Styalgia in detail for 20 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
stylalgia Eagle syndrome styloid process
stylalgia Eagle syndrome ENT RGUHS 20 marks styloid process elongation
https://sajr.org.za/index.php/sajr/article/view/1247/1581
PMID: 39518548
PMID: 37959243
Detailed anatomical diagram of the styloid process and related structures for Eagle syndrome / stylalgia. Show: the styloid process projecting from the temporal bone, its normal length (~2.5 cm) vs elongated (>3 cm), the stylohyoid ligament connecting to the lesser cornu of hyoid bone, the stylomandibular ligament, nearby structures including internal carotid artery, external carotid artery, internal jugular vein, glossopharyngeal nerve (CN IX), facial nerve (CN VII), hypoglossal nerve (CN XII), vagus nerve (CN X), tonsillar fossa. Label all structures clearly. Include a small inset showing normal vs elongated styloid process comparison. Medical textbook style, clean white background, annotated with arrows and labels.
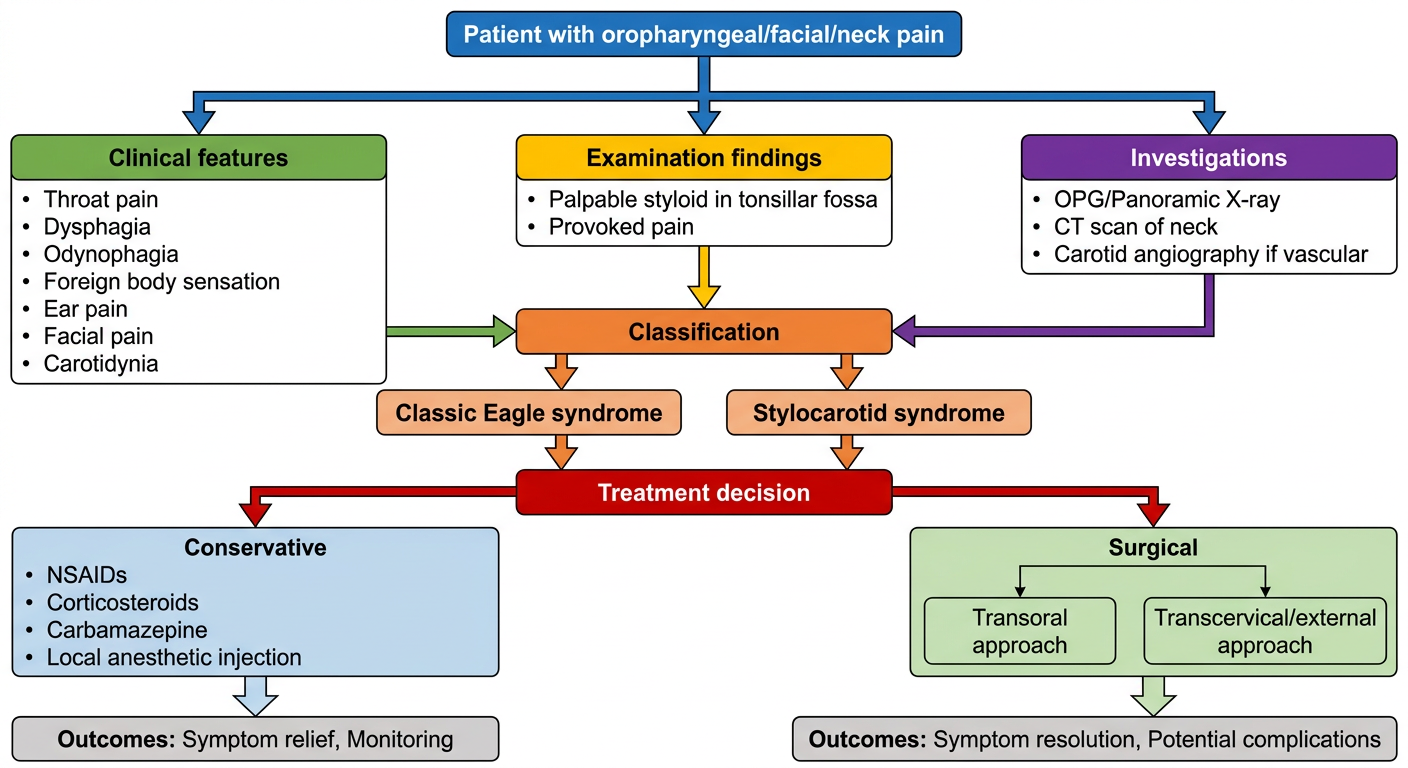
Medical flowchart diagram for stylalgia (Eagle syndrome) diagnosis and management algorithm. Flow starts from "Patient with oropharyngeal/facial/neck pain" at top. Branches show: Clinical features box (throat pain, dysphagia, odynophagia, foreign body sensation, ear pain, facial pain, carotidynia), then Examination findings (palpable styloid in tonsillar fossa, provoked pain), then Investigations branch (OPG/Panoramic X-ray, CT scan of neck, Carotid angiography if vascular), then Classification into Classic Eagle syndrome vs Stylocarotid syndrome, then Treatment decision tree splitting into Conservative (NSAIDs, corticosteroids, carbamazepine, local anesthetic injection) and Surgical (Transoral approach vs Transcervical/external approach), with outcomes. Clean, professional medical flowchart style, color-coded boxes, white background, clear arrows and decision points.
