Diffrence between first, second and third degree heat block
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Finding Sources
Here is a detailed breakdown of the three degrees of atrioventricular (AV) heart block, based on Braunwald's Heart Disease, Rosen's Emergency Medicine, and Goldman-Cecil Medicine.
Degrees of Atrioventricular (AV) Heart Block
AV block occurs when conduction of atrial impulses to the ventricles is delayed or interrupted. It is classified into three degrees of increasing severity.
First-Degree AV Block
- Definition: Every atrial impulse IS conducted to the ventricles, but the conduction time is prolonged. Nothing is truly "blocked" - it is more accurately a conduction delay.
- ECG finding: PR interval > 0.20 seconds (200 ms) in adults, with every P wave followed by a QRS complex. PR intervals as long as 1.0 second have been recorded.
- Site of delay: Usually within the AV node itself. If the QRS is normal in width, the delay is almost always in the AV node. If the QRS shows a bundle branch block pattern, the delay may be in the His-Purkinje system.
- Clinical significance: Generally benign, but notably 50% or more of patients with first-degree AV block have detectable higher-degree AV block on prolonged monitoring, or develop higher-grade block within about a year.
- Causes: Vagal tone, inferior MI, digoxin, beta-blockers, athletic conditioning, inflammatory conditions (myocarditis, Lyme disease).
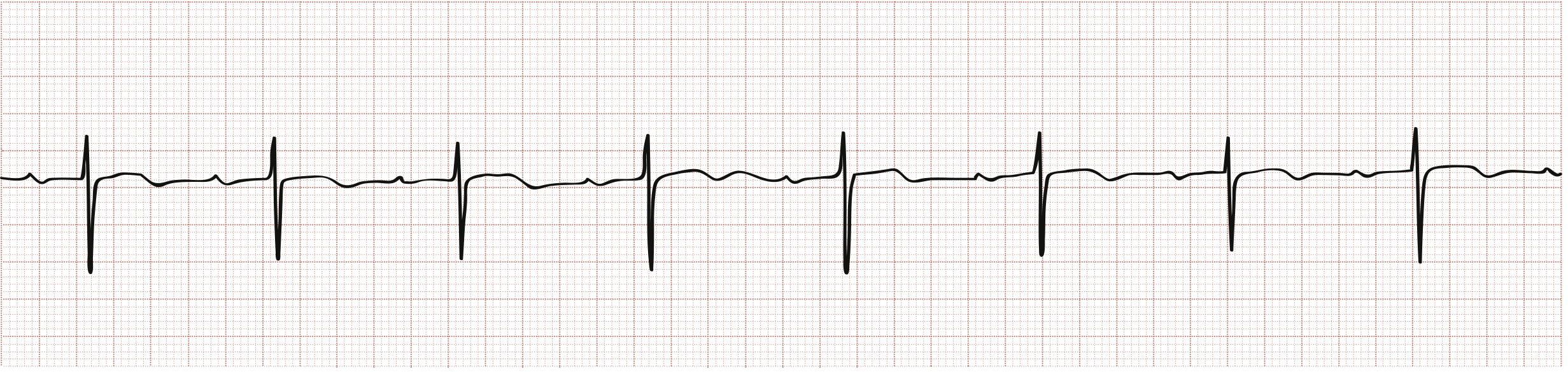
ECG Example - First-Degree AV Block (note the prolonged PR interval before each QRS):
Second-Degree AV Block
Some, but not all, atrial impulses reach the ventricles (some P waves are not followed by a QRS). It has two distinct subtypes:
Mobitz Type I (Wenckebach)
| Feature | Detail |
|---|---|
| PR interval | Progressively lengthens until one P wave is blocked (no QRS) |
| QRS | Usually narrow |
| Site | Usually AV node |
| Common causes | Inferior MI, digoxin, beta-blockers, vagotonia |
| Response to atropine/exercise | Improves |
| Response to carotid massage | Worsens |
| Prognosis | Generally benign, often reversible |
The key pattern: PR gets longer, then a beat drops, then the cycle resets (the first PR after the dropped beat is shorter than the last PR before the drop).
