U are best pharmacy professor in world more than 50 years of experience in working top institutions like Harvard , Monash , Oxford . Now u need to answer all the learning objectives with tabulate form for section b( SAQ and LAQ)list all important bold keywords in details on there . Give me easy memory trick to remember these for my exam . Make easy understandable those topics to the students to understand it like pro and can answer any questions related to that in exam .
cd /home/daytona/workspace/attachments/dbca5d55-aea7-483b-bf34-649d8f4870dc/ && python3 -c " from pypdf import PdfReader reader = PdfReader('MASRO - PHAR1612 SKIN DISORDERS - MICROBIOLOGY OF INFECTIOUS SKIN DISEASES.pdf') print(f'Total pages: {len(reader.pages)}') for i, page in enumerate(reader.pages): print(f'--- PAGE {i+1} ---') print(page.extract_text()) print() "
🎓 PHAR1612 - MICROBIOLOGY OF INFECTIOUS SKIN DISEASES
Complete SAQ & LAQ Study Guide | Section B
📋 LEARNING OBJECTIVES OVERVIEW
- Normal skin microbiome
- Portal of entry for microorganisms
- Bacterial skin infections
- Viral skin infections
- Fungal skin infections
- Parasitic skin infections
🧫 SECTION 1: SKIN MICROBIOME
Master Table
| Keyword | Detail | Exam Importance |
|---|---|---|
| Parturition | Childbirth - how we first acquire skin microbiome from mother | Foundation concept |
| Vaginal childbirth | Newborn colonized with Lactobacillus spp. | SAQ: "how does delivery method affect microbiome?" |
| Caesarean birth | Colonized with mother's skin microbiome instead | Compare/contrast |
| Resident microorganisms | = Core microbiome - permanent, beneficial colonizers | Define in SAQ |
| Transient microorganisms | = "Tourists" - temporary, picked up from environment/lifestyle | Define in SAQ |
| Actinobacteria | Most abundant phylum on skin | Most abundant = exam favourite |
| Firmicutes | Second most abundant phylum | List the 4 phyla |
| Proteobacteria | Third most abundant phylum | |
| Bacteroidetes | Fourth most abundant phylum | |
| Corynebacteria | Most common bacterial genus | Top 3 genera |
| Propionibacteria | Second most common genus | |
| Staphylococci | Third most common genus | |
| Malassezia spp. | Normal skin yeast | Can cause Pityriasis versicolor when overgrows |
| Demodex spp. | Normal parasitic arthropod mite | Lives in hair follicles |
🧠 Memory Trick #1 - The 4 Phyla: "A FiPrBa"
Actinobacteria → Firmicutes → Proteobacteria → Bacteroidetes Say it: "A FiFi Protects Bacteria"
🧠 Memory Trick #2 - The 3 Common Genera: "CPS"
Corynebacteria → Propionibacteria → Staphylococci Say: "Clever Pharmacy Students" (that's you!)
🧠 Memory Trick #3 - Delivery Type → Microbiome
Vaginal = Vitamin L (Lactobacillus) - the good gut bugs C-section = Copied from mother's Cutaneous (skin) bugs
🦠 SECTION 2: BACTERIAL SKIN INFECTIONS
Master Table - Impetigo
| Keyword | Detail | Exam Focus |
|---|---|---|
| Impetigo | Highly contagious superficial bacterial skin infection | Common SAQ topic |
| Golden crust | Classic hallmark sign - honey-colored crusted lesions | Clinical feature SAQ |
| Bullous impetigo | Variant forming large fluid-filled blisters (bullae) | Distinguish from non-bullous |
| Staphylococcus aureus | Primary causative agent | Most important organism |
| Streptococcus pyogenes | Secondary causative agent | Group A Strep |
| Topical: Fusidic acid | First-line topical antibiotic treatment | Treatment SAQ |
| Topical: Retapamulin | Alternative topical treatment | |
| Oral: Flucloxacillin | First-line oral antibiotic (anti-staphylococcal penicillin) | |
| Oral: Penicillin | Used for streptococcal coverage | |
| Oral: Erythromycin | Macrolide - used if penicillin allergy | |
| May complicate eczema | Eczema skin barrier damage = portal of entry | Risk factor |
Master Table - Cellulitis
| Keyword | Detail | Exam Focus |
|---|---|---|
| Cellulitis | Bacterial infection of skin AND deeper tissues (dermis + subcutaneous) | LAQ topic |
| Erysipelas | Superficial form, more sharply demarcated, involves upper dermis/lymphatics | Distinguish from cellulitis |
| Commonest site | Legs | Easy mark |
| Streptococcus pyogenes | Causes 2/3 of cellulitis cases | Most important organism |
| Staphylococcus aureus | Second most common cause | |
