Projectile vomiting pathphysiology and reason
Reading File
Finding Sources
Finding Sources
Searching the Web
projectile vomiting pathophysiology mechanism causes
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive textbook content. Here is a detailed, well-structured answer:
Projectile Vomiting: Pathophysiology & Causes
What Is Projectile Vomiting?
Projectile vomiting is a forceful expulsion of gastric contents, typically sudden and without warning, propelled with far greater force than ordinary vomiting. Unlike normal emesis, it is often not preceded by nausea (especially in neurological causes) and the vomit is expelled over a significant distance. — Sleisenger and Fordtran's Gastrointestinal and Liver Disease
The Normal Vomiting Reflex (Foundation)
To understand projectile vomiting, the underlying emetic reflex must be understood:
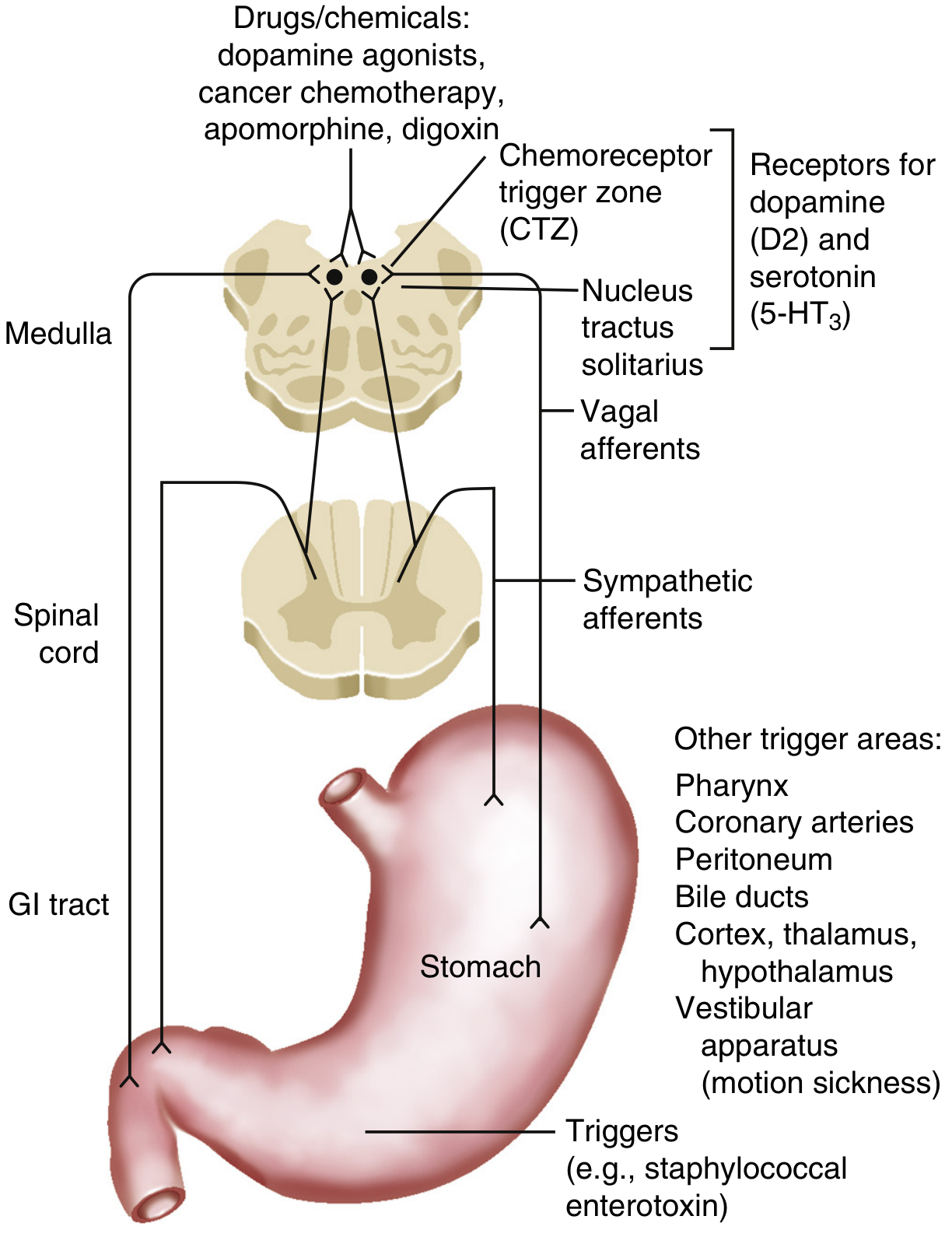
Neural pathways mediating vomiting. — Sleisenger and Fordtran's GI & Liver Disease, Fig. 15.1
The emetic reflex has three sequential phases:
- Nausea — cortical activation; stomach relaxes, antral/intestinal peristalsis is inhibited.
- Retching — spasmodic contractions of the diaphragm and intercostal muscles with glottis closure.