Mobitz Type II
| Feature | Detail |
|---|---|
| PR interval | Constant (does not lengthen before the block) |
| QRS | Wide (usually - bundle branch block pattern) |
| Site | Infranodal (His-Purkinje system) |
| Common causes | Anterior MI, Lenegre/Lev disease, cardiomyopathy |
| Response to atropine/exercise | May worsen |
| Response to carotid massage | May improve conduction ratio |
| Prognosis | More serious - can suddenly progress to complete heart block |
2:1 AV Block
When there are 2 P waves for every 1 QRS, it can be difficult to distinguish Mobitz I from II. Clues:
- Prolonged PR + narrow QRS → more likely Mobitz I (AV nodal)
- Normal PR + wide QRS (bundle branch block pattern) → more likely Mobitz II (infranodal)
Third-Degree AV Block (Complete Heart Block)
- Definition: No atrial impulses are conducted to the ventricles at all. Atrial and ventricular activity are completely independent (AV dissociation).
- ECG finding: P waves and QRS complexes march through at their own independent rates, with the atrial rate typically FASTER than the ventricular rate. The R-R interval is longer than the P-P interval. P waves bear no consistent relationship to QRS complexes.
- Escape rhythm: The ventricles are driven by a subsidiary escape pacemaker:
- Junctional (above His bundle): narrow QRS, rate 45-60 beats/min - more stable
- Ventricular (at or below His bundle): wide QRS, rate 30-45 beats/min - less reliable, hemodynamically compromised
- If no escape rhythm: asystole and cardiac arrest.
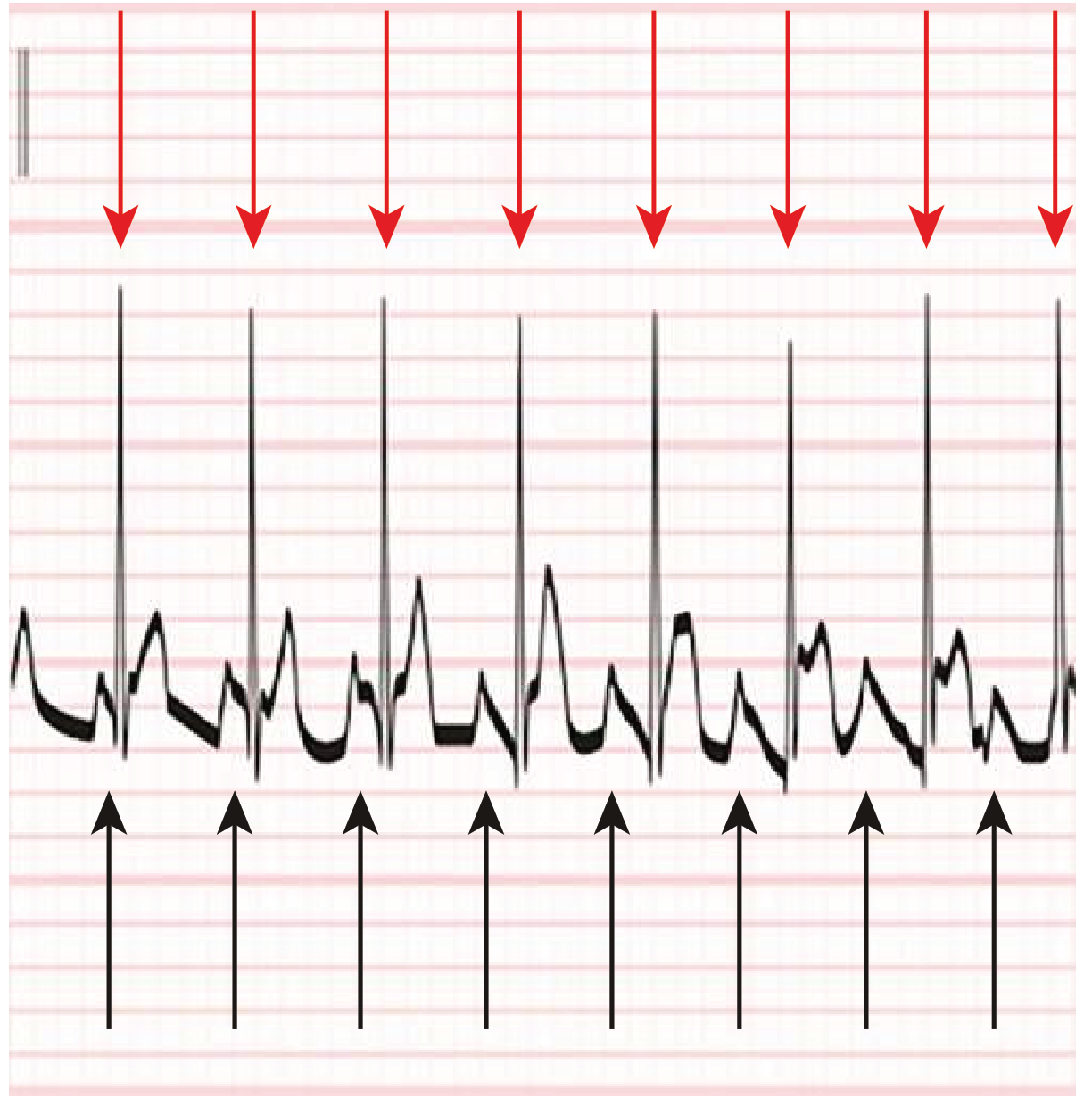
ECG Example - Third-Degree (Complete) Heart Block (red arrows = atrial P waves, black arrows = ventricular QRS complexes - completely dissociated):
- Causes: Senescent degeneration of the conduction system, acute ischemia (inferior or anterior MI), Lyme disease, Chagas disease, drug toxicity, congenital.