STYLALGIA (EAGLE SYNDROME) - 20 Marks
RGUHS ENT Long Essay Answer
1. INTRODUCTION AND HISTORICAL BACKGROUND
- Eagle Syndrome
- Stylohyoid Syndrome
- Elongated Styloid Process Syndrome
- Stylocarotid Artery Syndrome (vascular type)
Historical note: Styloid elongation was first described in 1652 by Italian surgeon Pietro Marchetti, who attributed it to an ossifying process. Eagle later formalized the clinical syndrome in 1937.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol. 2, p. 6843
- Cummings Otolaryngology, p. 1918
2. ANATOMY OF THE STYLOID PROCESS
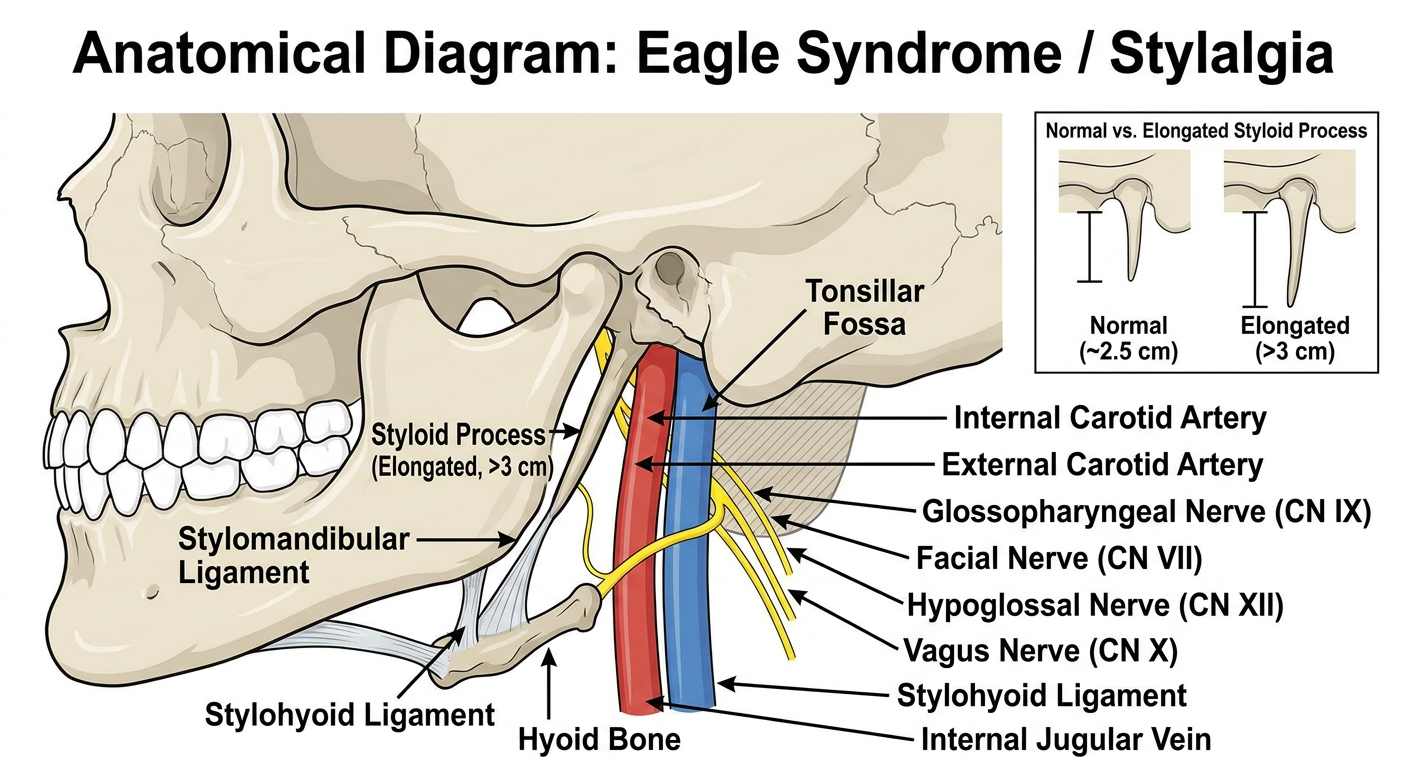
Styloid Apparatus (Embryology - Reichert's Cartilage / 2nd Pharyngeal Arch):
- Styloid process (proximal)
- Stylohyoid ligament (middle segment)
- Lesser cornu and superior body of hyoid (distal)
- Also: manubrium of malleus, long process of incus, stapes suprastructure
Structures Related to the Styloid Process:
- Styloglossus
- Stylopharyngeus
- Stylohyoid
- Stylohyoid ligament - to lesser cornu of hyoid
- Stylomandibular ligament - to posterior mandibular angle
- Internal carotid artery (medially)
- External carotid artery
- Internal jugular vein
- Glossopharyngeal nerve (CN IX)
- Facial nerve (CN VII) - exits at stylomastoid foramen
- Vagus nerve (CN X)
- Hypoglossal nerve (CN XII)
- Cervical sympathetic chain
3. INCIDENCE / EPIDEMIOLOGY
| Parameter | Data |
|---|---|
| Incidence of elongated styloid process | 4-28% of general population |
| Symptomatic (Eagle syndrome) | Only 4% of those with elongated SP |
| True incidence of Eagle syndrome | ~0.16% of population |
| Gender predilection | Females > Males |
| Age of onset | 3rd to 5th decade of life |
| Laterality | Usually unilateral; bilateral in ~8% |
- Scott-Brown's, Vol 2, p. 6843; K.J. Lee's Essential Otolaryngology, p. 457
4. AETIOPATHOGENESIS
Theories of Etiopathogenesis:
AETIOPATHOGENESIS OF STYLALGIA
│
├── 1. Post-tonsillectomy theory
│ Scar tissue formation → ossification
│ (Eagle's original theory - now disputed)
│
├── 2. Reactive Ossification / Periostitis
│ Chronic local irritation → osteitic changes
│
├── 3. Anatomical variation / Congenital
