Management of acute esophageal variceal hemorrhage
Reading File
Finding Sources
Finding Sources
Searching PubMed
"esophageal varices"[MeSH Terms] AND "hemorrhage"[MeSH Terms] AND management
Reading File
Reading File
Searching PubMed
"variceal bleeding" AND "acute management"
Reading File
Searching PubMed
"esophageal varices" AND "acute bleeding"
Loading Image
Loading Image
Loading Image
I have comprehensive textbook content and key images. Now let me compile the full, detailed answer.
Management of Acute Esophageal Variceal Hemorrhage
Acute esophageal variceal hemorrhage (EVH) is a life-threatening emergency in patients with portal hypertension, carrying a 6-week mortality of 15-20% even with modern treatment. Management follows a stepwise, simultaneous approach: resuscitation, pharmacotherapy, endoscopy, and escalation if needed.
1. Initial Resuscitation & Airway
Airway protection is the first priority. Patients with active hematemesis, encephalopathy, or hemodynamic instability should be electively intubated before endoscopy to prevent aspiration. A large-bore IV access (at least two peripheral lines or central line) and ICU-level monitoring are required.
Fluid and blood resuscitation should be restrictive:
- Transfuse packed red blood cells to maintain hemoglobin at 7-8 g/dL (not higher - overtransfusion raises portal pressure and worsens rebleeding)
- Fresh frozen plasma and platelets guided by coagulation studies
- Avoid aggressive crystalloid resuscitation (worsens portal hypertension)
2. Vasoactive Drug Therapy (Start Immediately - Before Endoscopy)
Vasoactive agents must be initiated promptly upon suspicion of variceal hemorrhage and continued for 5 days. They work by causing splanchnic vasoconstriction, reducing portal venous inflow and pressure.
| Drug | Dosing | Availability |
|---|---|---|
| Octreotide (somatostatin analog) | 50 μg IV bolus → 50 μg/h infusion; bolus may be repeated in 1st hour if bleeding uncontrolled | USA (preferred in US) |
| Somatostatin | 250 μg IV bolus → 250-500 μg/h infusion | Outside USA |
| Vapreotide | 50 μg IV bolus → 50 μg/h infusion | Outside USA |
| Terlipressin (vasopressin analog) | 2 mg IV q4h × 48h → then 1 mg IV q4h | Outside USA |
Vapreotide administered before endoscopy significantly reduces the rate of active bleeding seen at endoscopy, reduces transfusion requirements, and improves day-5 survival vs. placebo. In general, vasoactive drugs reduce all-cause mortality and decrease transfusion requirements.
- Yamada's Textbook of Gastroenterology, 7e, Table 124.5
3. Antibiotic Prophylaxis
Mandatory in all patients with cirrhosis presenting with EVH. Bacterial infections occur in 35-66% of cirrhotics with GI bleeding and worsen outcomes.
- Ceftriaxone 1 g IV daily (preferred, especially in patients with advanced cirrhosis or in hospitals with high prevalence of fluoroquinolone-resistant organisms)
- Norfloxacin 400 mg PO twice daily (alternative where oral route available)
- Duration: 5-7 days
- Reduces mortality, bacterial infections, and early rebleeding
4. Endoscopic Therapy (Within 6-12 Hours)
Upper endoscopy should be performed within 6-12 hours of admission (there is evidence suggesting no survival disadvantage if delayed up to 24 hours in stable patients, but early endoscopy is standard).