- Special association: Complete heart block with atrial fibrillation showing a slow, regular ventricular response ("regularized AF") = classic sign of digoxin toxicity.
Summary Comparison Table
| Feature | 1st Degree | 2nd Degree - Mobitz I | 2nd Degree - Mobitz II | 3rd Degree |
|---|---|---|---|---|
| P:QRS ratio | 1:1 | Variable (some P waves blocked) | Variable (some P waves blocked) | No relationship |
| PR interval | Prolonged, fixed | Progressively lengthens then drops | Fixed (normal or prolonged) | No fixed PR |
| QRS width | Normal | Normal | Wide (usually) | Narrow or Wide (escape) |
| Site of block | AV node | AV node | His-Purkinje (infranodal) | Anywhere |
| Ventricular rate | Normal | Slightly irregular | Irregular | 30-60 (escape) |
| Risk of progression | Low | Low | High | N/A (already complete) |
| Pacemaker needed | No | Rarely | Yes (or standby) | Yes |
| Atropine | May shorten PR | Improves | May worsen | Usually ineffective |
Management Points
- 1st degree: No treatment needed; monitor.
- Mobitz I: Usually no treatment; identify and remove reversible causes (e.g., digoxin, beta-blockers).
- Mobitz II: Pacing capability must be immediately available; high risk of progression to complete block. Permanent pacemaker is usually indicated.
- 3rd degree (complete block): Symptomatic patients with hypoperfusion require temporary transcutaneous or transvenous pacing urgently. Atropine is generally not effective and should be avoided in ischemia-related block. Permanent pacemaker is required.