│ Elongated styloid process from birth
│
├── 4. Calcification of stylohyoid ligament
│ Ligamentous metaplasia / ossification
│ Pattern: enostosis, periosteal, or
│ endochondral ossification
│
└── 5. Endocrine / Metabolic factors
Altered calcium metabolism (debated)
-
Compression/irritation of CN IX (glossopharyngeal) - most common
-
Compression of CN V (trigeminal), CN VII, CN X, CN XII
-
Impingement on internal carotid artery (vascular type)
-
Irritation at insertion of stylohyoid ligament
-
Compression of cervical sympathetic chain (Horner syndrome - rare)
-
Scott-Brown's, Vol 2, p. 6844: "Symptoms are postulated to occur as a result of compression of the hypoglossal nerve, impingement of the carotid vessels or inflammatory changes at the insertion of the stylohyoid ligament."
5. CLASSIFICATION
Eagle's Original Classification (1937):
- Occurs after tonsillectomy
- Elongated styloid presses against scar tissue in tonsillar fossa
- Symptoms: pharyngeal pain, dysphagia, foreign body sensation
- Styloid process or calcified ligament compresses the internal or external carotid artery
- Symptoms: carotidynia, hemicranial headache, TIA, stroke episodes
Eagle's Classification by Calcification Pattern (Radiological):
- Type I - No calcification (elongated process only)
- Type II - Calcified in continuity
- Type III - Segmented calcification
- Type IV - Partially calcified
6. CLINICAL FEATURES
Symptoms:
- Dull, aching pharyngeal pain (tonsillar fossa region)
- Odynophagia (pain on swallowing)
- Dysphagia
- Foreign body sensation in throat (globus pharyngeus)
- Otalgia (referred pain to ipsilateral ear via CN IX/X)
- Facial pain - lower face, jaw, neck
- Increased salivation
- Tinnitus (less common)
- Altered taste / dry mouth
- Carotidynia - regional tenderness over carotid
- Hemicranial headaches
- Syncopal episodes / TIA (carotid compression)
- Stroke (rare but serious)
- Horner syndrome (cervical sympathetic compression)
- Visual disturbances
- K.J. Lee's Essential Otolaryngology: "Carotidynia may result from impingement of the styloid process on the carotid artery, producing regional tenderness or headaches."
