Small cell lung carcinoma
Reading File
Finding Sources
Searching PubMed
"small cell lung carcinoma"[MeSH Terms]
Searching the Web
small cell lung carcinoma pathology clinical features treatment 2025
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive, authoritative content from multiple textbooks. Let me compile the complete answer.
Small Cell Lung Carcinoma (SCLC)
Overview
SCLC is the most aggressive pulmonary malignancy, accounting for approximately 13% of all lung cancer cases in the United States (a decline from ~17% in the 1980s). It is strongly linked to cigarette smoking and is rare in never-smokers; the diagnosis should be reconsidered in any patient without a significant tobacco history. It is the most common of the pulmonary neuroendocrine tumors and is pathologically classified as a high-grade neuroendocrine carcinoma.
- Goldman-Cecil Medicine, p. 2019
- Fishman's Pulmonary Diseases, p. 1972
Pathology and Histology
The 2021 WHO classification defines SCLC as a malignant epithelial tumor with:
- Small cells - typically less than the diameter of 3 resting small lymphocytes (~10 µm), though size varies (up to 45 µm)
- Scant cytoplasm with poorly defined cell borders
- Finely granular nuclear chromatin ("salt and pepper" pattern)
- Absent or inconspicuous nucleoli
- Nuclear molding - cells mold to each other under pressure
- Azzopardi effect - basophilic DNA encrustation of vessel walls from crush artifact
- High mitotic rate - averaging >60 mitoses per 2 mm²
- Extensive necrosis and numerous apoptotic cells
Cells may be round, oval, or spindle-shaped. The tumor arises centrally (peribronchial) and tends to grow submucosally along bronchi.
- Fishman's Pulmonary Diseases, p. 1971-1972
H&E histology (400x) - classic appearance:
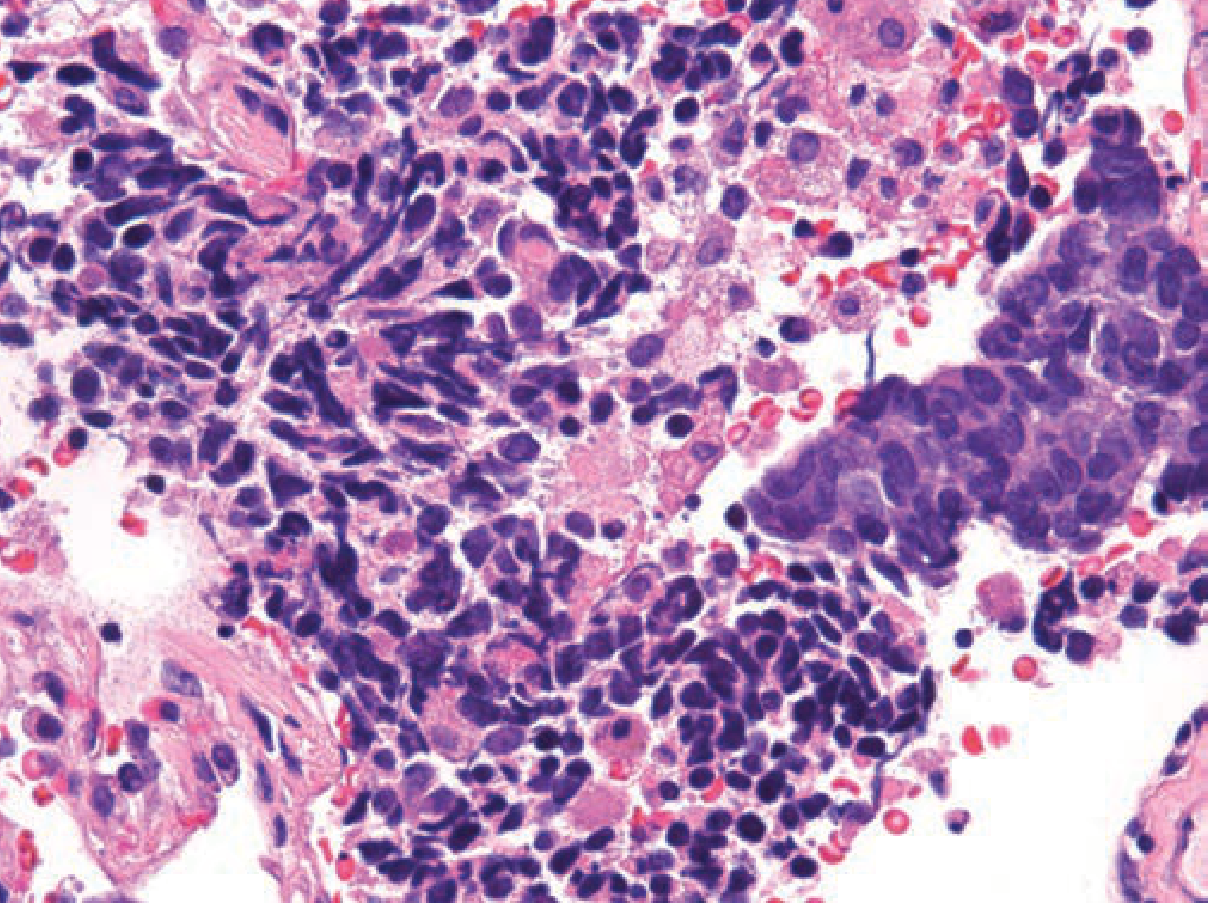
Figure: Small cell carcinoma. Classic tumor cell appearance with scant cytoplasm, hyperchromatic nuclei, nuclear molding, crush artifact, and necrosis. (H&E, 400x) - Fishman's Pulmonary Diseases
Immunohistochemistry
SCLC stains positively for neuroendocrine markers:
- Chromogranin A
- Synaptophysin
- CD56 (NCAM)
- TTF-1 (thyroid transcription factor-1) - positive in ~70-80%
Molecular Biology
Per recent evidence, SCLC is characterized by:
- Universal inactivation of TP53 and RB1 (tumor suppressor genes)
- MYC family overexpression (MYCL, MYCN, MYC)
- Dysregulation of multiple oncogenic signaling pathways
- A transcription factor-based molecular subtype system has now been proposed: SCLC-A (ASCL1), SCLC-N (NEUROD1), SCLC-P (POU2F3), and SCLC-I (YAP1/inflamed) - reflecting tumor heterogeneity and lineage plasticity