| Redness (erythema) | Classic sign | Clinical features |
| Swelling (oedema) | Classic sign | |
| Increased warmth | Classic sign | |
| Tenderness | Classic sign | |
| Blistering | Advanced sign | |
| Abscess | Complication | |
| Systemic symptoms | Fever + malaise = systemic spread | LAQ: why IV antibiotics? |
| Predisposing factors | Venous disease, diabetes, obesity, alcoholism, tinea pedis, eczema, trauma, pregnancy, prior cellulitis | BIG LAQ topic |
| Tinea pedis | Fungal foot infection = breaks skin barrier = entry portal for cellulitis | Interconnection concept |
| Oral or IV Penicillin | First-line treatment | Treatment SAQ |
| Erythromycin | Alternative if penicillin allergy | |
| Treat underlying factor | Key management principle - not just antibiotics alone | Exam favourite instruction |
🧠 Memory Trick #4 - Cellulitis Signs: "RSWT-BAU"
Redness → Swelling → Warmth → Tenderness → Blistering → Abscess → Ulceration Say: "Red Swollen Wounds Take Bacteria And Ulcerate"
🧠 Memory Trick #5 - Cellulitis Predisposing Factors: "VODATOP"
Venous disease → Obesity → Diabetes → Alcoholism → Trauma/surgery → Old episode of cellulitis → Pregnancy + tinea Pedis Say: "VODATOP is a cocktail for infection"
🧠 Memory Trick #6 - Impetigo vs Cellulitis at a glance
| Feature | Impetigo | Cellulitis |
|---|---|---|
| Depth | Superficial (epidermis) | Deep (dermis + subcutaneous) |
| Main Bug | Staph aureus | Strep pyogenes |
| Classic Sign | Golden crust | Redness + warmth + systemic fever |
| Contagious? | YES, highly | Less so |
| Treatment | Topical fusidic acid / oral flucloxacillin | Oral/IV penicillin |
🦟 SECTION 3: VIRAL SKIN INFECTIONS
Master Table - Herpes Simplex Virus (HSV)
| Keyword | Detail | Exam Focus |
|---|---|---|
| HSV Type 1 | Most common type - causes oral/labial herpes | SAQ: which type is commonest |
| Herpes labialis | Cold sores on lips - recurrent form of HSV-1 | Clinical manifestation |
| Stomatogingivitis | Primary HSV-1 infection - mouth/gum inflammation (often mild) | Primary episode |
| Prodrome | Warning symptom = burning/tingling sensation BEFORE lesion appears | Classic exam question |
| Vesicles | Small fluid-filled blisters - classic lesion type | Morphology |
| Crusting | Vesicles dry and crust over | Healing phase |
| Self-limiting | Resolves without treatment in immunocompetent | Key concept |
| Eczema herpeticum | Dangerous complication - HSV spreads widely over eczematous skin | EMERGENCY - refer immediately |
| Aciclovir | Antiviral treatment - topical for mild, oral for severe/recurrent | Treatment |
| Long-term aciclovir | For recurrent episodes (prophylaxis) | Chronic management |
Master Table - Herpes Zoster (Shingles)
| Keyword | Detail | Exam Focus |
|---|---|---|
| Reactivation | Varicella-zoster virus (VZV) dormant in dorsal root ganglia, reactivates | Core mechanism - LAQ |
| Chicken pox (Varicella) | PRIMARY infection - virus then stays latent | Distinguish primary vs reactivation |
| Elderly + immunocompromised | High-risk groups for reactivation | Risk factors |
| Dermatomal pattern | Rash follows a single dermatome/nerve distribution - does NOT cross midline | Classic clinical sign |
| Pain precedes rash | By 1-3 days - prodromal pain/burning before vesicles appear | Very common SAQ |
| Crops of blisters | Vesicular rash in dermatomal pattern | Clinical feature |
| Commonest sites | Chest, neck, forehead | Sites |
| Slow healing in elderly | Important clinical caveat | |
| Post-herpetic neuralgia (PHN) | Most important complication - persistent nerve pain after rash resolves | LAQ: complication |
| Virus in vesicles | Fluid in blisters is infectious (risk of chickenpox to susceptible contacts) | Transmission |
| Antivirals orally (if early) | Start ASAP - aciclovir/valaciclovir - reduces duration and prevents PHN | Treatment principle |
| Topical antiseptics | Secondary bacterial infection prevention | |
| Pain relief | Analgesics for PHN - NSAIDs, tricyclics, gabapentin |
Master Table - Human Papillomavirus (HPV)
| Keyword | Detail | Exam Focus |
|---|---|---|
| HPV | Causes warts (verrucae) on skin | Common, often SAQ |
| Very common | 12% in 4-6 yr olds, 4.9% in 16 yr olds | Epidemiology |