Sources: - Braunwald's Heart Disease, pp. 155-157 | - Rosen's Emergency Medicine, pp. 1847-1888 | - Goldman-Cecil Medicine, pp. 2943-2959
Give me a list of ECGs containing first degree, second degree and third degree AV blocks. I will find out the answer. Give the images.
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I have all the ECG images. Here is a mixed list from multiple textbooks - try to identify each one before checking the answer!
ECG Practice Set - AV Heart Blocks
The ECGs below are unlabelled. Each one shows either a 1st, 2nd (Mobitz I or Mobitz II), or 3rd degree AV block. Try to identify each before revealing the answer.
ECG 1
Answer
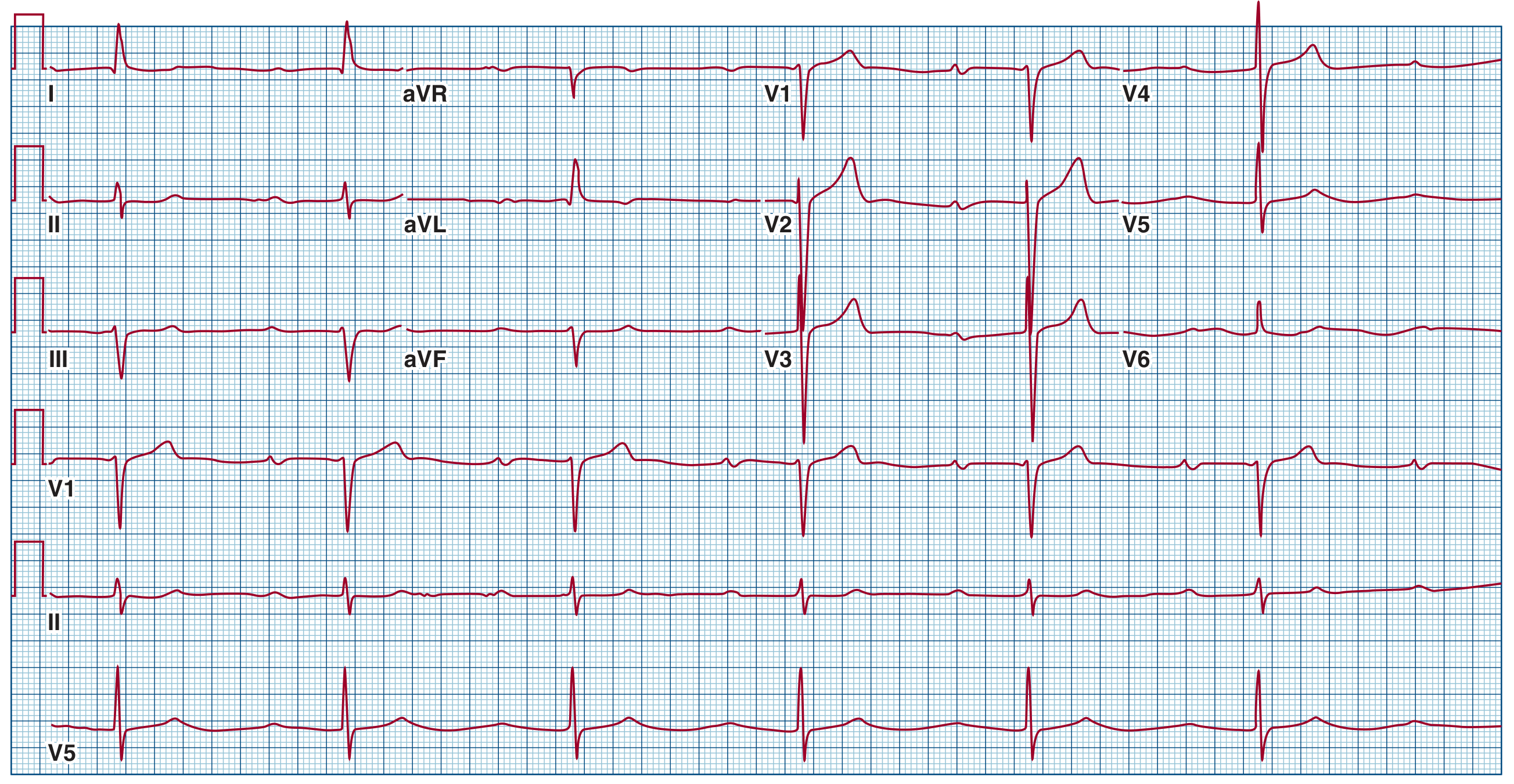
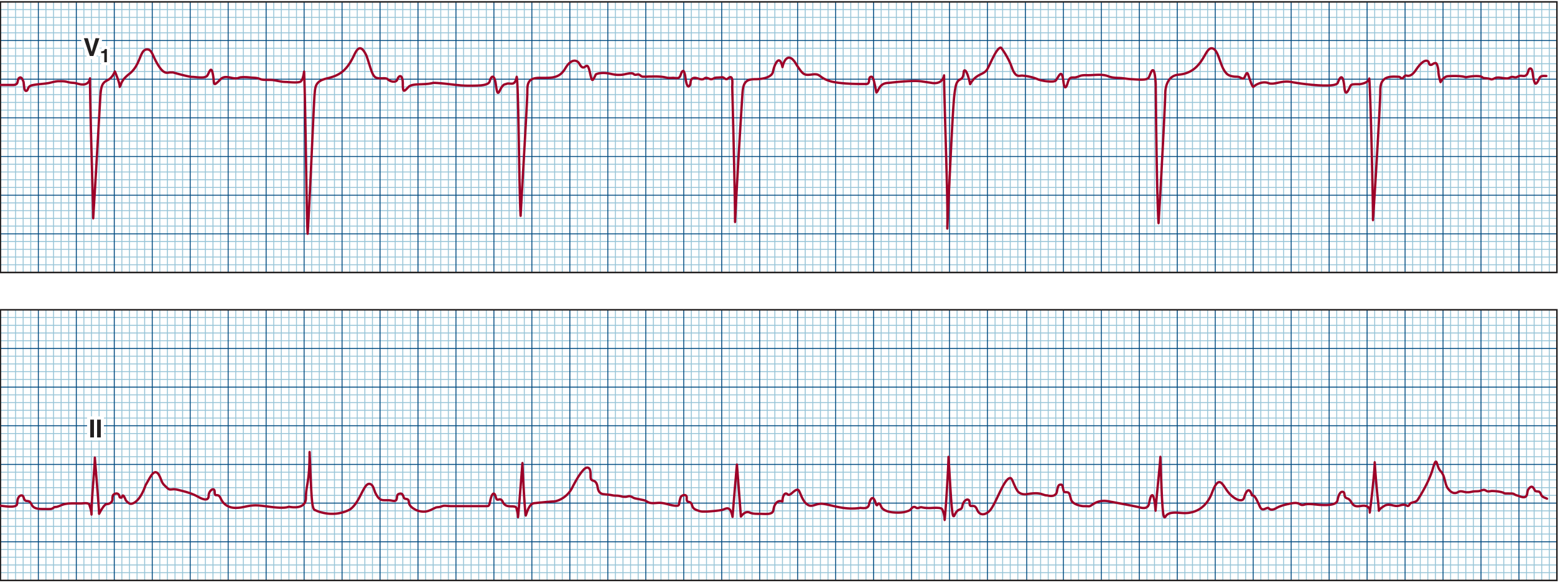
**First-Degree AV Block.** Note the prolonged PR interval of 520 ms across all leads. Every P wave is followed by a QRS. Source: Fuster & Hurst's The Heart.ECG 2
Answer
