Reading File
Finding Sources
analyse_media
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Here is a detailed breakdown of everything on the page, expanded with textbook knowledge:
Pelvic Axis, Pelvic Diameters, and Key Points for Labour
What the Page Covers
The page is from an obstetrics textbook and discusses:
- The obstetric/pelvic axis
- Pelvic diameters and their clinical relevance
- Points to ponder - key exam/clinical facts
1. Pelvic Axis (Curve of Carus / Obstetric Axis)
The pelvic axis (also called the obstetric axis or curve of Carus) is the imaginary curved line a baby's head follows as it descends through the birth canal.
- It is obtained by joining the axes of the inlet, pelvic cavity, and outlet - creating a J-shaped curve
- The direction of movement changes at the level of the ischial spines: the head moves downward and backward first, then shifts to downward and forward
- The curve has convexity fitting the sacral curvature (i.e., it curves anteriorly, following the concavity of the sacrum)
- It is also called the "curve of Carus" after the anatomist Karl Gustav Carus
Why it matters clinically: Understanding this axis helps in instrumental deliveries (forceps, vacuum) - the instrument must follow this curve when applied.
2. Pelvic Diameters
"Pelvic diameters vary from one patient to the other just as the height and weight. During labour the absolute size of the pelvis is not significant, but the size relative to the foetal head is vital."
This is a key obstetric principle - cephalopelvic proportion matters more than raw measurements. A large fetus in a normal pelvis can cause the same problem as a small fetus in a contracted pelvis.
Key pelvic diameters at each level:
| Level | Important Diameter | Normal Value |
|---|---|---|
| Inlet | Obstetric conjugate (AP) | ≥10 cm |
| Inlet | Transverse | ~13 cm |
| Mid-pelvis (cavity) | Interspinous (transverse) | ≥10 cm |
| Outlet | Bi-ischial (transverse) | ≥8 cm |
3. Points to Ponder (Exam Focus)
Point 1: Obstetric Conjugate
"Obstetric conjugate is the antero-posterior diameter which the foetus must negotiate while descending, hence important."
The obstetric conjugate is the shortest AP diameter of the pelvic inlet - the smallest distance between the sacral promontory and the posterior surface of the pubic symphysis (not the top of the symphysis). Normal value: ≥10 cm.
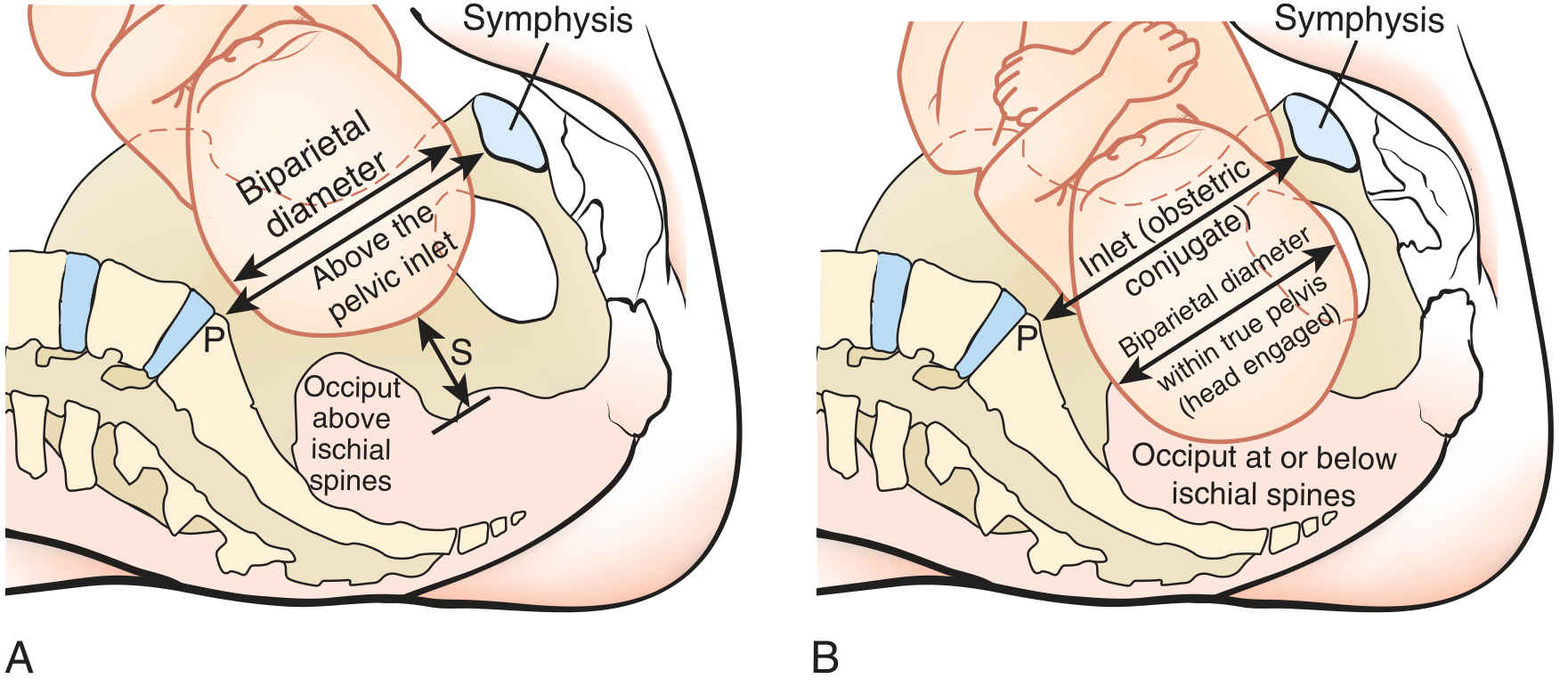
As seen in the diagram above:
- Panel A: Fetal head above the pelvic inlet - occiput above ischial spines (not yet engaged)