| Self-limiting | Warts resolve spontaneously - 93% of 11-yr-olds with warts clear by 16 | Key management concept |
| Occupational risk | Commoner in butchers and abattoir (slaughterhouse) workers | Occupational exposure |
| Contagious | Spread through direct contact | Transmission |
🧠 Memory Trick #7 - HSV vs HZV key differences:
| Feature | HSV | HZV (Shingles) |
|---|---|---|
| Primary infection | Oral/genital herpes | Chickenpox |
| Mechanism | New infection OR reactivation | Always REactivation of dormant VZV |
| Distribution | Localized | Dermatomal - one side only |
| Key complication | Eczema herpeticum | Post-herpetic neuralgia |
| Treatment | Aciclovir | Antivirals EARLY + pain relief |
🧠 Memory Trick #8 - Shingles Sequence: "PDRP"
Pain first → Dermatome rash (1-3 days later) → Resolution (slow in elderly) → PHN risk Say: "Pain Does Really Persist"
🍄 SECTION 4: FUNGAL SKIN INFECTIONS
Master Table - Dermatophytes (Tinea)
| Keyword | Detail | Exam Focus |
|---|---|---|
| Dermatophytes | Fungi that infect keratinized tissue (skin, hair, nails) | Definition |
| Tinea | General term for dermatophyte infection | Latin for "gnawing worm" |
| Tinea corporis | Body ringworm | Location memory |
| Tinea cruris | Groin - "jock itch" | Location memory |
| Tinea pedis | Feet - "athlete's foot" | Most common |
| Tinea capitis | Scalp ringworm | Children mainly |
| Tinea unguium (Onychomycosis) | Nail fungal infection - "onycho" = nail | Common in elderly |
| Annular/ringed lesion | Classic ring shape with central clearing | Classic SAQ sign |
| Central sparing | Inside of ring appears clear/normal | Clinical sign |
| Asymmetrical | Not bilateral/symmetric | Clinical sign |
| Scaly + pruritic | Scaly, itchy lesion | Symptoms |
| Trichophyton tonsurans | Main causative organism for Tinea capitis | Organism SAQ |
| Skin scraping for mycology | Diagnostic method | Investigation |
| Topical imidazole | E.g. clotrimazole - first-line for most tinea | Treatment |
| Daktacort | Imidazole + steroid combination | Specific product |
| Terbinafine | Oral antifungal - gold standard for Tinea capitis (12 weeks) and Tinea unguium (12 weeks) | LAQ: treatment |
| Amorolfine nail paint | Topical option for onychomycosis (relatively ineffective) | |
| Reservoir for recurrent infection | Onychomycosis in nails acts as reservoir | Concept |
Master Table - Candida & Pityriasis Versicolor
| Keyword | Detail | Exam Focus |
|---|---|---|
| Candida spp. | Yeast causing opportunistic infections in moist areas | SAQ |
| Nappy rash | Common cause in infants | Candida clinical |
| Candidal vulvitis | Vaginal thrush - pruritic | Clinical |
| Satellite lesions | Small lesions beyond main lesion border - pathognomonic of Candida | Classic exam sign |
| Imidazole creams | Treatment for Candida (clotrimazole, miconazole) | Treatment |
| Pityriasis versicolor | Caused by Malassezia spp. - normal yeast gone rogue | |
| Common in young adults | Epidemiology of pityriasis versicolor | |
| Hypopigmented macules | Classic presentation - pale patches | Classic clinical |
| Scaly erythematous macules | Also can present as scaly red patches | Clinical |
| Slow progression | Pityriasis versicolor is chronic | |
| Itraconazole 200mg x 1 week | Oral treatment for pityriasis versicolor | Specific dose = high-yield |
| Ketoconazole shampoo | Topical treatment for pityriasis versicolor | |
| May recur | Common recurrence | Management point |
| Intertrigo | Rash in body folds (intertriginous areas) - moist environment | SAQ |
| Bacteria + yeast thrive | Why body folds are infected | Mechanism |
| Treat underlying cause | Management principle for intertrigo |
Master Table - Mycoses Classification
| Type | Location | Example |
|---|---|---|
| Superficial/Cutaneous mycoses | Epidermis, hair, nails | Tinea, onychomycosis |
| Subcutaneous mycoses | Deeper epidermis + dermis | Sporotrichosis |
| Systemic mycoses | Multiple body systems | Candidiasis (invasive) |
🧠 Memory Trick #9 - Tinea Locations: "Corpus Cruris Pedis Capitis Unguium"
Corpus = Chest/body Cruris = Crotch/groin Pedis = Peds/feet Capitis = Cap on head/scalp Unguium = Under/inside nail
🧠 Memory Trick #10 - Satellite lesions = Candida
Think: "Candida sends out satellites!" - baby lesions orbiting the main one