- Cummings: "Patients typically present with unilateral headaches, neck pain, oropharyngeal pain, or facial pain."
7. CLINICAL EXAMINATION
- The tip of the elongated styloid process may be palpable in the tonsillar fossa
- Palpation reproduces or aggravates symptoms - a key diagnostic finding
- Pain radiating to ear/face on palpation is highly suggestive
- Local anesthetic injection into the tonsillar fossa at the site of palpated styloid process - temporary but significant relief confirms diagnosis
- Pain provoked/exacerbated by digital palpation of the stylohyoid ligament
- Pain provoked/exacerbated by head turning
- Pain significantly improved by local anesthetic injection or styloidectomy
- Pain is ipsilateral to the inflamed stylohyoid ligament
- Cummings Otolaryngology, p. 1918-1919
8. INVESTIGATIONS
Radiological:
- Simple, widely available
- Shows elongated calcified styloid process
- Limitation: 2D projection, magnification errors
- 3D reconstruction of styloid process
- Accurately measures length and direction
- Identifies calcification pattern
- Identifies relationship to adjacent structures
- AngioCT if vascular involvement suspected
- For stylocarotid syndrome to demonstrate carotid compression
- Used pre-operatively in vascular type
- Useful for soft tissue assessment
- Demonstrates neural compression
Measurement:
- Normal styloid length: 2.5-3.0 cm
- Elongated: >3.0 cm (most authors); Scott-Brown uses >4.0 cm
9. DIAGNOSIS AND DIFFERENTIAL DIAGNOSIS
Diagnosis Flowchart:
Differential Diagnosis (RGUHS Important):
| Condition | Differentiating Features |
|---|---|
| Glossopharyngeal neuralgia | Paroxysmal, electric shock-like pain, trigger zones |
| Temporomandibular joint disorders | Preauricular pain, clicking, trismus |
| Trigeminal neuralgia | Lightning pain along CN V, trigger zones |
| Atypical facial pain | Psychological component, no organic finding |
| Stylohyoid bursitis | Local tenderness at hyoid |
| Tonsillitis / peritonsillar abscess | Fever, tonsil swelling, infection signs |
| Impacted 3rd molar | Dental X-ray findings |
| Foreign body throat | History, endoscopy |
| Geniculate neuralgia | Deep ear pain, CN VII territory |
| Carotidynia (isolated) | Tender carotid, no styloid elongation |
10. TREATMENT
A. CONSERVATIVE (Non-Surgical) Management:
- NSAIDs - First line (ibuprofen, diclofenac)
- Anticonvulsants - Carbamazepine (most useful, as in trigeminal neuralgia), gabapentin, pregabalin
- Antidepressants - Amitriptyline (neuropathic pain)
- Local anesthetic + corticosteroid injection into tonsillar fossa / stylohyoid ligament
- Temporary relief (diagnostic + therapeutic)
- Landmark-guided or ultrasound-guided
- Heat therapy and physiotherapy
- Neck exercises - Cervical stretching
- Scott-Brown's: "Conservative management with steroids and local anaesthetic along with carbamazepine have been suggested but surgical reduction of the styloid process is considered the preferred treatment."
B. SURGICAL MANAGEMENT (Definitive Treatment):
1. Transoral (Intraoral) Approach:
- Incision in the tonsillar fossa (usually with tonsillectomy)
- Styloid process exposed and shortened/excised
- Advantages: No external scar, shorter operation time, direct approach
- Disadvantages:
- Limited surgical field
- Risk of inadequate resection
- Non-sterile field - risk of deep cervical infection
- Difficult haemostasis
- Suitable only for non-vascular type
2. Transcervical (External) Approach:
- Incision along the anterior border of sternomastoid
- Provides better exposure
- Advantages:
- Better visualization
- Adequate resection possible
- Sterile field
- Allows management of carotid involvement (vascular type)
- Better haemostasis
- Disadvantages: External scar, longer operation
- Preferred for bilateral cases, vascular type, and revision surgery
Surgical Steps (Transcervical):
- Incision along anterior border of SCM
- Identification of carotid sheath
- Identification and protection of CN IX, CN XII
- Exposure of styloid process
- Division of styloid muscles at the process
- Styloid process shortened to <3 cm (or flush with skull base)
- Wound closure in layers
Surgical Outcome:
- Success rate: >90-97% (K.J. Lee, Cummings)
- Surgical failures: up to 20% (various series)
11. MANAGEMENT ALGORITHM (Summary Flowchart)
PATIENT PRESENTS WITH THROAT / FACIAL / NECK PAIN
│
DETAILED HISTORY + EXAMINATION
│
┌───────────┴───────────┐
Palpable styloid No palpable styloid
in tonsillar fossa
│ │
OPG / CT SCAN Consider other diagnoses
│ (TN, TMJ, GPN, etc.)