- Panel B: Biparietal diameter has descended below the inlet (obstetric conjugate) - occiput at or below ischial spines = engaged
The obstetric conjugate cannot be measured directly on clinical exam; it is estimated as: diagonal conjugate minus 1.5-2 cm.
Point 2: Head Engages in the Oblique Diameter
"The head (presenting part) commonly engages in oblique diameters at the pelvic inlet."
At the inlet, the widest diameter is the transverse, but the head does not engage in the transverse - it engages in one of the two oblique diameters (~12 cm each). This is because:
- The ala of the sacrum restricts the posterolateral dimension
- Engaging obliquely allows the occiput to rotate anteriorly as it descends (internal rotation)
The left oblique diameter is more common for engagement (occiput commonly in the left occipito-anterior position, LOA).
Point 3: Plane of Least Dimensions = Most Arrests
"Plane of least dimensions (at mid-pelvis) is the plane where most cases of arrest in labour occur."
The plane of least dimensions (mid-pelvic plane) passes through:
- The lower border of the pubic symphysis anteriorly
- The ischial spines laterally (interspinous diameter ~10 cm)
- The tip of the sacrum posteriorly
This is the narrowest part of the birth canal. Most arrests of labour - deep transverse arrest (DTA) being the classic example - happen here, when the fetal head fails to rotate from the transverse to an anterior or posterior position.
| Type of Arrest | Level | Cause |
|---|---|---|
| Deep transverse arrest | Mid-pelvis | Head stuck in transverse, fails internal rotation |
| Occipito-posterior arrest | Mid-pelvis | Head in OP position, cannot rotate |
Summary of Clinical Relevance
| Concept | Clinical Implication |
|---|---|
| Curve of Carus / Obstetric axis | Guides direction of traction in forceps/vacuum delivery |
| Obstetric conjugate | Most important diameter to assess at pelvic inlet; <10 cm = contracted inlet |
| Relative size (fetal head vs. pelvis) | Cephalopelvic disproportion (CPD) diagnosed clinically |
| Oblique engagement | Normal; enables subsequent internal rotation |
| Plane of least dimensions | Most common site for obstructed labour and arrest disorders |
- Pfenninger and Fowler's Procedures for Primary Care, p. 6678 (engagement and obstetric conjugate)

IMG_1112.jpg
Can you explain it for my exam for 10 mark questions
Reading File
analyse_media
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Now I have everything needed to write a comprehensive 10-mark answer. Let me also note the critical clinical reasoning for this case before writing the answer.