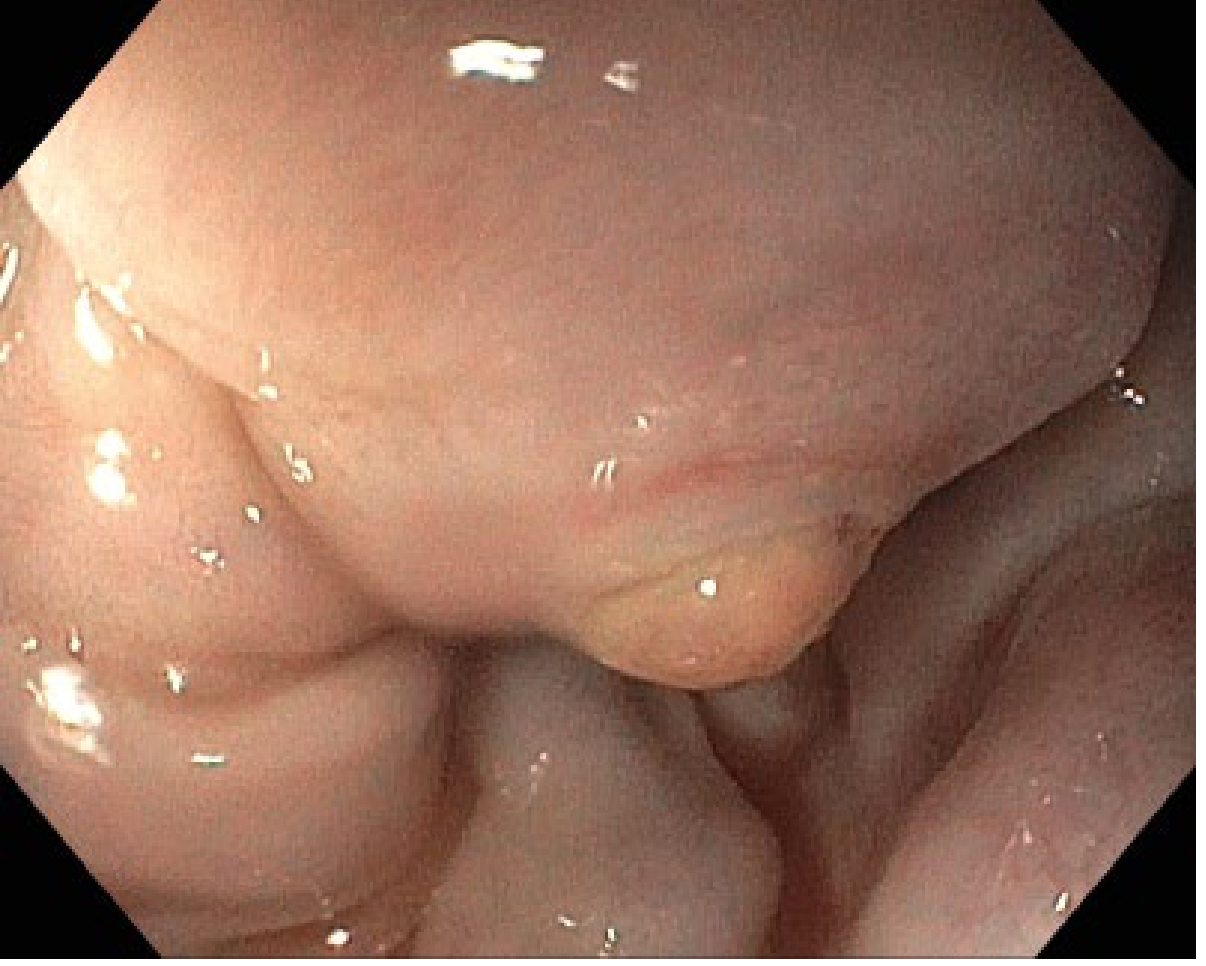
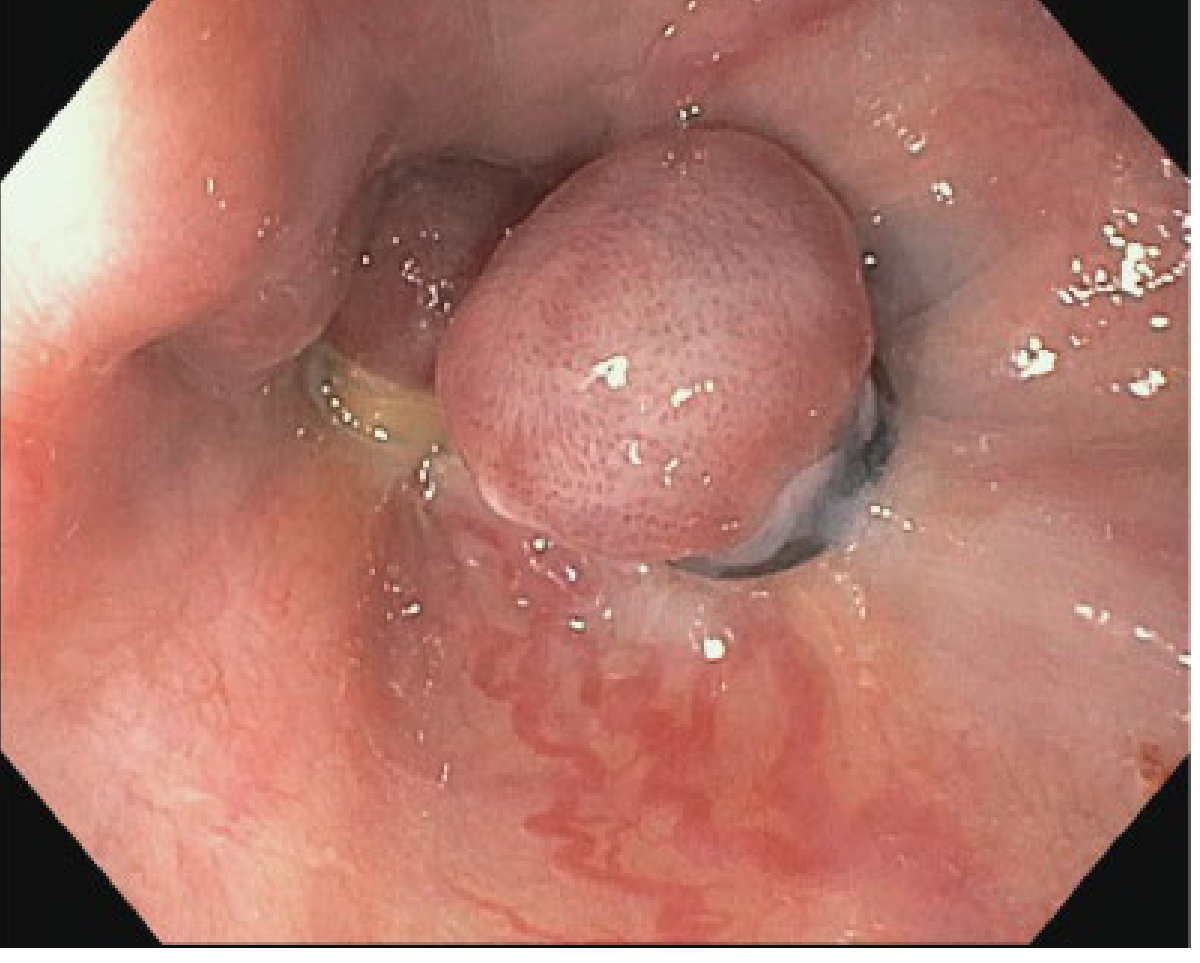
Diagnostic criteria for variceal bleeding at endoscopy:
- Active bleeding (spurting or oozing) from a varix
- White nipple sign or clot adherent to a varix
- Varices without other potential source of bleeding
Endoscopic Variceal Ligation (EVL) - Treatment of Choice
EVL is preferred over sclerotherapy and achieves initial hemostasis in 75-90% of patients. Multiple randomized trials have confirmed EVL is superior to endoscopic sclerotherapy (EST) for:
- Faster variceal eradication
- Lower rebleeding rates
- Improved survival
- Fewer complications (lower rates of stricture, ulceration)
Technique: Elastic bands are placed starting at the gastroesophageal junction, applied in a spiral fashion targeting varices in the distal 5-7 cm of the esophagus. Up to 6 bands per session is standard; more than 6 does not improve outcomes and increases complications. Procedure is done under direct vision by suctioning the varix into the ligator cap until "red out" is achieved, then deploying the band.
Post-EVL: transient chest pain/dysphagia treated with lidocaine-antacid mixture; liquid diet for 24 hours; repeat sessions every 2-4 weeks until obliteration.
Endoscopic Sclerotherapy (EST)
- Reserve for situations where EVL is not technically feasible
- Higher complication rate (esophageal ulcers, strictures, mediastinitis)
- Same initial hemostasis rate (~75-90%) but inferior long-term profile
5. Prokinetics (Pre-Endoscopy Visualization)
- IV erythromycin or metoclopramide given 20-30 minutes before endoscopy improves gastric emptying and visualization
- Reduces the need for repeat endoscopy
- Does not affect survival, but improves procedural quality
6. Balloon Tamponade (Bridge Therapy)
Used as a bridge when definitive therapy is unavailable or when massive hemorrhage prevents endoscopy. Controls bleeding in ~80% of patients but is associated with serious complications and must not remain in place for >24 hours.
