or pancytopenia) caused by failure of DNA synthesis, leading to an imbalance between nuclear and cytoplasmic maturation, resulting in large abnormal cells.
2. Causes - Two Big Groups to Memorize
Vitamin B12 Deficiency
| Mechanism | Examples |
|---|---|
| Decreased intake | Strict vegetarians, poor diet |
| Impaired absorption | Pernicious anemia (most important!), gastrectomy |
| Malabsorption | Ileal resection, ileitis, intestinal lymphoma |
| Competitive use | Fish tapeworm, bacterial overgrowth |
Folic Acid Deficiency
| Mechanism | Examples |
|---|---|
| Decreased intake | Alcoholism, infancy, poor diet |
| Impaired absorption | Anticonvulsants, oral contraceptives |
| Increased requirement | Pregnancy, infancy, disseminated cancer |
| Increased loss | Hemodialysis |
Also remember: Drugs like methotrexate block folate metabolism → same picture.
3. Pathogenesis - WHY Do These Vitamins Cause This?
Here is the simple chain to memorize:
B12 + Folate → needed to make THYMIDINE (one of the 4 DNA bases)
↓
Deficiency → can't make DNA properly
↓
Cells grow (cytoplasm matures) BUT nucleus can't divide
↓
NUCLEAR-CYTOPLASMIC ASYNCHRONY (nucleus looks immature, cytoplasm looks mature)
↓
Cells are large and abnormal = MEGALOBLASTS
↓
Most die in bone marrow = INEFFECTIVE HEMATOPOIESIS
↓
Result: Pancytopenia (low RBC + WBC + platelets)
One-liner for the exam: "B12 and folate are cofactors for thymidine synthesis; their deficiency causes defective DNA replication, nuclear maturation arrest, and ineffective hematopoiesis."
4. Morphology (What You See Under Microscope) - HIGH YIELD
Peripheral Blood Smear:
- Macro-ovalocytes - large, oval red cells (most characteristic)
- Hypersegmented neutrophils - 5 or more nuclear lobes (normal = 3-4 lobes)
- Anisocytosis (variation in size) + poikilocytosis (variation in shape)
- Low reticulocyte count
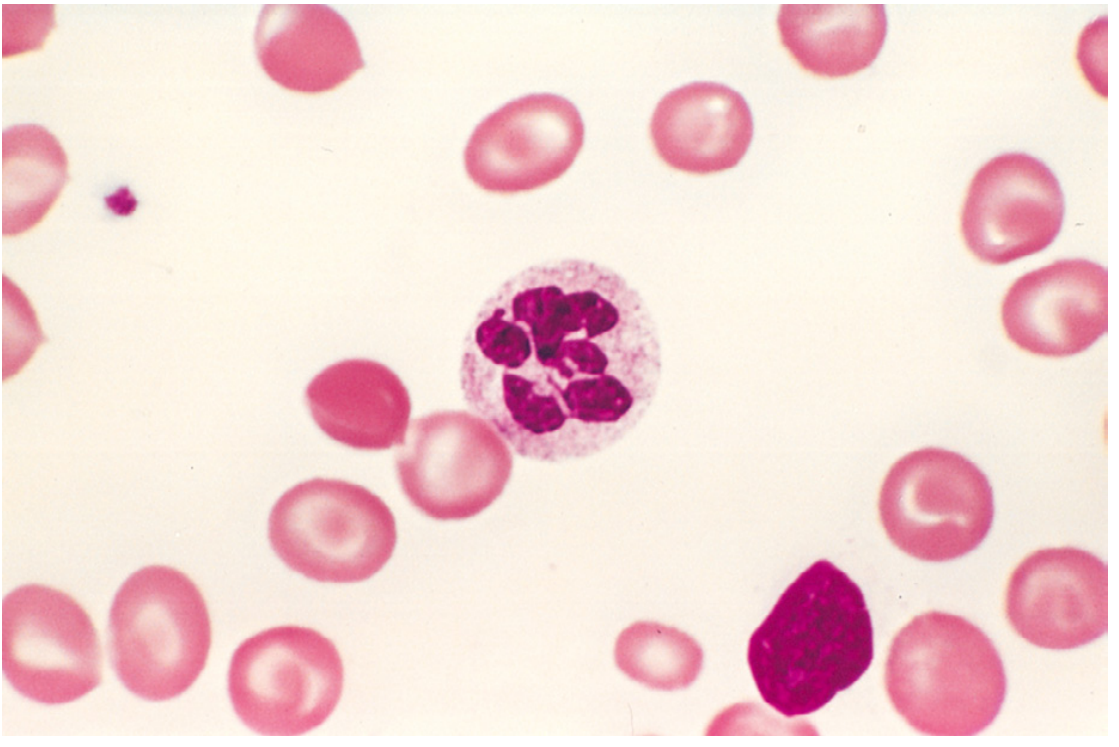
Fig: Hypersegmented neutrophil (center) - the hallmark finding on peripheral smear. Notice the large oval red cells around it.