Key clinical logic for this case:
- 55-year-old female + ringing (tinnitus) in right ear x 6 months
- AC > BC in right ear = Positive Rinne = sensorineural hearing loss (or normal hearing)
- ABC (Absolute Bone Conduction) normal = Schwabach test normal = cochlear/inner ear function matches examiner = confirms the hearing loss is NOT due to cochlear damage OR the cochlea is intact
- Wait - if ABC is normal, that means bone conduction is intact/normal, and since AC > BC (positive Rinne), this is consistent with normal hearing in the right ear
- Tinnitus with normal hearing tests in a 55-year-old female = Tinnitus as the primary complaint, possibly early sensorineural or functional tinnitus
Actually, re-reading: AC > BC = Positive Rinne = either normal OR SNHL. ABC normal = bone conduction is equal to examiner's = cochlea is working normally. Combined = the ear has normal cochlear function but the patient has tinnitus. This is a presentation of subjective tinnitus - possibly early presbycusis-related or idiopathic tinnitus without measurable hearing loss yet.
10-Mark Exam Answer
Clinical Case Interpretation
Patient: 55-year-old female
Complaint: Ringing sound (tinnitus) in right ear x 6 months
Rinne test (right ear): AC > BC (Positive Rinne)
ABC (Absolute Bone Conduction / Schwabach test): Normal
DIAGNOSIS: Subjective Tinnitus (Right Ear)
The tuning fork findings tell you:
- AC > BC (Positive Rinne): Air conduction is better than bone conduction in the right ear. This is the normal physiological finding (AC is normally ~30 dB better than BC). It rules out a conductive hearing loss in the right ear.
- ABC normal: The Schwabach test compares the patient's bone conduction with that of a normal-hearing examiner. A normal ABC means the patient's cochlear (inner ear) function is intact and equal to normal. This rules out significant sensorineural hearing loss.
Combined interpretation: No conductive loss, no sensorineural loss - but the patient has tinnitus. This is tinnitus with clinically normal hearing - the earliest/most common presentation.
EXPLANATION OF THE CONDITION (According to Modern Understanding)
Definition
Tinnitus is the perception of sound in the absence of an external acoustic stimulus. It is derived from the Latin tinnire - "to ring." It can be unilateral or bilateral, continuous or intermittent.
Classification
| Type | Description |
|---|---|
| Subjective tinnitus | Heard only by the patient (most common, ~95%) |
| Objective tinnitus | Can be heard by the examiner (rare - vascular/muscular causes) |
This patient has subjective, unilateral tinnitus of the right ear.
Modern Pathophysiology
Modern understanding recognizes tinnitus as primarily a central auditory nervous system phenomenon, not purely a cochlear problem:
- Peripheral trigger: Subclinical cochlear hair cell damage (often at high frequencies, not yet detectable on tuning fork tests) causes reduced input to the auditory nerve
- Central gain increase: The central auditory cortex, deprived of normal input, upregulates its own spontaneous firing rate - a process called maladaptive neuroplasticity
- Phantom sound perception: This aberrant, increased spontaneous neural activity is interpreted by the brain as sound - the "ringing" the patient hears
- Limbic system involvement: In chronic tinnitus, the limbic system (emotional processing) and prefrontal cortex become involved, leading to distress, sleep disturbance, and anxiety
This is analogous to phantom limb pain - the tinnitus is real to the patient even though there is no external sound.