- Vomiting (emesis) — simultaneous activation of somatic and visceral components:
- Brisk contraction of the diaphragm and abdominal muscles
- Relaxation of the lower esophageal sphincter
- Forceful retrograde peristaltic contraction in the jejunum, pushing enteric content orally
- Soft palate elevates to protect the nasopharynx
- Glottis closes to prevent aspiration
— Sleisenger and Fordtran's GI & Liver Disease, p. 212
Central Control: Brainstem "Vomiting Center"
The coordinating center is a network of neurons in the ventrolateral medullary tegmentum (near the nucleus ambiguus). It integrates signals from:
| Input Source | Pathway |
|---|---|
| GI tract (pharynx, stomach, small intestine) | Vagal afferents → nucleus tractus solitarius |
| Bloodborne toxins/drugs | Chemoreceptor Trigger Zone (CTZ) in area postrema |
| Vestibular system | Via cerebellum |
| Cortex, hypothalamus, thalamus | Higher CNS pathways |
| Extraintestinal organs (heart, testis, peritoneum) | Sympathetic/vagal afferents |
The CTZ/area postrema sits on the floor of the 4th ventricle and lies outside the blood-brain barrier — it can detect circulating emetic molecules directly. It contains dopamine (D2) and serotonin (5-HT3) receptors. — Plum and Posner's Diagnosis and Treatment of Stupor and Coma
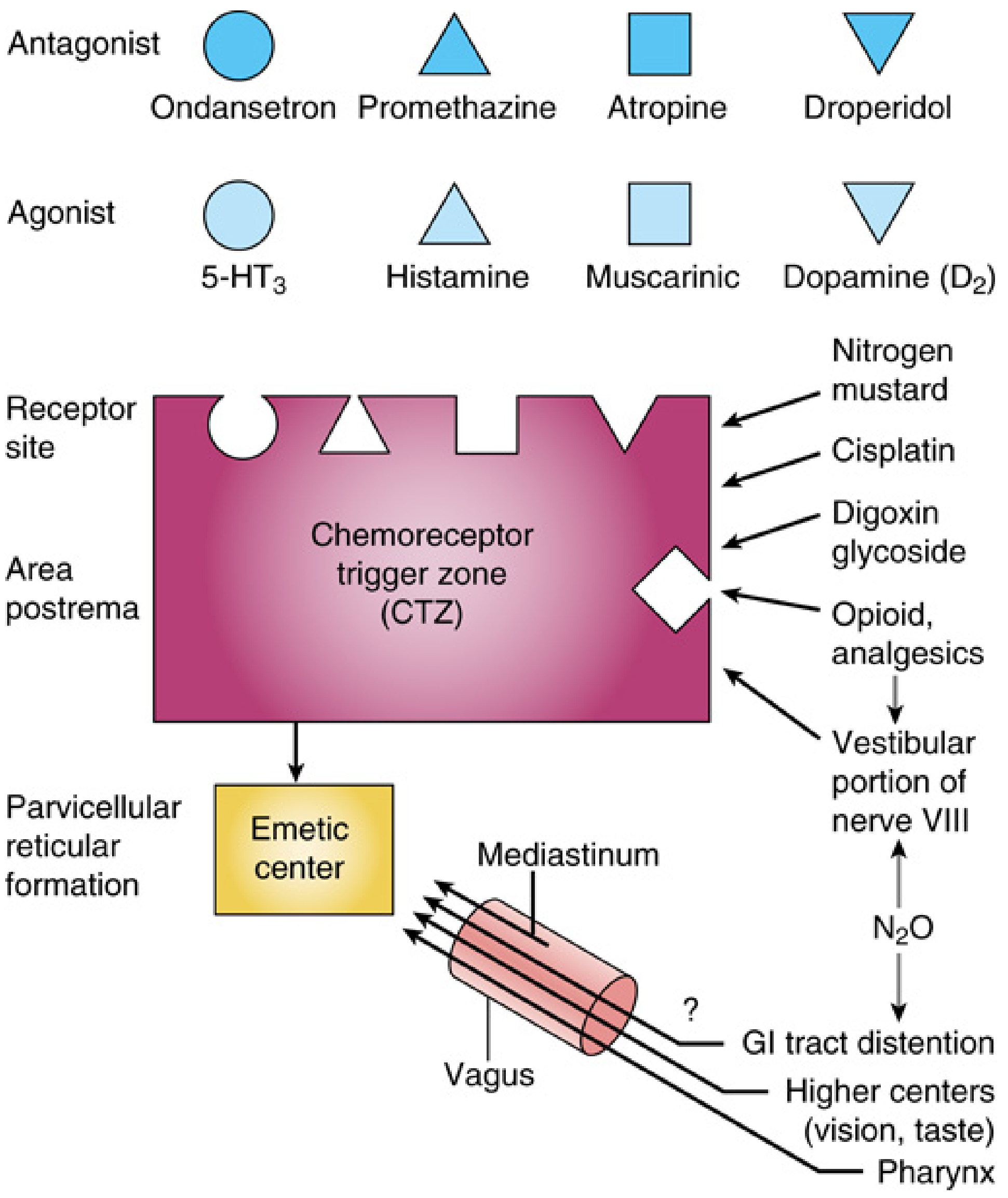
CTZ receptor sites and emetic stimuli. — Miller's Anesthesia, Fig. 22.20
What Makes Vomiting "Projectile"?