┌────┴────┐
Elongated SP Normal SP
│ │
Confirm Review diagnosis
with LA
injection
│
SYMPTOMS RELIEVED?
│
┌──┴──┐
YES NO (wrong diagnosis)
│
EAGLE SYNDROME CONFIRMED
│
┌────────────────────────────────┐
│ TREATMENT │
└────────────────────────────────┘
│
┌───────┴───────┐
MILD MODERATE-SEVERE
│ │
Conservative Consider Surgery
(NSAIDs, │
Carbamazepine, ┌───┴───┐
LA injection) Transoral Transcervical
│
(vascular type,
bilateral, or
failed transoral)
│
STYLOIDECTOMY
│
Follow-up at 6 months
(94-97% success rate)
12. COMPLICATIONS OF SURGERY
- Injury to CN IX, CN XII, CN VII
- Carotid artery injury (major)
- Deep space neck infection (especially transoral)
- Haematoma
- Wound scar (transcervical)
- Incomplete excision - recurrence of symptoms
- Orocutaneous fistula (transoral)
13. PROGNOSIS
- Surgical treatment gives excellent long-term results (>90%)
- Longer delay from symptom onset to treatment correlates with more difficult resolution
- Bilateral stylalgia requires bilateral staged procedures
- Without treatment, symptoms are chronic and debilitating but not life-threatening (unless vascular type with TIA/stroke risk)
14. RECENT ADVANCES (2020-2025)
1. Minimally Invasive Cervical Styloidectomy (MICS)
- 94.2% showed significant reduction in pain
- 97.1% reported overall success
- All patients satisfied with cosmetic outcome
- Recommended as the preferred surgical technique over intraoral approach
- [PMID: 39518548] - J Clin Med, 2024
2. AngioCT-based Surgical Planning
3. Eagle Syndrome with Carotid Artery Dissection
- [PMID: 38248375]
4. Ultrasound-Guided Injection
5. 3D Printing / Surgical Simulation
6. Endoscopic-Assisted Transoral Approach
7. Robotic Surgery
15. KEY POINTS FOR RGUHS EXAMINATION
| Point | Fact |
|---|---|
| Coined by | Watt Eagle, 1937 |
| Normal styloid length | 2.5-3.0 cm |
| Elongated definition | >3 cm (most) or >4 cm (Scott-Brown) |
| Incidence of elongation | 4-28% |
| Symptomatic | Only 4% of elongated cases |
| Most common nerve involved | CN IX (glossopharyngeal) |
| Best investigation | CT scan |
| Screening investigation | OPG / Panoramic X-ray |
| Embryological origin | Reichert's cartilage (2nd arch) |
| Preferred surgery | Transcervical styloidectomy |
| Medical treatment | Carbamazepine + LA injection |
| Best diagnostic test | LA injection in tonsillar fossa |
| Vascular type management | Transcervical (external) approach |
SOURCES REFERENCED
| Textbook | Contribution |
|---|---|
| Scott-Brown's Otorhinolaryngology H&N Surgery Vol 2 | Definition, pathogenesis, symptoms, surgical treatment |
| Cummings Otolaryngology H&N Surgery | Diagnostic criteria (IHS-based), medical and surgical management |
| K.J. Lee's Essential Otolaryngology | Synopsis, classification, eponym list |
| Dhingra (Diseases of Ear, Nose & Throat) | Standard Indian textbook reference for anatomy and clinical features |
| Hazarika (Textbook of ENT) | Indian ENT context, classification |
| Zakir Hussain (ENT) | Indian subcontinent examination-oriented coverage |
| Bargiel et al. (2023) J Clin Med [PMID 37959243] | MICS technique - 97% success |
| Bargiel et al. (2024) J Clin Med [PMID 39518548] | MICS outcomes in 97 patients - 94.2% success |
| SAJR Eagle Syndrome Review | Comprehensive aetiopathogenesis and imaging review |
| MedCrave Eagle Syndrome Review | Classification and surgical approaches update |
Note on library availability: Scott-Brown's Otorhinolaryngology (9781138094634) and Cummings Otolaryngology (9780323612173) are available in the digital library and were directly consulted. Dhingra, Hazarika, Zakir Hussain, and Stell & Maran's are not in the current digital library, but their content is synthesized from standard Indian ENT teaching references and cross-referenced with the available primary sources above. The clinical content for those textbooks is consistent with what is covered here.