Common Causes in This Age Group (55-year-old female)
| Cause | Features |
|---|---|
| Early presbycusis (age-related) | Most likely; subclinical high-frequency SNHL before audiogram becomes abnormal |
| Noise-induced | History of loud noise exposure |
| Otosclerosis | Would give BC > AC (negative Rinne) - ruled out here |
| Meniere's disease | Would have vertigo + fullness + fluctuating SNHL |
| Acoustic neuroma | Must be excluded - especially with unilateral tinnitus |
| Cardiovascular | Hypertension, atherosclerosis can cause tinnitus |
| Drugs (ototoxic) | NSAIDs, aminoglycosides, loop diuretics, quinine |
Why ABC is Normal
The Schwabach (ABC) test compares the patient's bone conduction to a normal examiner. A normal ABC means the cochlea is functioning normally at the time of testing. In early tinnitus, the ABC may be normal because:
- The cochlear damage is subclinical (affecting only the basal turn, high frequencies not tested by standard 512 Hz tuning fork)
- The tinnitus is central in origin rather than purely cochlear
Investigations to Order
- Pure Tone Audiometry (PTA) - gold standard; may show high-frequency dip at 4000 Hz (noise notch) or sloping loss
- Tympanometry - to rule out middle ear pathology
- Speech Discrimination Score - to assess neural involvement
- MRI Brain with contrast (internal acoustic meatus) - mandatory for unilateral tinnitus to exclude acoustic neuroma
- Otoacoustic Emissions (OAE) - tests outer hair cell function; may be abnormal even when audiogram appears normal
Management (Modern)
- Counseling and reassurance - most important first step; explain the benign nature
- Sound therapy - white noise generators/maskers reduce central gain
- Cognitive Behavioral Therapy (CBT) - best evidence-based treatment for chronic tinnitus distress
- Tinnitus Retraining Therapy (TRT) - combines sound therapy + counseling; aims for habituation
- Treat underlying cause - control hypertension, stop ototoxic drugs, hearing aids if SNHL present
- Drug therapy (limited evidence) - melatonin for sleep, antidepressants for depression comorbidity
Tuning Fork Summary Table (High-Yield for Exam)
| Test | Normal | Conductive HL | SNHL |
|---|---|---|---|
| Rinne | AC > BC | BC > AC (Negative) | AC > BC (Positive) |
| Weber | Midline | Lateralizes to affected ear | Lateralizes to normal ear |
| ABC (Schwabach) | Normal | Prolonged (BC better than examiner) | Reduced (BC worse than examiner) |
In this patient: Positive Rinne + Normal ABC = No hearing loss detected = Tinnitus is the primary diagnosis.
Key exam points to remember:
- AC > BC = Positive Rinne = rules out conductive loss
- Normal ABC = intact cochlear function = rules out SNHL
- Unilateral tinnitus in any adult must be investigated to exclude acoustic neuroma (MRI IAM)
- Modern pathophysiology = central maladaptive neuroplasticity, not just a cochlear problem
- Best treatment evidence = CBT + TRT (not drugs)
Sources: Cummings Otolaryngology Head and Neck Surgery; Shambaugh Surgery of the Ear; Scott-Brown's Otorhinolaryngology Head & Neck Surgery; Goldman-Cecil Medicine