As highlighted in a 2025 review on current and future therapies, molecular subtyping adds complexity and poses challenges for therapeutic development.
Clinical Features
Presentation
- Pulmonary symptoms: cough, wheezing, dyspnea, hemoptysis (from large central mass)
- Mediastinal extension: superior vena cava (SVC) syndrome, recurrent laryngeal nerve paralysis, dysphagia
- Constitutional symptoms: pain, anorexia, weight loss
- Widespread metastases at presentation: liver, brain, bone, adrenal glands
Paraneoplastic Syndromes
SCLC is the classic tumor associated with multiple paraneoplastic syndromes:
Endocrine:
| Syndrome | Features | Key Labs |
|---|---|---|
| SIADH | Gait disturbance, headache, nausea, confusion, seizures, coma | Hyponatremia (severe <125 mmol/L), elevated urine osmolality |
| Ectopic ACTH (Cushing syndrome) | Muscle weakness, edema, hypertension, weight gain | Hypokalemia <3.0 mmol/L, cortisol >800 nmol/L, not suppressed by dexamethasone |
| Hypercalcemia | Via PTHrP secretion | Elevated serum calcium |
Neurological (from Table 116-4, Fishman's):
| Syndrome | Antibodies | Features |
|---|---|---|
| Limbic encephalitis | Anti-Hu (ANNA-1), anti-CRMP5 | Mood changes, hallucinations, memory loss, seizures |
| Lambert-Eaton myasthenic syndrome (LEMS) | Anti-VGCC | Proximal muscle weakness, hyporeflexia, autonomic dysfunction; improves with repetitive stimulation (opposite of myasthenia gravis) |
| Sensory neuropathy | Anti-Hu | Painful paresthesias, loss of proprioception |
SCLC accounts for 19-50% of carcinomas causing ectopic ACTH syndrome.
- Fishman's Pulmonary Diseases, p. 2039; Goldman-Cecil Medicine
Staging
SCLC uses a two-stage system developed by the Veterans Administration Lung Cancer Staging Group:
Limited Stage (LS)
Tumor confined to one hemithorax and regional lymph nodes (hilar, ipsilateral and contralateral mediastinal, ipsilateral and contralateral supraclavicular nodes), including ipsilateral pleural effusion (regardless of cytology). About 30-40% of patients present at this stage.
Extensive Stage (ES)
Disease beyond the above boundaries, including: contralateral chest, distant metastases, malignant pericardial effusion, bilateral pulmonary involvement. About 60-70% of patients present with ES disease.
Note: The IASLC now recommends adopting the TNM staging system (used for surgical candidates), and the TNM system is used in pathologic evaluation per CAP protocols.