**First-Degree AV Block.** Prolonged PR interval with every P wave conducting. Source: Rosen's Emergency Medicine.ECG 3

Answer
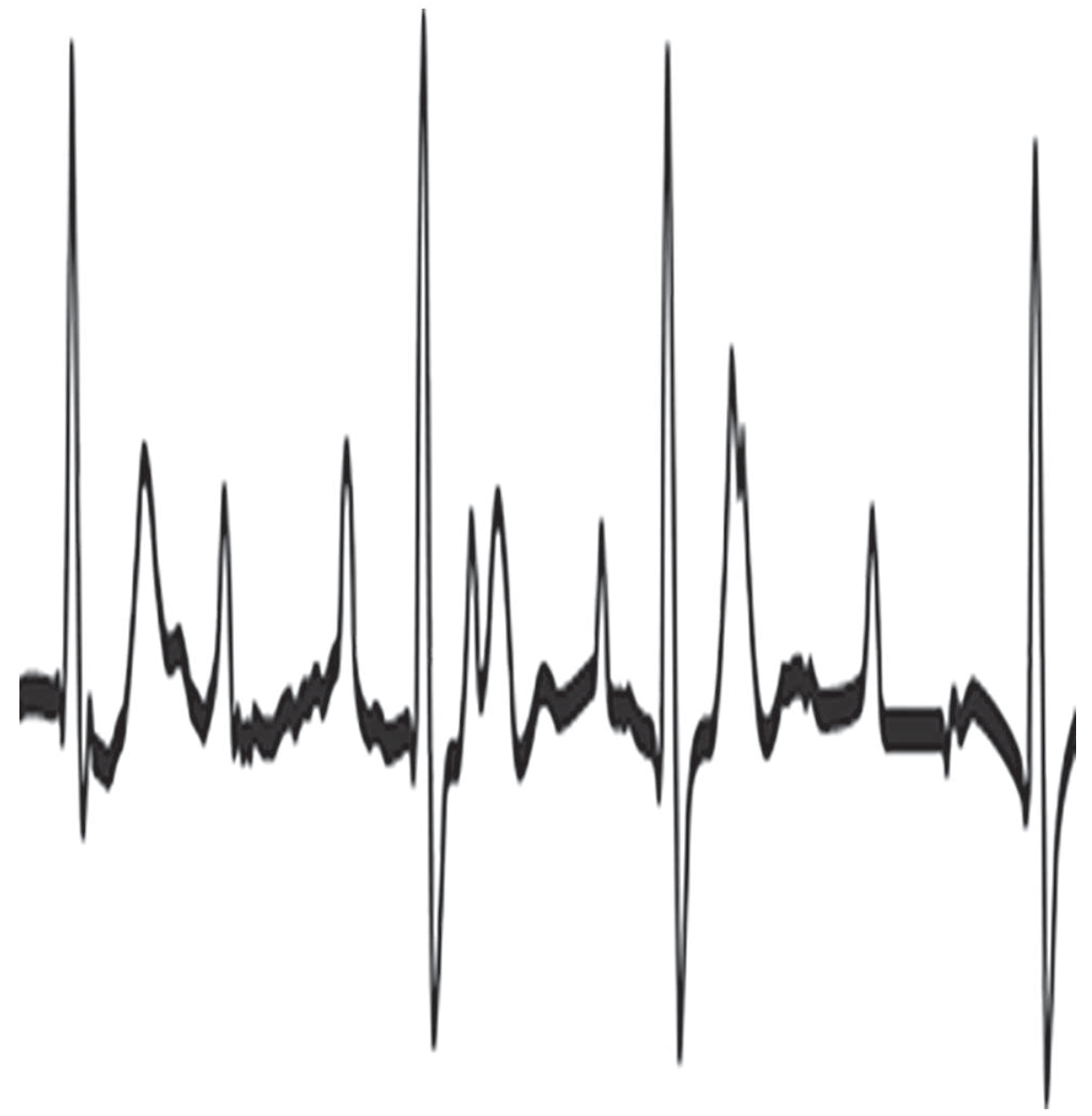
**Second-Degree AV Block - Mobitz Type I (Wenckebach).** A 6.5 AV Wenckebach periodicity is shown. The PR interval progressively lengthens with a decreasing increment, R-R intervals shorten, and then a beat is dropped. The first PR after the dropped beat is shorter than the last PR before. Source: Fuster & Hurst's The Heart.ECG 4
Answer
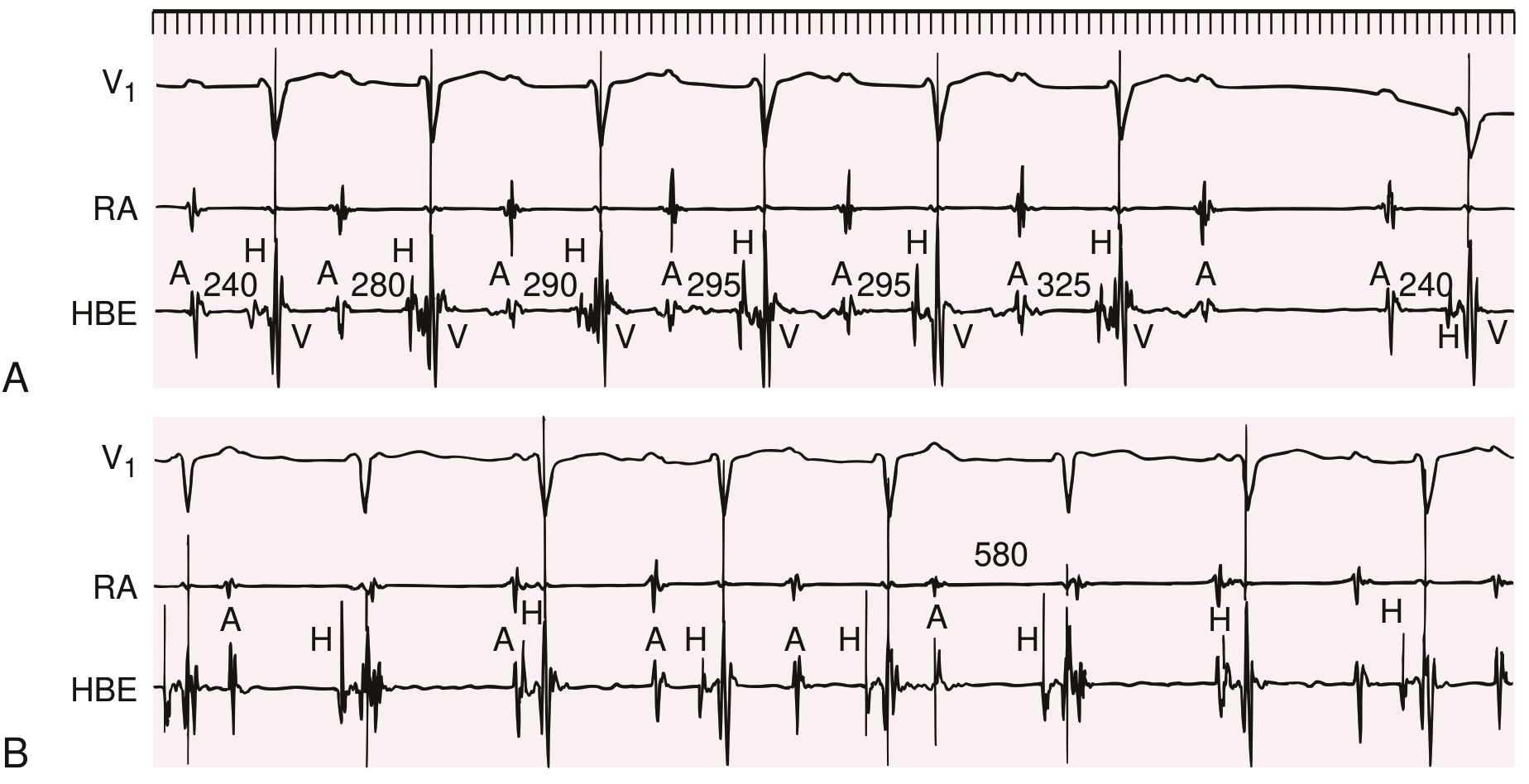
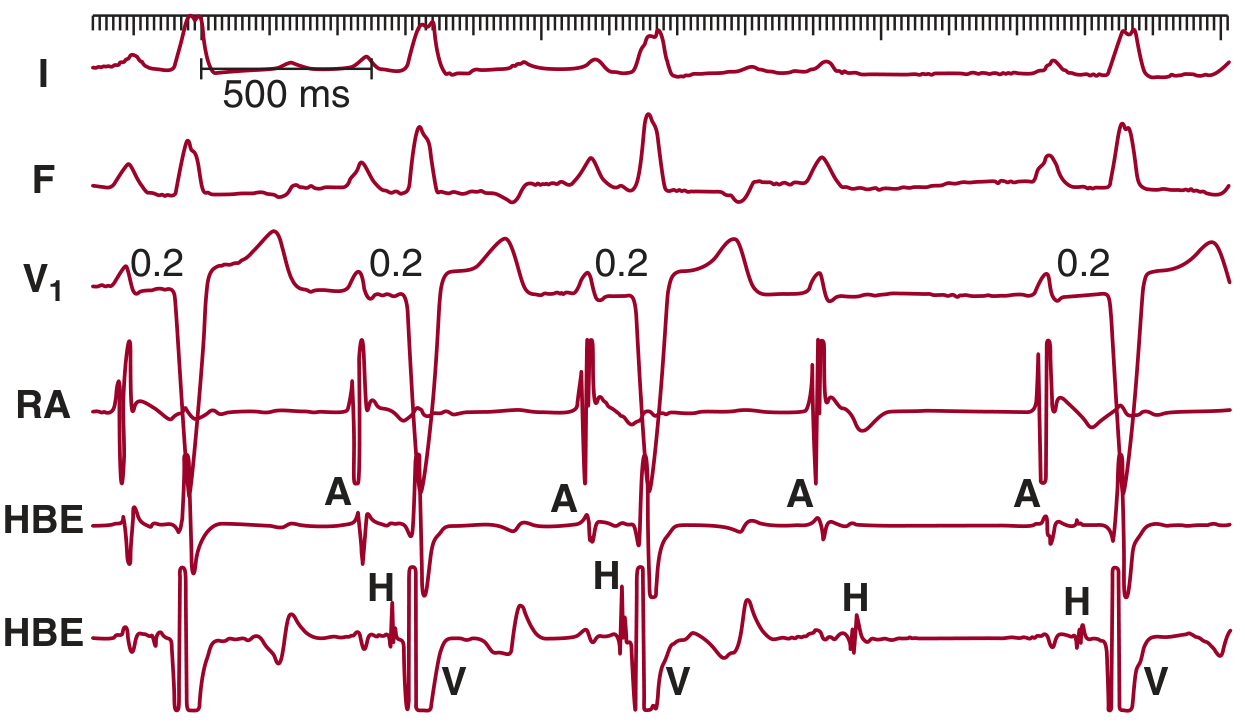
**Second-Degree AV Block - Mobitz Type I (Wenckebach), Panel A.