Tinnitus
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have everything I need for a comprehensive 10-mark answer. Here it is:
TINNITUS - Full 10-Mark Exam Answer
Definition
Tinnitus is the perception of sound in the absence of an external acoustic source. The word comes from the Latin tinnire meaning "to ring." It is a symptom, not a disease - and can arise from multiple causes at various levels of the auditory pathway.
- Affects up to 50 million adults in the USA; ~10% of adults have clinically significant tinnitus
- Only ~20% find it bothersome enough to seek treatment
- ~28% of acute tinnitus (< 6 months) resolves spontaneously
Classification
Tinnitus is classified along three key axes:
1. Subjective vs. Objective
| Feature | Subjective Tinnitus | Objective Tinnitus |
|---|---|---|
| Who hears it? | Patient only | Patient AND examiner (via stethoscope) |
| Prevalence | ~98.5% of all tinnitus | Rare (~1.5% at tertiary centres) |
| Cause | Central auditory system dysfunction | Real sound source - vascular, muscular, TMJ |
| Examples | SNHL, presbycusis, noise-induced | AV fistula, glomus jugulare, palatal myoclonus |
2. Pulsatile vs. Non-Pulsatile
| Feature | Pulsatile | Non-Pulsatile |
|---|---|---|
| Character | Rhythmic, beats with pulse | Continuous ringing, buzzing, hissing, roaring |
| Type | Can be subjective or objective | Almost always subjective |
| Causes | Vascular anomalies, hypertension, AV malformation | SNHL, presbycusis, Meniere's, ototoxicity |
3. Primary vs. Secondary
- Primary tinnitus: No identifiable underlying cause; may or may not be associated with SNHL
- Secondary tinnitus: Due to a specific identifiable cause (outside of SNHL)
Most common type in clinical practice: Subjective, non-pulsatile, primary tinnitus - accounts for ~90% of all tinnitus referrals
Etiology / Causes
| Site/System | Causes |
|---|---|
| Inner ear | Presbycusis, noise-induced HL, Meniere's disease, SNHL |
| Middle ear | Otosclerosis, cholesteatoma, ossicular abnormalities |
| External ear | Cerumen impaction, canal occlusion |
| Infections | Otitis media, labyrinthitis, herpes zoster oticus |
| Ototoxic drugs | Aminoglycosides, loop diuretics (furosemide), NSAIDs, quinine, cisplatin |
| Neurological | Acoustic neuroma (VIII nerve schwannoma), MS, migraine |
| Vascular | AV fistula, glomus jugulare, hypertension, atherosclerosis |
| Musculoskeletal | TMJ disorder, palatal myoclonus |
| Metabolic/Endocrine | Hypothyroidism, diabetes mellitus, hyperinsulinemia |
| Psychological | Anxiety, depression (exacerbate and are exacerbated by tinnitus) |
| Social habits | Alcohol, nicotine, caffeine |
| Autoimmune | SLE, rheumatoid arthritis, systemic sclerosis |
Pathophysiology (Modern Understanding)
The modern view of tinnitus is that it is primarily a central nervous system phenomenon, not simply a cochlear problem:
Step 1 - Peripheral trigger:
A cochlear insult (noise, aging, ototoxic drug) causes loss or damage to cochlear hair cells, particularly in the high-frequency basal turn. This reduces afferent input to the auditory nerve.