- Mulholland & Greenfield's Surgery, p. 4279; Fishman's, p. 1971
Metastatic Workup
- CT chest/abdomen/pelvis (or PET-CT)
- MRI brain
- Bone scan (if PET not available)
- Serum electrolytes, glucose, calcium; renal and liver function tests
PET/CT has a sensitivity of 97.5% and specificity of 98.2% for extensive disease. It can change clinical management in 27-47% of SCLC patients at initial staging and changes the LS vs ES classification in ~15% of cases.
- Murray & Nadel's Respiratory Medicine; Fishman's Nuclear Medicine section
Treatment
Management Algorithm
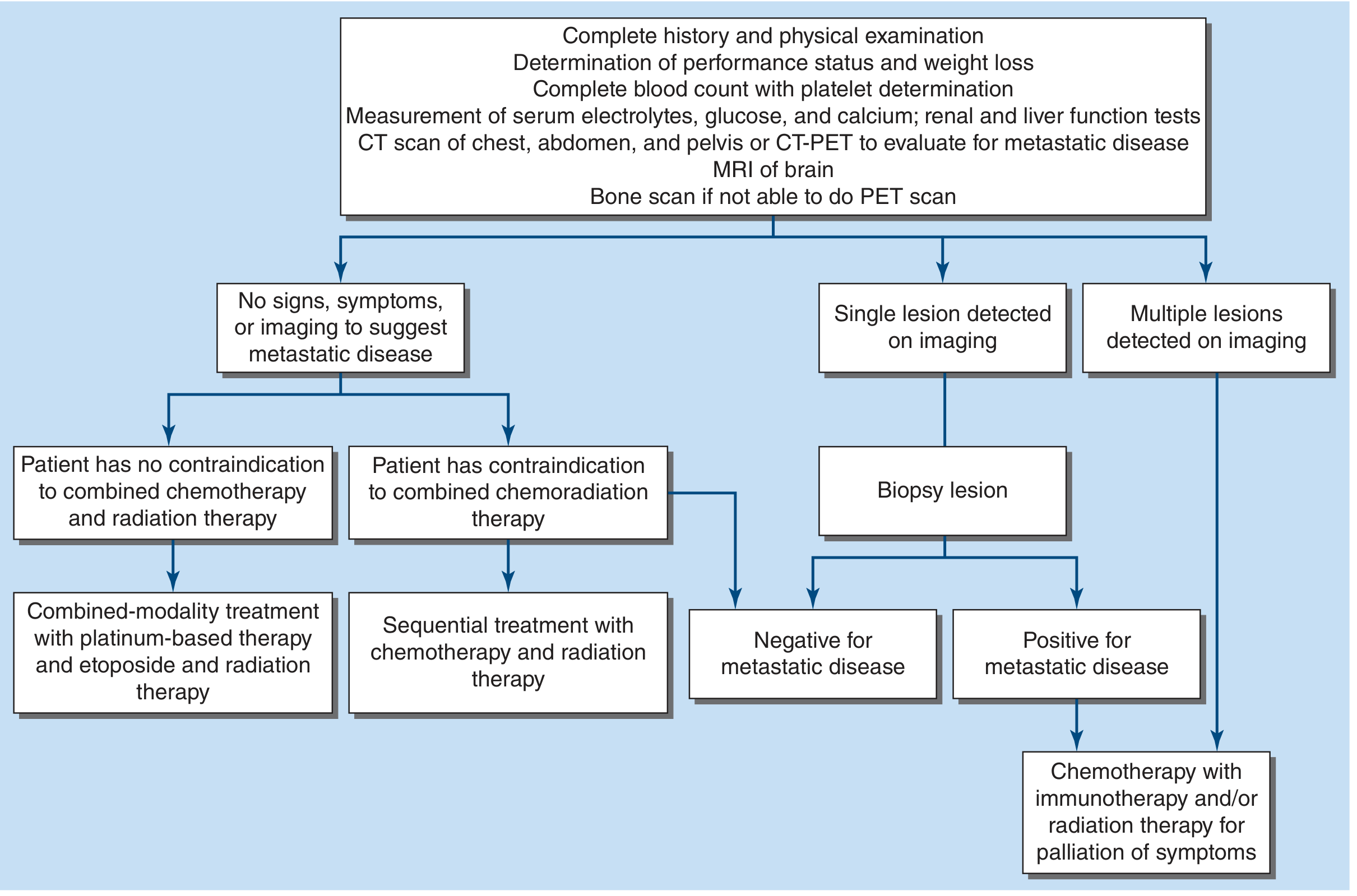
Figure: Algorithm for management of small-cell lung cancer - Harrison's Principles of Internal Medicine 22E
Limited-Stage SCLC
Standard of care: concurrent chemoradiotherapy
- Chemotherapy: Cisplatin + etoposide x 4 cycles (carboplatin is acceptable alternative)
- Thoracic radiation therapy (TRT): Concurrent preferred over sequential; ideally started by cycle 2
- 45 Gy twice-daily (1.5 Gy fractions) OR 70 Gy once-daily
- Twice-daily fractionation improves survival but increases grade 3 esophagitis
- Response rates: 85-90%; complete response 50-60%
- Median survival: 18-24 months; 2-year survival 40-50%; 5-year survival ~29-34%
- Combined modality therapy improves 3-year survival by ~5% vs chemotherapy alone
Surgery: Considered only for clinical stage I disease (T1-2 N0) after thorough metastatic evaluation and invasive mediastinal staging - <10% of all SCLC patients. If resected, platinum-based adjuvant chemotherapy is required. Retrospective series show 5-year survival of 30-50% for T1-2 N0 after resection.