🧠 Memory Trick #11 - Pityriasis Versicolor vs Tinea
Pityriasis = "Patchy, pale, young adult" - hypoPIGmented Tinea corporis = "Ring with central clearing" - annular
🕷️ SECTION 5: PARASITIC SKIN INFECTIONS
Master Table - Scabies
| Keyword | Detail | Exam Focus |
|---|---|---|
| Sarcoptes scabiei var. hominis | Causative organism - human itch mite | Organism identification LAQ |
| Microscopic mite | Cannot be seen with naked eye | Description |
| Burrows into stratum corneum | Female mite burrows to lay eggs | Pathogenesis - key |
| Female mites | Lay eggs in burrows in stratum corneum | Specifically females |
| Eggs hatch in 3-4 days | Life cycle | Pathogenesis |
| ~200 million cases annually | Global burden - very common | Epidemiology |
| Crowded environments | Nursing homes, prisons, childcare, refugee camps | Risk factors |
| Prolonged skin-to-skin contact | Primary mode of transmission | Transmission |
| Sharing bedding/towels/clothing | Indirect transmission route | |
| Sexual contact | Transmission route | |
| Nocturnal pruritus | Intense itching at night - most classic symptom | VERY high-yield SAQ |
| Burrows on skin | Track-like lines on skin surface | Clinical sign |
| Papules, vesicles, nodules | Lesion types | Clinical |
| Finger webs | Commonest site - first place to look | Sites |
| Wrists, elbows, axillae | Common sites | |
| Waistline, genital area | Common sites | |
| Secondary bacterial infection | Complication from scratching | Complication |
| Crusted (Norwegian) scabies | Severe form in immunocompromised - millions of mites, highly contagious | High-yield complication |
| Skin scraping microscopy | Gold standard diagnosis - identifies mites, eggs, fecal pellets | Investigation |
| Dermoscopy | Visualizes mite at end of burrow | Investigation |
| Permethrin 5% cream | First-line treatment - applied to whole body | Treatment |
| Oral Ivermectin | Alternative treatment | |
| Benzyl benzoate | Alternative treatment | |
| Sulfur ointment | Alternative treatment | |
| Treat all household contacts | Non-pharmacological - simultaneously | Key management principle |
| Wash bedding in hot water | Kills mites on fomites | Prevention |
Master Table - Pediculosis (Lice)
| Keyword | Detail | Exam Focus |
|---|---|---|
| Pediculosis | Lice infestation of hair or skin | Definition |
| Pediculus humanus capitis | Head lice | Species |
| Pediculus humanus corporis | Body lice | Species |
| Pthirus pubis | Pubic lice ("crab lice") | Species - note different genus |
| Parasitic insects | Lice are insects (6 legs), not mites | Distinguish from scabies |
| Nits | Lice eggs attached to hair shafts | Classic clinical finding |
| Common in school-aged children | Epidemiology | |
| NOT associated with poor hygiene | Important distinction - affects clean hair too | Common misconception - exam question |
| Direct head-to-head contact | Primary transmission of head lice | Transmission |
| Sharing combs, hats, towels | Indirect transmission | |
| Sexual contact | Transmission of pubic lice | Specific to Pthirus pubis |
| Intense scalp itching | Main symptom | Clinical |
| Tickling sensation | Sensation of lice moving | Clinical |
| Excoriations from scratching | Skin damage from scratching | Complication |
| Secondary bacterial infection | Complication | |
| Sleep disturbance in children | Complication | |
| Permethrin 1% lotion | First-line treatment for lice | Treatment - note: 1% for lice vs 5% for scabies |
| Malathion | Organophosphate alternative | Alternative |
| Ivermectin lotion | Alternative | |
| Spinosad | Alternative | |
| Wet combing | Non-pharmacological - fine-tooth comb through wet hair |
🧠 Memory Trick #12 - Scabies vs Lice at a glance:
| Feature | Scabies | Lice (Pediculosis) |
|---|---|---|
| Organism | Mite (Sarcoptes scabiei) | Insect (Pediculus spp.) |
| Where | Burrows in skin | Lives on hair/skin surface |
| Key sign | Nocturnal itching + burrows | Nits on hair shafts |
| Classic site | Finger webs | Scalp (head lice) |
| Permethrin dose | 5% cream | 1% lotion |
| Hygiene link | Not linked to hygiene | NOT linked to hygiene |
🧠 Memory Trick #13 - Permethrin Doses:
Scabies = 5% (S has 5 letters!) Lice = 1% (L is 1 letter!)