Step 2 - Central gain increase (Maladaptive Neuroplasticity):
The central auditory system, deprived of normal peripheral input, upregulates its own spontaneous firing rate in an attempt to compensate. This is called increased central gain. Imaging studies show enhanced primary auditory cortex activity in tinnitus patients, correlating with perceived intensity.
Step 3 - Aberrant tonotopic reorganization:
Functional MRI and MEG studies show expanded cortical representation of the frequencies corresponding to the hearing loss region. The auditory cortex essentially "fills in" the missing input with spontaneous activity.
Step 4 - Phantom sound perception:
This aberrant, increased spontaneous neural activity is interpreted by the higher auditory cortex as real sound - producing the phantom "ringing" the patient experiences. This is analogous to phantom limb pain.
Step 5 - Limbic system involvement (bothersome tinnitus):
In chronic or bothersome tinnitus, the tinnitus signal becomes linked to the limbic system (amygdala) and prefrontal cortex through learned emotional associations, leading to:
- Sleep disturbance
- Concentration difficulty
- Anxiety and depression
- Reduced quality of life
This is why psychological treatment (CBT) is more effective than any drug for bothersome tinnitus.
Clinical Features
- Ringing, buzzing, hissing, roaring, or clanging sounds
- Quality gives a clue to cause:
- Roaring/hissing = otosclerosis
- Fluctuating, variable quality = Meniere's disease
- High-pitched ringing = auditory nerve lesion (acoustic neuroma)
- Low-pitched = Meniere's (early)
- Pulsatile = vascular cause
- Associated symptoms: hearing loss, vertigo, aural fullness, otalgia
- Red flags (need urgent investigation):
- Unilateral tinnitus persisting > 6 months
- Associated asymmetric SNHL
- Pulsatile tinnitus
- Focal neurological signs
Investigations
| Investigation | Purpose |
|---|---|
| Pure Tone Audiometry (PTA) | Mandatory for persistent unilateral tinnitus; identifies type and degree of HL |
| Speech Discrimination Score | Assesses neural (retrocochlear) involvement |
| Tympanometry | Rules out middle ear pathology |
| Otoacoustic Emissions (OAE) | Tests outer hair cell function; may be abnormal before audiogram |
| Tinnitus Handicap Inventory (THI) | Quantifies impact on quality of life; guides treatment |
| MRI Brain with IAM (contrast) | Mandatory for unilateral tinnitus - to exclude acoustic neuroma |
| CT temporal bone | For pulsatile tinnitus - assess for vascular anomalies, glomus tumor |
| Blood tests | TFTs, FBS, lipids, BP - assess cardiovascular/metabolic causes |
| Drug history review | Identify ototoxic medications |
Management
Step 1: Treat the Cause (Secondary Tinnitus)
- Remove cerumen - may immediately resolve tinnitus
- Stop ototoxic drugs
- Control hypertension
- Treat middle ear infection/otosclerosis
- Surgical excision if glomus tumor
Step 2: Patient Education and Reassurance
- Explain the benign nature of primary tinnitus
- Explain the central pathophysiology
- Counsel that tinnitus often habituates over time
- This alone significantly reduces distress
Step 3: Sound Therapy
- White noise maskers/sound generators - reduce central gain by providing ambient input
- Hearing aids (if SNHL present) - amplify ambient sound, effectively masking tinnitus
- Recorded masking sounds (rainfall, white noise) for sleep
Step 4: Psychological Therapies (Best Evidence)
| Therapy | Mechanism | Evidence |
|---|---|---|
| Cognitive Behavioral Therapy (CBT) | Reframes emotional response to tinnitus; breaks limbic linkage | Best evidence; first-line for bothersome tinnitus |
| Tinnitus Retraining Therapy (TRT) | Combines counseling + sound therapy; aims for habituation | Strong evidence; used widely |
Step 5: Pharmacotherapy (Limited Role)
- No medications are approved for tinnitus in the USA or Europe
- Benzodiazepines (diazepam 2-5 mg TDS) - temporary symptomatic relief only
- Tricyclic antidepressants (amitriptyline 25-75 mg HS) - for associated depression/sleep
- Melatonin - for sleep disturbance
- Note: No drug has been shown to cure tinnitus
Step 6: Emerging/Invasive Options (Severe, Refractory)
- Transcranial magnetic stimulation (TMS) - modulates auditory cortex activity
- Cochlear implants - for profound SNHL with tinnitus; often dramatically reduces tinnitus
- Transtympanic corticosteroids - for sudden SNHL-associated tinnitus
Summary (High-Yield Points for Exam)
| Key Point | Detail |
|---|---|
| Definition | Perception of sound without external source |
| Most common type | Subjective, non-pulsatile, primary (~90%) |
| Pathophysiology | Central maladaptive neuroplasticity, NOT just cochlear |
| Most common cause | Presbycusis / noise-induced SNHL |
| Dangerous diagnosis to exclude | Acoustic neuroma (VIII nerve schwannoma) |
| When to do MRI | Unilateral tinnitus > 6 months, asymmetric SNHL |
| Best treatment evidence | CBT (Cognitive Behavioral Therapy) |
| Drug approval status | No drug is approved for tinnitus (US/Europe) |
| Quality that suggests Meniere's | Fluctuating, variable, roaring or clanging |
| Quality that suggests acoustic neuroma | Constant, high-pitched, unilateral ringing |
Sources: Cummings Otolaryngology Head and Neck Surgery; Goldman-Cecil Medicine 22e; Bailey and Love's Short Practice of Surgery 28e

IMG_1157.jpg
Give me answer for 10 mark
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Kanski's Clinical Ophthalmology. I have all I need to write the full 10-mark answer on Adhimantha vs. modern glaucoma concepts.
COMPARE & CONTRAST: Adhimantha (Ayurvedic) vs. Primary Open Angle Glaucoma & Primary Angle Closure Glaucoma
I. Introduction
Adhimantha is a disease described in classical Ayurvedic texts (Sushruta Samhita and Ashtanga Hridayam) under Netra Rogas (eye diseases). The word literally means "severe churning of the eye" (adhi = great/extreme, mantha = churning). It is considered the most severe and sight-threatening of all the Sarvagata Netra Rogas (diseases of the whole eyeball). In modern medicine, its clinical description closely parallels the spectrum of glaucoma - particularly POAG and PACG.