- Harrison's Principles of Internal Medicine 22E, p. 673-674; Goldman-Cecil Medicine, p. 2020
Extensive-Stage SCLC
Standard of care: chemotherapy +/- immunotherapy
First-line regimens:
- Cisplatin or carboplatin + etoposide (4-6 cycles)
- Cisplatin or carboplatin + etoposide + atezolizumab (PD-L1 inhibitor; IMpower133 trial)
- Cisplatin or carboplatin + etoposide + durvalumab (PD-L1 inhibitor; CASPIAN trial)
- Carboplatin + etoposide + serplulimab
Two phase 3 RCTs (IMpower133, CASPIAN) demonstrated that adding a PD-L1 inhibitor to platinum-etoposide provides superior progression-free and overall survival. Disease recurs at a median of 4-6 months.
- Response rates: 75-85%; complete response only 15-25%
- Median survival: 7-12 months; 2-year survival <5%
Second-Line Therapy
For sensitive relapse (>3 months after initial therapy):
- Topotecan (IV or oral) - 20% response rate
- Lurbinectedin - 35% response rate, progression-free survival 3.5 months (FDA-approved)
- Platinum rechallenge
- Irinotecan, paclitaxel, docetaxel, vinorelbine, oral etoposide, gemcitabine
For refractory relapse (<90 days from platinum): Same agents but with low response rates.
Emerging Therapies
Tarlatamab - a bispecific T-cell engager (BiTE) targeting DLL3 (delta-like ligand 3) and CD3: 40% objective response rate, median PFS 4.9 months (DeLLphi-301 phase 2 study). Confirmatory phase 3 results are pending.
- Harrison's 22E, p. 673
Prophylactic Cranial Irradiation (PCI)
- Historically offered to all SCLC patients without progression on initial treatment
- A meta-analysis of 987 LS-SCLC patients in complete remission showed 5.4% improvement in overall survival with PCI
- Role is now controversial because original studies predated brain MRI staging
- In ES-SCLC responding to first-line therapy: observation without PCI did not reduce overall survival despite a higher rate of brain metastases
- Goldman-Cecil Medicine: PCI associated with modest improvement in 5-year survival for LS-SCLC achieving complete remission
Prognosis Summary
| Stage | Response Rate | Median Survival | 2-Year Survival |
|---|---|---|---|
| Limited | 85-90% (CR: 50-60%) | 18-24 months | 40-50% |
| Extensive | 75-85% (CR: 15-25%) | 7-12 months | <5% |
| Surgical T1-2 N0 | High | - | 30-50% (5-yr) |
Poor prognostic factors identified by the SWOG include: elevated serum LDH, older age, and presence of pleural effusion.
Recent Evidence Update
A recent network meta-analysis (PMID: 39397360) confirmed immunotherapy combined with chemotherapy improves outcomes in ES-SCLC. A 2025 meta-analysis (PMID: 41101157) evaluated surrogate endpoints for overall survival in ES-SCLC. A 2025 systematic review on brain metastases (PMID: 40615342) reviewed focal therapies for SCLC brain metastases - an important evolving area as PCI's role becomes more restricted.
Note: The role of immunotherapy in first-line ES-SCLC is now established (atezolizumab, durvalumab), and tarlatamab (DLL3-targeting BiTE) represents the most exciting emerging agent per current literature. SCLC's poor prognosis despite initial responsiveness remains a major clinical challenge.
This is a shared conversation. Sign in to Orris to start your own chat.