🧠 Memory Trick #14 - Lice Species by Location: "HBC"
Head = capitis Body = corporis Crotch (pubic) = Pthirus pubis (the "crab")
📊 MEGA COMPARISON TABLE - All Infectious Skin Diseases
| Disease | Organism | Type | Classic Sign | 1st-Line Treatment |
|---|---|---|---|---|
| Impetigo | Staph aureus | Bacterial | Golden crust | Fusidic acid (topical) / Flucloxacillin (oral) |
| Cellulitis | Strep pyogenes (2/3) | Bacterial | Redness + warmth + fever | Penicillin (oral/IV) |
| HSV (cold sore) | Herpes simplex virus | Viral | Vesicles + crusting + burning prodrome | Aciclovir |
| Shingles | Varicella-zoster (VZV) | Viral | Dermatomal rash, pain before rash | Antivirals early |
| HPV warts | Human papillomavirus | Viral | Verrucous papules | Self-limiting |
| Tinea corporis | Dermatophytes | Fungal | Annular rash, central clearing | Topical imidazole |
| Tinea capitis | Trichophyton tonsurans | Fungal | Scaly itchy scalp, hair loss (children) | Terbinafine 12 weeks |
| Onychomycosis | Dermatophytes | Fungal | Nail dystrophy, elderly | Terbinafine 12 weeks |
| Pityriasis versicolor | Malassezia spp. | Fungal | Hypopigmented macules | Itraconazole 200mg x 1 week |
| Candidiasis | Candida spp. | Fungal | Satellite lesions, moist areas | Imidazole creams |
| Scabies | Sarcoptes scabiei | Parasitic mite | Nocturnal itch + burrows + finger webs | Permethrin 5% cream |
| Pediculosis | Pediculus spp. | Parasitic insect | Nits on hair shafts + scalp itch | Permethrin 1% lotion |
🎯 PORTAL OF ENTRY CONCEPT TABLE
| Route | Mechanism | Example |
|---|---|---|
| Breaks in skin barrier | Cuts, wounds, ulcers, surgical wounds, trauma | Cellulitis entry |
| Hair follicles | Folliculitis, furunculosis | Staph aureus |
| Pre-existing skin disease | Eczema, tinea pedis cracks | Cellulitis complicating tinea pedis |
| Insect/mite burrowing | Direct penetration | Scabies |
| Mucous membranes | Oral/genital routes | HSV |
| Direct contact | Touching infected person | Impetigo, lice |
⚡ ULTIMATE EXAM QUICK TIPS
SAQ-type answers need these 4 elements per disease:
- Causative agent (organism name)
- Pathogenesis (how it causes disease)
- Clinical manifestations (signs + symptoms)
- Treatment (first-line + alternatives)
LAQ-type answers additionally need:
- Risk factors/predisposing factors
- Diagnosis/investigations
- Complications
- Prevention
🧠 MASTER MEMORY TRICK - The Big Picture
Use "BACTERIA VIRUS FUNGUS PARASITE" = "BVFP"
Bacteria = Golden crust (Impetigo) + Red warm legs (Cellulitis) Virus = Blisters (HSV) + Dermatome (Shingles) + Warts (HPV) Fungus = Rings (Tinea) + Pale patches (Pityriasis) + Satellites (Candida) Parasite = Night itch + burrows (Scabies) + Nits (Lice)
🔑 HIGH-YIELD SINGLE KEYWORDS TO MEMORIZE
| Keyword | = | Disease |
|---|---|---|
| "Golden crust" | = | Impetigo |
| "Pain before rash" | = | Shingles |
| "Dermatomal" | = | Shingles |
| "Post-herpetic neuralgia" | = | Shingles complication |
| "Eczema herpeticum" | = | HSV on eczema (emergency!) |
| "Central clearing" | = | Tinea corporis |
| "Satellite lesions" | = | Candida |
| "Hypopigmented macules" | = | Pityriasis versicolor |
| "Malassezia spp." | = | Pityriasis versicolor |
| "Nocturnal pruritus" | = | Scabies |
| "Norwegian/crusted scabies" | = | Immunocompromised + scabies |
| "Nits on hair shafts" | = | Lice |
| "NOT poor hygiene" | = | Lice (common misconception) |
| "Stratum corneum burrow" | = | Sarcoptes scabiei |
| "Trichophyton tonsurans" | = | Tinea capitis |
| "Finger webs" | = | Scabies (first site to check) |
| "Treat all contacts" | = | Scabies management |
| "Treat underlying cause" | = | Cellulitis / Intertrigo |
🗺️ RISK FACTORS SUMMARY TABLE
| Disease | Key Risk Factors |
|---|---|
| Cellulitis | Diabetes, venous disease, obesity, tinea pedis, eczema, prior cellulitis, alcoholism, pregnancy, trauma |
| Fungal infections | Moist skin, poor hygiene, shared showers, humid weather, sweaty clothes |
| Shingles | Elderly, immunocompromised |
| Norwegian scabies | Immunocompromised |
| Scabies (general) | Crowded living (nursing homes, prisons, childcare, refugee camps) |
| Candida | Moist areas, nappy area (infants), diabetes, antibiotics |
| Tinea capitis | Children, animal contact, family spread |
Study Strategy: Read the bold keywords first. Cover and recall. Use the memory tricks to link them. Then attempt writing a full SAQ answer using the 4-element formula (Organism → Pathogenesis → Clinical Features → Treatment). For LAQs, add risk factors, investigations, complications, and prevention.