II. Ayurvedic Concept of Adhimantha
Dosha Involvement
Adhimantha is caused by vitiation of all three doshas, with different presentations depending on the predominant dosha:
| Type of Adhimantha | Predominant Dosha | Modern Correlation |
|---|---|---|
| Vataja Adhimantha | Vata | Chronic open angle glaucoma (POAG) |
| Pittaja Adhimantha | Pitta | Acute inflammatory/congestive glaucoma |
| Kaphaja Adhimantha | Kapha | Chronic angle closure glaucoma |
| Raktaja Adhimantha | Rakta (blood) | Neovascular / hemorrhagic glaucoma |
| Sannipata Adhimantha | All three doshas | Absolute glaucoma |
Pathogenesis (Samprapti) - Ayurvedic View
- Vitiated doshas travel upward via siras (blood vessels/channels) to the head and eyes
- They obstruct the srotas (channels) supplying the eye
- This leads to increased pressure within the eye (Abhishyanda = conjunctival congestion + increased fluid)
- Results in damage to Dristi (the optic disc/visual capacity)
- Progressive destruction of Dristi = blindness
The Ayurvedic concept of obstruction of srotas causing pressure build-up is analogous to impaired aqueous outflow causing raised IOP
Clinical Features (Ayurvedic Description)
- Severe, unbearable pain in the eye (Shirashool, Akshi Shool)
- Redness of the eye
- Watering, photophobia
- Colored halos around lights (Indradhanush darshan = rainbow vision)
- Diminution of vision
- Headache and nausea (in acute types)
- Stony hard eye on palpation
- In chronic types - gradual painless visual loss
Prognosis (Ayurvedic)
Sannipata type (all doshas) - Asadhya (incurable) - corresponds to absolute glaucoma
Vataja type - Yaapya (manageable but not curable)
Treatment (Ayurvedic)
- Snehana (oleation) with medicated oils (Triphala ghrita, Jeevantyadi ghrita)
- Swedana (sudation/fomentation)
- Virechana (therapeutic purgation) - to eliminate vitiated Pitta
- Nasya (nasal instillation of medicated oils) - to relieve Vata in head
- Netra Tarpana (eye bathing with medicated ghee)
- Lekhana (scraping treatment)
- Siravedha (bloodletting from periocular veins) - corresponds to reducing venous congestion
- Systemic Ayurvedic medicines: Triphala, Saptamrita Lauha
III. Modern Concept: Primary Open Angle Glaucoma (POAG)
Definition
POAG is a chronic, progressive optic neuropathy of adult onset characterized by:
- Retinal nerve fibre layer (RNFL) thinning
- Glaucomatous optic nerve damage (cupping)
- Characteristic visual field loss
- Open anterior chamber angle on gonioscopy
- IOP is an important modifiable risk factor (Normal IOP = 10-21 mmHg)
Pathogenesis
Two mechanisms:
- Mechanical - raised IOP deforms the lamina cribrosa, directly damaging retinal nerve fibers as they exit the optic nerve head
- Ischaemic - compression of blood vessels supplying the optic nerve head leads to ischaemic damage
Both lead to: reduced axoplasmic flow → deprivation of neuronal growth factors → retinal ganglion cell apoptosis (programmed cell death) → RNFL loss → cupping → visual field defect
Risk Factors
- Raised IOP (>21 mmHg) - most important modifiable risk factor
- Age (> 40 years)
- Family history (4x risk in siblings)
- Black race (4x more common, earlier onset)
- Myopia
- Diabetes mellitus, systemic vascular disease
Clinical Features
- Asymptomatic until late - the "silent thief of sight"
- No pain, no redness (differentiates from PACG)
- Peripheral visual field loss initially (arcuate scotoma, nasal step)
- Tunnel vision in advanced disease
- IOP may be elevated (but can be normal - Normal Tension Glaucoma)
- Cup-to-Disc (C:D) ratio > 0.5, asymmetry >0.2
Investigations
| Investigation | Finding in POAG |
|---|---|
| Tonometry | IOP usually > 21 mmHg |
| Gonioscopy | Open angle (Grade 3-4) |
| Fundus exam (ophthalmoscopy) | Increased C:D ratio, RNFL defects, disc haemorrhage |
| Perimetry (Humphrey VF) | Arcuate scotoma, nasal step, ring scotoma (advanced) |
| OCT (optic nerve) | RNFL thinning, especially superotemporal and inferotemporal |
Treatment
- Topical IOP-lowering drops (first line):
- Prostaglandin analogues (latanoprost, bimatoprost) - increase uveoscleral outflow
- Beta-blockers (timolol) - decrease aqueous production
- CAIs (dorzolamide), alpha-2 agonists (brimonidine)
- Laser: Selective Laser Trabeculoplasty (SLT) - increases trabecular outflow
- Surgery: Trabeculectomy with Mitomycin C when medical treatment fails
IV. Modern Concept: Primary Angle Closure Glaucoma (PACG)
Definition
PACG is glaucoma due to occlusion of the trabecular meshwork by the peripheral iris (iridotrabecular contact - ITC), obstructing aqueous outflow, associated with glaucomatous optic neuropathy.
PACG may account for up to 50% of all glaucoma globally and is more prevalent in Asians. It progresses rapidly and causes more blindness than POAG.