Bone Marrow:
- Hypercellular marrow (looks busy - lots of precursors)
- Megaloblasts at all stages - large cells with fine, open nuclear chromatin but hemoglobinized cytoplasm (this nuclear-cytoplasmic asynchrony is key!)
- Giant metamyelocytes and band forms
- Abnormally large megakaryocytes with bizarre multilobate nuclei
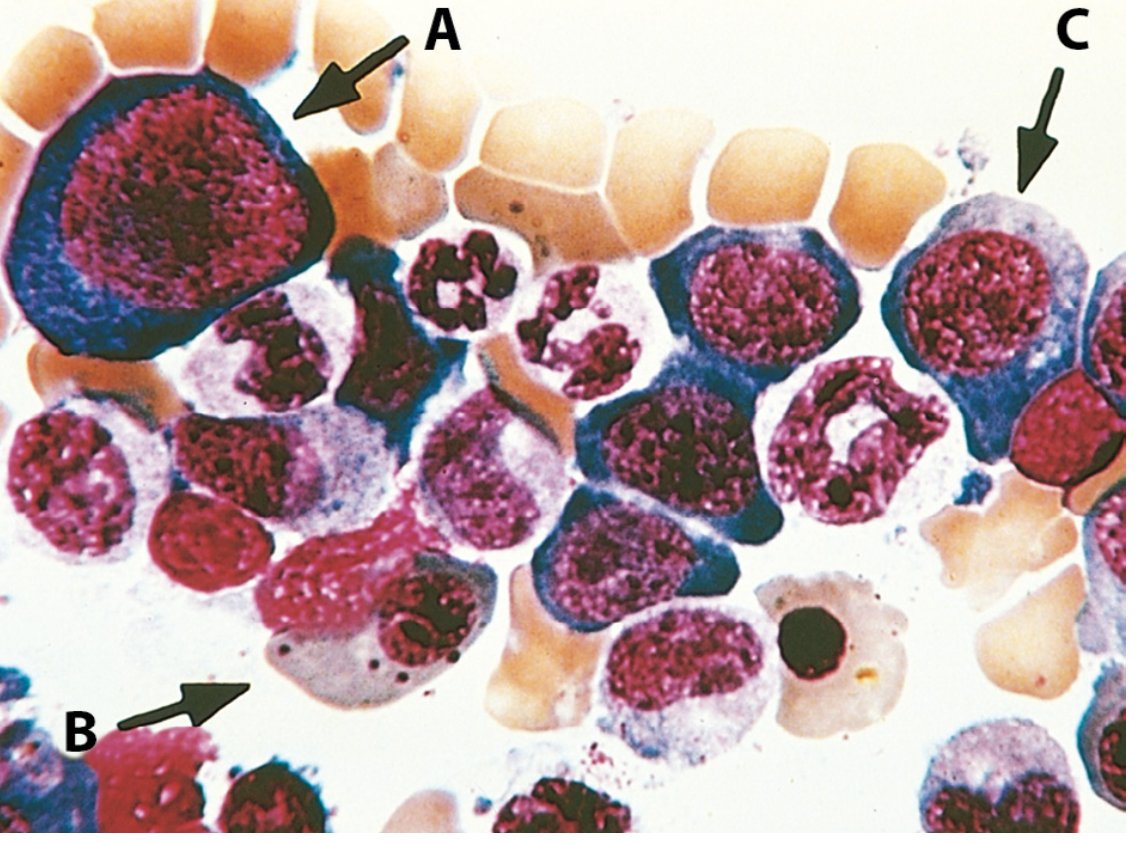
Fig: Bone marrow - (A) early megaloblast with deeply blue cytoplasm and fine nuclear chromatin, (B) orthochromatic megaloblast - hemoglobinized but nucleus NOT pyknotic (key difference from normal!), (C) another erythroid precursor.