Make a visual poster comparing all 12 diseases side-by-side
A large, detailed, colorful medical study poster titled "PHAR1612 - Infectious Skin Diseases: All 12 Diseases Compared" with a dark navy blue background. The poster is divided into 4 color-coded horizontal sections: SECTION 1 - BACTERIAL (red/orange band header): Three disease cards side by side: Card 1 - IMPETIGO: organism "Staph aureus", classic sign "Golden crust (honey-colored)", treatment "Fusidic acid / Flucloxacillin", icon of crusted skin lesion Card 2 - CELLULITIS: organism "Strep pyogenes (2/3)", classic sign "Red, warm, swollen leg + fever", treatment "Penicillin oral/IV", icon of red swollen leg Card 3 - ERYSIPELAS: organism "Strep pyogenes", classic sign "Sharp border, upper dermis", treatment "Penicillin", icon of demarcated red patch SECTION 2 - VIRAL (purple/violet band header): Three disease cards side by side: Card 4 - HSV (Cold Sore): organism "Herpes Simplex Virus Type 1", classic sign "Vesicles + burning prodrome", treatment "Aciclovir", complication "Eczema herpeticum" Card 5 - SHINGLES (HZV): organism "Varicella-Zoster Virus", classic sign "Dermatomal rash, pain BEFORE rash", treatment "Antivirals early", complication "Post-herpetic neuralgia" Card 6 - HPV WARTS: organism "Human Papillomavirus", classic sign "Verrucous papules", treatment "Self-limiting", note "Clears in 93% by age 16" SECTION 3 - FUNGAL (green band header): Four disease cards: Card 7 - TINEA CORPORIS: organism "Dermatophytes", classic sign "Annular ring, central clearing", treatment "Topical imidazole" Card 8 - TINEA CAPITIS: organism "Trichophyton tonsurans", classic sign "Scaly scalp, hair loss (children)", treatment "Terbinafine 12 weeks" Card 9 - ONYCHOMYCOSIS: organism "Dermatophytes", classic sign "Nail dystrophy (elderly)", treatment "Terbinafine 12 weeks" Card 10 - PITYRIASIS VERSICOLOR: organism "Malassezia spp.", classic sign "Hypopigmented macules (young adults)", treatment "Itraconazole 200mg x 1 week" Card 11 - CANDIDIASIS: organism "Candida spp.", classic sign "Satellite lesions, moist areas", treatment "Imidazole creams" SECTION 4 - PARASITIC (yellow/amber band header): Two disease cards: Card 12 - SCABIES: organism "Sarcoptes scabiei var. hominis", classic sign "NOCTURNAL itch + burrows + finger webs", treatment "Permethrin 5% cream", complication "Norwegian scabies (immunocompromised)" Card 13 - PEDICULOSIS (LICE): organism "Pediculus humanus capitis/corporis, Pthirus pubis", classic sign "Nits on hair shafts, scalp itch", treatment "Permethrin 1% lotion", note "NOT linked to poor hygiene" At the bottom, a small legend/key box showing the 4 categories with their color codes, and a memory tip row: "BVFP: Bacteria=Golden crust | Virus=Blisters/Dermatome | Fungus=Rings/Pale patches | Parasite=Night itch/Nits" All cards have white text on colored semi-transparent backgrounds, clean modern design, medical icons, and are clearly readable. Professional pharmacy lecture poster style.
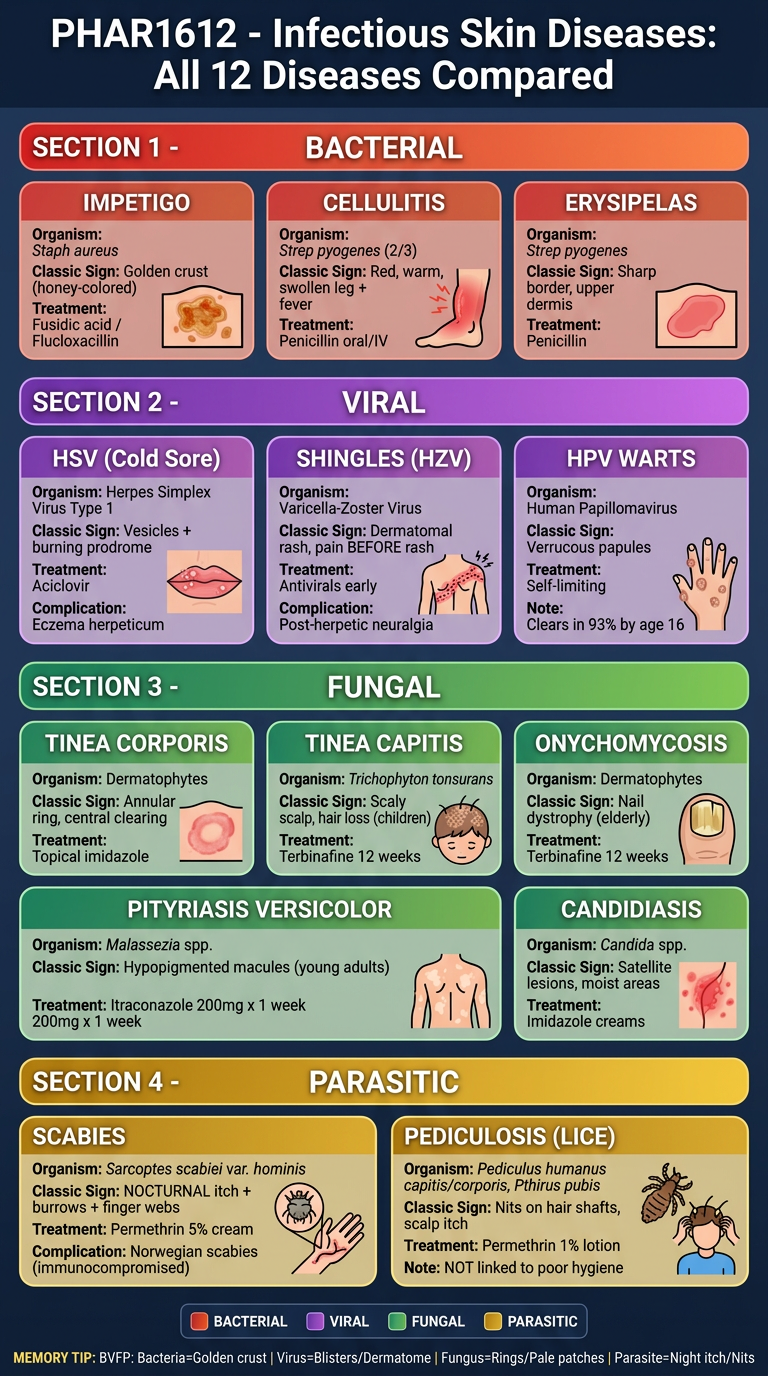
- 🔴 Red/Orange - Bacterial (Impetigo, Cellulitis, Erysipelas)
- 🟣 Purple - Viral (HSV, Shingles, HPV Warts)
- 🟢 Green - Fungal (Tinea corporis, Tinea capitis, Onychomycosis, Pityriasis versicolor, Candidiasis)
- 🟡 Yellow/Amber - Parasitic (Scabies, Lice)
Make a summary infographic showing diagnosis workflow for each disease type