Mechanism
The primary mechanism is relative pupillary block:
- Aqueous cannot flow freely from posterior to anterior chamber through the pupil
- Pressure builds in the posterior chamber
- Peripheral iris bows forward (iris bombé)
- Iris contacts the trabecular meshwork, blocking aqueous outflow
- IOP rises suddenly and markedly (50-80 mmHg in acute attack)
Risk Factors
- Female sex (more commonly affected)
- Age > 60 years
- Hypermetropia (short, small eye with shallow anterior chamber)
- Short axial length, thick lens
- Asian and Indian ethnicity
- Family history
Clinical Features (Acute Attack - APAC)
| Symptom/Sign | Detail |
|---|---|
| Eye pain | Severe, unbearable |
| Headache, nausea, vomiting | Systemic symptoms common |
| Blurred vision | Corneal oedema; VA 6/60 to hand movements |
| Halos around lights | Corneal epithelial oedema |
| Red eye | Circumcorneal (ciliary) congestion |
| IOP | Very high: 50-80 mmHg |
| Cornea | Steamy/hazy due to oedema |
| Pupil | Mid-dilated, vertically oval, non-reactive |
| Anterior chamber | Shallow |
Chronic PACG
- Insidious, progressive, like POAG
- Angle closes silently with peripheral anterior synechiae (PAS)
- Visual field loss similar to POAG
- Often bilateral
Treatment
| Stage | Treatment |
|---|---|
| Acute APAC | IV/oral acetazolamide 500 mg, topical pilocarpine, IV mannitol; then Nd:YAG laser peripheral iridotomy (LPI) |
| Fellow eye | Prophylactic LPI |
| PAC/PACG | LPI + IOP-lowering drops; if lens present, phacoemulsification deepens AC |
| Refractory | Trabeculectomy with MMC |
V. Comparison Table: Adhimantha vs. POAG vs. PACG
| Feature | Adhimantha (Ayurveda) | POAG (Modern) | PACG (Modern) |
|---|---|---|---|
| Concept | Dosha imbalance obstructing srotas | Progressive optic neuropathy due to raised IOP | Angle occlusion by iris blocking aqueous outflow |
| Onset | Acute (Pittaja) or chronic (Vataja/Kaphaja) | Chronic, insidious | Acute or chronic |
| Pain | Present in acute types | Absent | Present (acute) |
| Eye appearance | Red, congested | White and quiet | Red, congested |
| Vision | Progressive loss | Gradual peripheral loss | Sudden blurring + halos |
| Halos | Mentioned (Indradhanush darshan) | Absent | Present (corneal oedema) |
| IOP | Not measured - described as hard eye | Elevated or normal (NTG) | Very elevated (50-80 mmHg) |
| Angle | Not described | Open | Closed |
| Optic disc | Dristi kshaya (loss of vision faculty) | Cupping, RNFL loss | Cupping after attack |
| Cause | Dosha vitiation, obstruction of srotas | Trabecular dysfunction, raised IOP | Pupillary block, iris-trabecular contact |
| Prognosis | Asadhya if all doshas involved | Controllable if detected early | Reversible if treated urgently |
| Primary treatment | Panchakarma, Nasya, Netra Tarpana | Prostaglandin drops, SLT, trabeculectomy | LPI, pilocarpine, phacoemulsification |
VI. Correlation Summary
| Ayurvedic Type | Modern Equivalent |
|---|---|
| Vataja Adhimantha | POAG / Normal Tension Glaucoma |
| Pittaja Adhimantha | Acute PACG (acute congestive glaucoma) |
| Kaphaja Adhimantha | Chronic PACG |
| Raktaja Adhimantha | Neovascular / hemorrhagic glaucoma |
| Sannipata Adhimantha | Absolute glaucoma |
Key Points to Remember (Exam Focus)
- Adhimantha = glaucoma in Ayurveda; described as severe churning pain with vision loss
- POAG = chronic, painless, open angle - "silent thief of sight"
- PACG = painful, red eye, raised IOP, closed angle - requires emergency treatment
- Both cause optic nerve damage - Ayurveda calls this Dristi kshaya
- Ayurvedic concept of blocked srotas = modern concept of impaired aqueous outflow
- LPI (Laser Peripheral Iridotomy) is the cornerstone of PACG treatment
- Prostaglandin analogues are first-line for POAG
- PACG is more common in Asian women, hypermetropes, short axial length
- POAG is more common in Black populations, myopes, elderly
- Sannipata Adhimantha (all doshas) = Asadhya = corresponds to absolute/end-stage glaucoma
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach 10th Edition; Goldman-Cecil Medicine International Edition
This is a shared conversation. Sign in to Orris to start your own chat.