** His bundle recording confirms delay within the AV node (prolonged AH interval). Progressive PR prolongation culminates in a non-conducted P wave. Source: Braunwald's Heart Disease.ECG 5
Answer
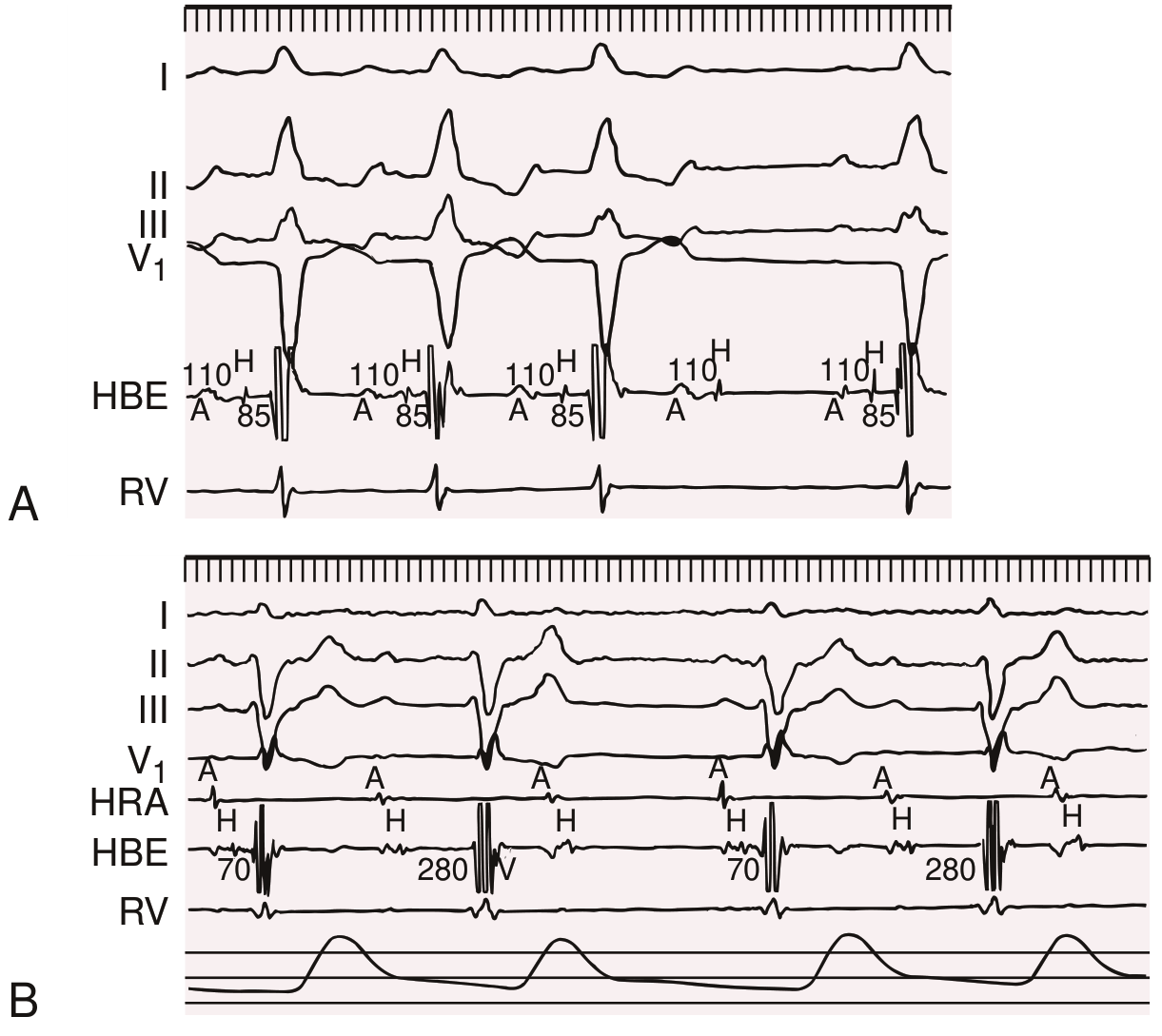
**Second-Degree AV Block - Mobitz Type II (Panel A).** PR intervals are constant at 0.2 seconds with LBBB morphology; the 4th P wave suddenly fails to conduct. His bundle electrogram confirms block below the His bundle. Source: Fuster & Hurst's The Heart.ECG 6
Answer
**Second-Degree AV Block - Mobitz Type II (Panel A) with His-Purkinje block.** Sudden block with constant A-H and H-V intervals and constant PR interval. LBBB present. Source: Braunwald's Heart Disease.ECG 7
Answer
**High-Grade (Advanced) Second-Degree AV Block.** Multiple consecutive non-conducted P waves (some buried in QRS complexes), with only occasional conduction. Source: Goldman-Cecil Medicine.ECG 8
Answer
**Third-Degree AV Block (Complete Heart Block) with narrow-complex escape rhythm.** P waves and QRS complexes are completely dissociated. The escape rhythm is junctional (narrow QRS), indicating block at the AV node level. Source: Fuster & Hurst's The Heart.ECG 9
Answer
**Third-Degree AV Block (Complete Heart Block).** Red arrows mark atrial beats (P waves), black arrows mark ventricular QRS complexes - completely dissociated. ST elevation in leads III and aVF indicates an acute inferior MI as the cause. Source: Goldman-Cecil Medicine.9 ECGs total - 2 first-degree, 4 second-degree (including one high-grade), and 2 third-degree. Good luck!
This is a shared conversation. Sign in to Orris to start your own chat.