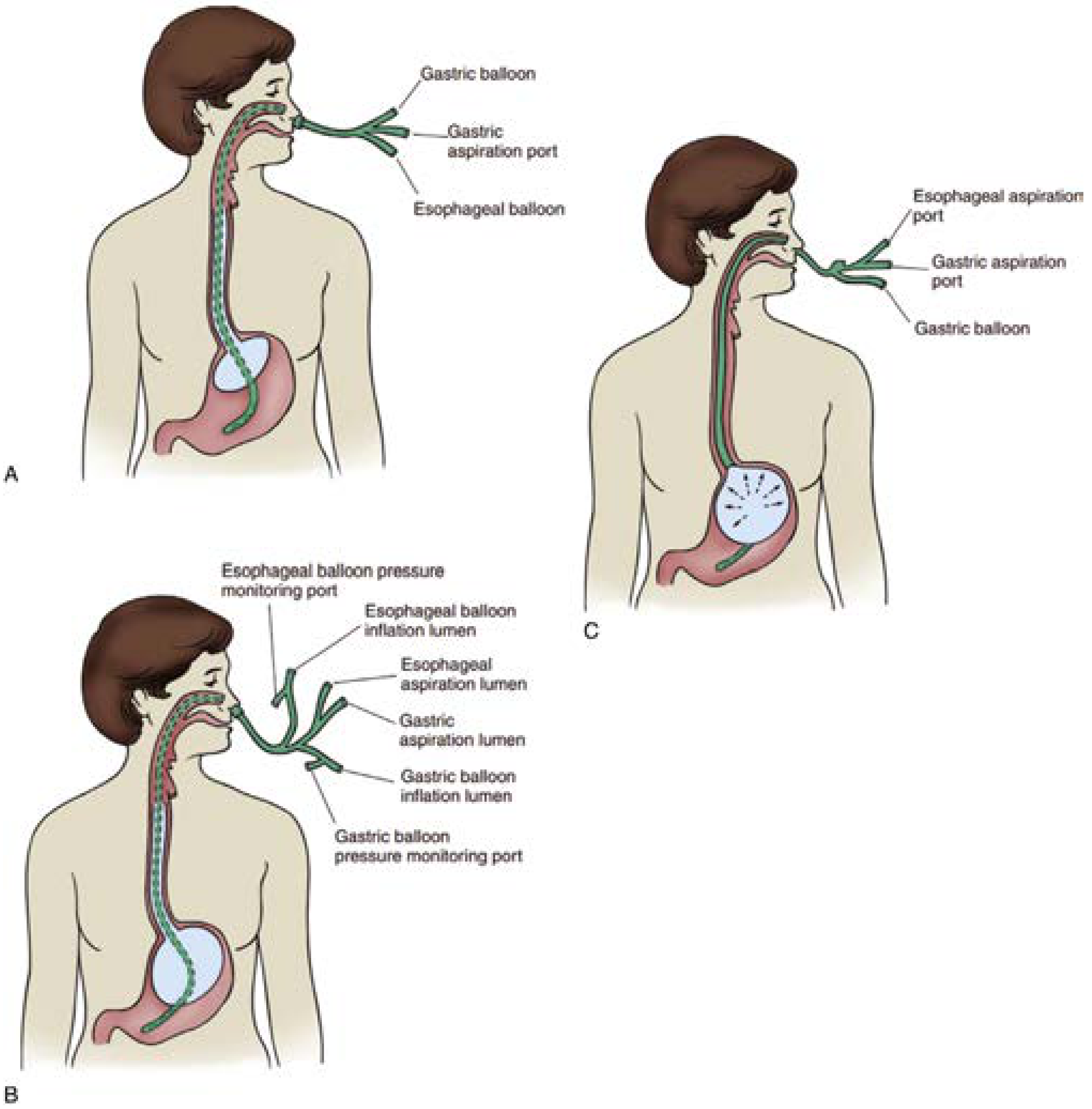
Key points for insertion:
- Always intubate before insertion (aspiration risk, poor patient tolerance)
- Insert tube at least 50 cm before inflating the gastric balloon (to avoid esophageal perforation)
- Confirm position with X-ray showing air-filled balloon in stomach
- Apply gentle traction (0.5-1.0 kg, using saline IV bags)
- Most bleeding is controlled with gastric balloon alone (since most varices are at the GEJ)
- Inflate esophageal balloon only if bleeding persists from the esophageal port
- Minnesota tube has 4 ports (includes esophageal suction) - preferred over Sengstaken-Blakemore
Complications: aspiration, tube migration, esophageal perforation/necrosis - hence use is a true temporizing measure only.