5. Pernicious Anemia - The MOST IMPORTANT Subtype
Pernicious anemia = Vitamin B12 deficiency due to autoimmune destruction of parietal cells
Mechanism:
Parietal cells in stomach → make INTRINSIC FACTOR (IF)
↓
Autoantibodies attack parietal cells
↓
No intrinsic factor
↓
B12 cannot be absorbed in terminal ileum
↓
B12 deficiency → Megaloblastic anemia
What the Autoantibodies Attack (know all 3 types):
- Anti-parietal cell antibodies - against parietal cells themselves (most common, ~90%)
- Type I antibody - blocks IF binding to B12
- Type II antibody - blocks IF-B12 complex from binding to ileal receptor
Gastric Changes in Pernicious Anemia:
- Chronic atrophic gastritis - affects body and fundus
- Loss of parietal cells (no IF, no acid) and chief cells (no pepsinogen)
- Intestinal metaplasia of mucosa
- Lymphocytic and plasma cell infiltration
Clinical Features:
- Anemia symptoms: weakness, fatigue, pallor
- Lemon-yellow tinge to skin (pallor + mild jaundice from ineffective erythropoiesis)
- Atrophic glossitis (beefy red, smooth tongue)
- NEUROLOGIC damage (B12 ONLY, NOT folate!) - subacute combined degeneration of spinal cord:
- Posterior columns - loss of vibration sense, position sense
- Lateral corticospinal tracts - weakness, spasticity
- Peripheral nerves - peripheral neuropathy
Exam Trap: Folate deficiency looks identical to B12 deficiency on blood smear BUT does NOT cause neurologic damage. If a question says "patient has megaloblastic anemia AND neurological symptoms" → answer is B12 deficiency / Pernicious anemia.
6. Folate Deficiency - Key Points
- Blood picture = identical to B12 deficiency (same morphology)
- NO neurologic symptoms (key difference!)
- Diagnosis: decreased serum or red cell folate levels
- Most common cause: poor diet + alcoholism
- Also seen in pregnancy (increased demand - that's why folate supplements are given in pregnancy)
7. Lab Findings Summary Table
| Lab Test | Result |
|---|---|
| MCV (mean cell volume) | HIGH (macrocytic) |
| Peripheral smear | Macro-ovalocytes, hypersegmented neutrophils |
| Reticulocyte count | LOW |
| Serum B12 | Low (in B12 deficiency) |
| Serum folate / RBC folate | Low (in folate deficiency) |
| LDH | HIGH (due to ineffective erythropoiesis - cells dying) |
| Indirect bilirubin | Mildly HIGH (cell breakdown) |
| Bone marrow | Hypercellular with megaloblasts |
8. Key Concepts Summary (Perfect for Last-Minute Revision)
| Point | Detail |
|---|---|
| Core mechanism | Impaired DNA synthesis → nuclear maturation arrest |
| Key word | Nuclear-cytoplasmic asynchrony |
| Two main causes | B12 deficiency + Folate deficiency |
| Most important B12 cause | Pernicious anemia (autoimmune) |
| Most important folate cause | Poor diet, alcoholism, pregnancy |
| Hallmark blood smear finding | Macro-ovalocytes + hypersegmented neutrophils |
| Bone marrow | Hypercellular + megaloblasts |
| B12 ONLY feature | Neurologic damage (subacute combined degeneration) |
| Diagnosis pernicious anemia | Anti-parietal cell antibodies, anti-IF antibodies |
| Treatment | B12 injections (pernicious anemia), oral folate |
9. Exam One-Liners to Memorize
- "Megaloblastic = DNA problem, not hemoglobin problem" (big cells but still make hemoglobin)
- "Nucleus stays baby, cytoplasm grows up" = nuclear-cytoplasmic asynchrony
- "Hypersegmented neutrophil = megaloblastic anemia until proven otherwise"
- "B12 deficiency + neuro symptoms = pernicious anemia"
- "Folate = no neuro"
- "Bone marrow looks busy but works poorly" = ineffective hematopoiesis
10. Quick Mnemonics
Causes of B12 deficiency → "I AM BLIND"
- Intrinsic factor absent (pernicious anemia)
- Alcohol
- Malabsorption (Crohn's, ileal resection)
- Bacterial overgrowth
- Low diet (vegetarians)
- Ileal disease
- Nitrous oxide (drug - inactivates B12)
- Diphyllobothrium (fish tapeworm)
Features of Pernicious Anemia → "PLAN"
- Parietal cell antibodies (autoimmune)
- Lemon-yellow skin
- Atrophic glossitis + Atrophic gastritis
- Neurological damage (subacute combined degeneration)
This covers everything you need from Robbins for a university pathology exam. The highest-yield points for examiners are: (1) nuclear-cytoplasmic asynchrony, (2) hypersegmented neutrophils, (3) B12 vs folate - neurological distinction, and (4) pernicious anemia mechanism with autoantibodies.
This is a shared conversation. Sign in to Orris to start your own chat.