A large, detailed, professional medical infographic poster titled "INFECTIOUS SKIN DISEASES — DIAGNOSIS WORKFLOW" on a deep dark navy background with white and bright colored text. The poster is organized into 4 vertical flowchart columns, one per disease category, each with a distinct color theme. COLUMN 1 - BACTERIAL (color theme: red/coral): Header box: "🦠 BACTERIAL" in red Step 1 box: "HISTORY" — fever? systemic symptoms? prior episodes? diabetes? tinea pedis? trauma? Arrow down Step 2 box: "CLINICAL EXAM" — Golden honey crust → IMPETIGO | Red warm swollen limb + fever → CELLULITIS/ERYSIPELAS | Sharp vs. diffuse border distinguishes Erysipelas vs Cellulitis Arrow down Step 3 box: "INVESTIGATIONS" — Usually clinical diagnosis | Wound swab if needed | Blood cultures if systemic Arrow down Step 4 box: "DIAGNOSIS CONFIRMED" — Impetigo / Cellulitis / Erysipelas Arrow down Step 5 box (green): "TREAT" — Fusidic acid (Impetigo) | Penicillin oral/IV (Cellulitis) | Treat underlying predisposing factor! COLUMN 2 - VIRAL (color theme: purple/violet): Header box: "🔬 VIRAL" in purple Step 1 box: "HISTORY" — burning prodrome? prior chickenpox? immunocompromised? age? warts? Arrow down Step 2 box: "CLINICAL EXAM" — Lip vesicles + burning prodrome → HSV-1 | Dermatomal rash + pain before rash → SHINGLES | Verrucous papules → HPV WARTS | Widespread vesicles on eczema → ECZEMA HERPETICUM (emergency!) Arrow down Step 3 box: "INVESTIGATIONS" — Usually clinical | Tzanck smear for HSV | PCR for confirmation Arrow down Step 4 box: "DIAGNOSIS CONFIRMED" — HSV / HZV / HPV Arrow down Step 5 box (green): "TREAT" — Aciclovir (HSV/HZV) | Early antivirals reduce post-herpetic neuralgia | HPV = self-limiting (watchful waiting) COLUMN 3 - FUNGAL (color theme: green/teal): Header box: "🍄 FUNGAL" in green Step 1 box: "HISTORY" — moist environment? shared showers? immunocompromised? nail changes? young adult? infant nappy rash? Arrow down Step 2 box: "CLINICAL EXAM" — Annular ring + central clearing → TINEA CORPORIS | Scaly scalp + hair loss (child) → TINEA CAPITIS | Nail dystrophy (elderly) → ONYCHOMYCOSIS | Hypopigmented macules (young adult) → PITYRIASIS VERSICOLOR | Satellite lesions + moist folds → CANDIDIASIS Arrow down Step 3 box: "INVESTIGATIONS" — Skin scraping for mycology | Hair samples for Tinea capitis | Nail clippings for onychomycosis | KOH preparation microscopy Arrow down Step 4 box: "DIAGNOSIS CONFIRMED" — Type of Tinea / Candida / Pityriasis Arrow down Step 5 box (green): "TREAT" — Topical imidazole (Tinea corporis/Candida) | Terbinafine 12 wks (Tinea capitis/Onychomycosis) | Itraconazole 200mg x 1 week (Pityriasis) | Ketoconazole shampoo COLUMN 4 - PARASITIC (color theme: amber/yellow): Header box: "🕷️ PARASITIC" in amber Step 1 box: "HISTORY" — crowded living? nursing home? school-age child? sexual contact? nocturnal itch? household contacts affected? Arrow down Step 2 box: "CLINICAL EXAM" — Nocturnal itch + burrows + finger webs → SCABIES | Crusty hyperkeratotic skin (immunocomp.) → NORWEGIAN SCABIES | Nits on hair shafts + scalp itch → HEAD LICE | Pubic area + sexual contact → PUBIC LICE Arrow down Step 3 box: "INVESTIGATIONS" — SCABIES: Skin scraping microscopy (mites + eggs + fecal pellets), Dermoscopy, Adhesive tape test | LICE: Visual inspection for nits and live lice Arrow down Step 4 box: "DIAGNOSIS CONFIRMED" — Scabies / Head Lice / Body Lice / Pubic Lice Arrow down Step 5 box (green): "TREAT" — Permethrin 5% cream (Scabies) | Permethrin 1% lotion (Lice) | Treat ALL household contacts simultaneously | Wash bedding in HOT water At the very top of the poster, a subtitle reads: "HISTORY → CLINICAL EXAM → INVESTIGATIONS → CONFIRMED DIAGNOSIS → TREATMENT" At the bottom, a red alert box: "⚠️ RED FLAGS: Eczema Herpeticum (refer urgently) | Norwegian Scabies (immunocompromised) | Cellulitis with systemic fever (IV antibiotics)" Clean flowchart arrows connecting each step. Each column has a subtle colored background panel. Bold white text, modern medical infographic style, highly readable and organized for exam revision.