Self-expandable metal stents (SEMS): An emerging alternative to balloon tamponade - esophageal covered stents can be placed endoscopically to tamponade bleeding with less aspiration risk and longer duration of placement. Shown superior to balloon tamponade in randomized trials.
7. Salvage Therapy: TIPS (Transjugular Intrahepatic Portosystemic Shunt)
Standard/Rescue TIPS
Indicated when EVL + vasoactive therapy fails (refractory/recurrent bleeding after 2 endoscopic sessions). TIPS creates a low-resistance communication between the portal and hepatic veins, reducing portal pressure directly.
Early/Pre-emptive TIPS
A major advance: In high-risk patients (Child-Pugh C ≤13 or Child-Pugh B with active bleeding at endoscopy), early TIPS within 72 hours of presentation significantly improves survival compared to standard medical therapy + EVL. This approach - studied by Garcia-Pagan et al. - has been incorporated into guidelines.
- TIPS with covered (PTFE-coated) stents is preferred (lower shunt dysfunction/occlusion rates)
- Post-TIPS complications: hepatic encephalopathy (most common), shunt occlusion, heart failure from increased venous return
- All patients who survive EVH should be evaluated for liver transplantation (1-year mortality up to 50% after variceal bleeding)
- Current Surgical Therapy 14e, p. 473; Yamada's Gastroenterology, 7e
8. Surgical Options (Rarely Used)
Surgery is reserved for patients who fail endoscopic and TIPS therapies and are not transplant candidates, or in centers without TIPS capability.
- Portosystemic shunts: Distal splenorenal shunt (Warren shunt), mesocaval shunt - decompress the portal system
- Esophageal transection: With devascularization (Sugiura procedure) - used in refractory cases in some centers
- Liver transplantation: Definitive treatment - addresses the underlying portal hypertension and liver failure
9. Secondary Prophylaxis (Post-Acute Phase)
Every patient who survives an episode of EVH requires secondary prophylaxis to prevent rebleeding (risk ~60-70% at 1-2 years without treatment):
- EVL repeated every 2-4 weeks until variceal obliteration (then surveillance at 3 months, 6 months, then yearly)
- Non-selective beta-blockers (NSBBs): Propranolol, nadolol, or carvedilol - combine with EVL for superior efficacy
- Carvedilol provides additional alpha-1 blockade, lowering HVPG more than traditional NSBBs
- Combination EVL + NSBB is the current standard for secondary prevention
- NSBB monotherapy reduces HVPG - a response (>20% reduction or HVPG <12 mmHg) correlates with lower rebleeding risk
Summary Algorithm
Suspected EVH
↓
Airway protection (intubate if needed)
↓
Restrictive transfusion (Hb target 7-8 g/dL)
↓
Start vasoactive agent (octreotide 50 μg IV bolus → 50 μg/h × 5 days)
↓
IV antibiotics (ceftriaxone 1 g/day × 5-7 days)
↓
Upper endoscopy within 6-12 hours → EVL (preferred)
↓
Bleeding controlled?
YES → Continue vasoactive × 5 days; secondary prophylaxis (EVL + NSBB)
NO → Repeat endoscopy / balloon tamponade as bridge
→ TIPS (rescue or early TIPS in high-risk patients)
→ Surgical shunt / transplantation evaluation
Key mortality predictors: Child-Pugh/MELD score, failure to control bleeding at 5 days, bacterial infection, and renal failure. All survivors of EVH should be referred for liver transplant evaluation given the 1-year mortality risk of up to 50%.
Sources: Yamada's Textbook of Gastroenterology 7e (Ch. 124); Current Surgical Therapy 14e; Miller's Anesthesia 10e
This is a shared conversation. Sign in to Orris to start your own chat.