Projectile vomiting results from an exaggerated or abrupt activation of the emetic motor program — specifically, a more explosive contraction of the diaphragm and abdominal wall muscles combined with forceful retrograde gut contractions. There are two main mechanisms:
1. Mechanical Obstruction (GI Origin)
When there is gastric outflow obstruction, the stomach builds up pressure over time. Eventually, the stomach overdistends and the emetic reflex fires in an exaggerated fashion — the contractile force needed to overcome the obstruction propels vomit with great force. The vomit is typically nonbilious (because obstruction is proximal to the ampulla of Vater).
2. Raised Intracranial Pressure (Central/Neurological Origin)
A sudden rise in ICP directly compresses the floor of the fourth ventricle, stimulating the emetic center abruptly and without preceding nausea. This produces the hallmark "sudden, projectile vomiting without warning." — Plum and Posner's Stupor and Coma, p. 123
"The pressure wave may stimulate the emetic response directly by pressure on the floor of the fourth ventricle, resulting in sudden, 'projectile' vomiting, without warning."
Causes of Projectile Vomiting
In Infants & Children
| Condition | Mechanism | Key Features |
|---|---|---|
| Hypertrophic Pyloric Stenosis | Hypertrophy of pyloric smooth muscle → gastric outflow obstruction → progressive distension → forceful emesis | Most classic cause; 2–6 weeks of age; nonbilious; olive-shaped mass; ♂ > ♀; metabolic alkalosis (hypochloremic, hypokalemic, hyponatremic) |
| Malrotation with Volvulus | Midgut twisting → obstruction | Bilious vomiting; surgical emergency |
| Intussusception | Bowel telescoping → obstruction | Colicky pain; currant-jelly stool |
| Increased ICP (posterior fossa tumors, hydrocephalus) | Direct compression of 4th ventricle floor | Morning vomiting, papilledema, headache |
| Gastroenteritis / Overeating | GI tract distension → vagal activation | Often with diarrhea |
— Tintinalli's Emergency Medicine; Robbins & Cotran Pathologic Basis of Disease
Pyloric stenosis is the prototypical cause: muscle hypertrophy narrows the pyloric channel progressively, presenting between 3–6 weeks of life with post-feed projectile vomiting, followed by the infant remaining hungry ("hungry vomiter"). — Quick Compendium of Clinical Pathology
In Adults
| Condition | Mechanism |
|---|---|
| Raised ICP (tumors, SAH, hydrocephalus, cerebral edema) | Compression of 4th ventricle → abrupt CTZ/emetic center activation |
| Posterior fossa tumors / medulloblastoma | Direct brainstem/cerebellum pressure; morning vomiting on awakening (CO2 rise during sleep → cerebral vasodilation → ICP spike) |
| Subarachnoid hemorrhage | Sudden ICP surge |
| Acute meningitis / encephalitis | Meningeal irritation + raised ICP |
| GI obstruction (e.g., pyloric stricture from PUD, gastric cancer) | Mechanical gastric outlet obstruction |
| Cyclic vomiting syndrome | Hypothalamic dysfunction; episodic severe emesis |
| Acute vestibular disorders | Vestibular → cerebellar → brainstem activation |
Key Receptor Pathways (Pharmacological Relevance)
| Receptor | Location | Role | Drug Target |
|---|---|---|---|
| 5-HT3 | Vagal afferents, CTZ | Chemotherapy-induced, peripheral emesis | Ondansetron |
| D2 (dopamine) | CTZ/area postrema | Drug/toxin-induced emesis | Metoclopramide, droperidol |
| NK-1 (substance P) | Area postrema, NTS | Delayed emesis (24–72 h post-chemo) | Aprepitant |
| H1 (histamine) | Vestibular nucleus, NTS | Motion sickness, pregnancy | Promethazine |
| Muscarinic M1 | Vestibular center | Motion sickness | Scopolamine |
— Sleisenger and Fordtran's GI & Liver Disease, p. 212
Summary
Projectile vomiting occurs via two broad pathophysiological routes:
- Peripheral: Gastric outlet obstruction builds intragastric pressure → explosive activation of the emetic motor program (classic example: pyloric stenosis in infants — nonbilious, post-prandial, progressive)
- Central: Sudden raised ICP directly compresses the floor of the 4th ventricle → abrupt emetic center firing without nausea warning (classic examples: posterior fossa tumors, subarachnoid hemorrhage, acute hydrocephalus)
The force comes from the synchronized, over-recruited contraction of the diaphragm, abdominal wall, and retrograde jejunal peristalsis — the same machinery as normal vomiting, but activated more abruptly and intensely.
Chps detail
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.