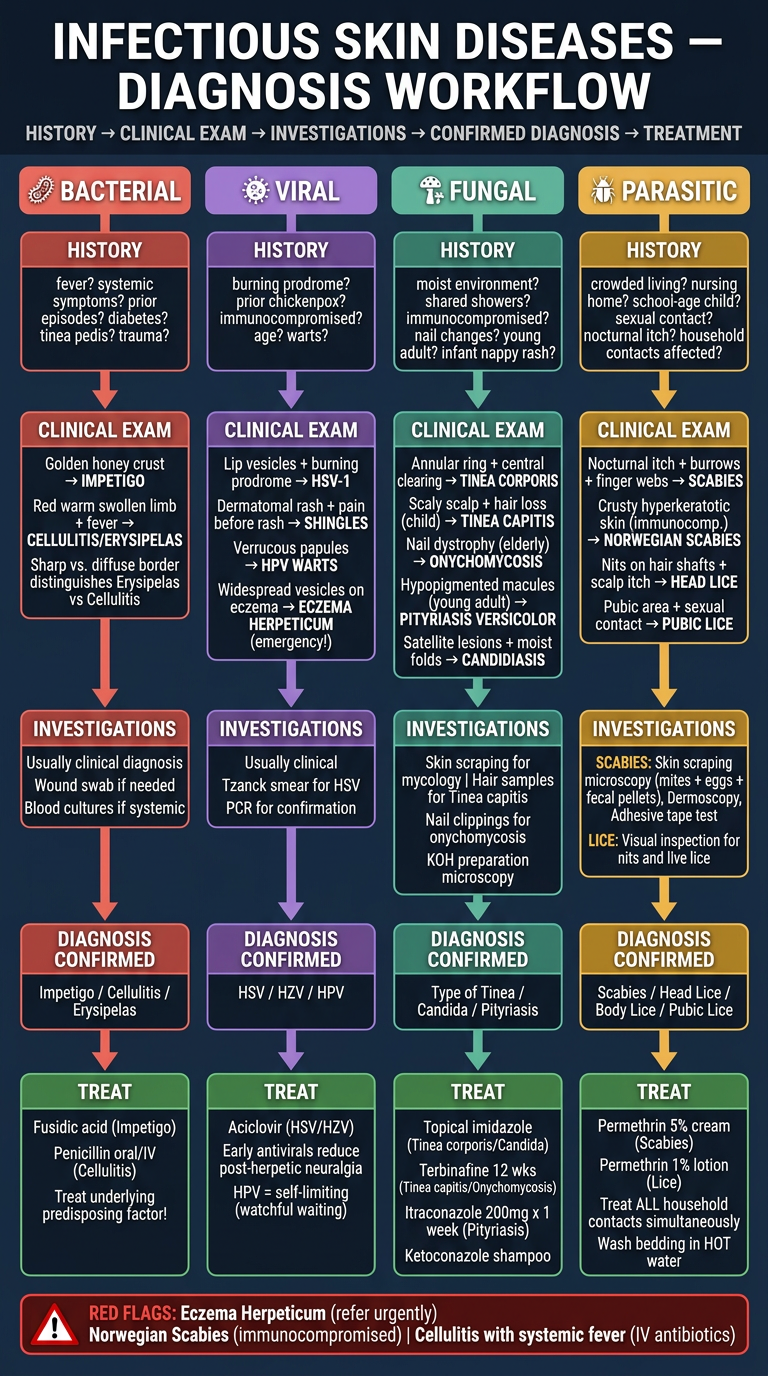
- History - Key questions to ask (risk factors, symptoms)
- Clinical Exam - Pattern recognition (which finding = which disease)
- Investigations - What to order and why
- Confirmed Diagnosis - Naming the disease
- Treatment - First-line drugs
- Eczema herpeticum - HSV on eczema, refer urgently
- Norwegian scabies - in immunocompromised, millions of mites
- Cellulitis with fever - needs IV antibiotics, not just oral