Marcus gunn pupil
Reading File
Finding Sources
Finding Sources
Searching PubMed
"relative afferent pupillary defect" OR "Marcus Gunn pupil"
Reading File
Reading File
Reading File
Loading Image
Reading File
Excellent - I now have all the content needed for a thorough answer. Here it is:
Marcus Gunn Pupil (Relative Afferent Pupillary Defect / RAPD)
Definition
A Marcus Gunn pupil (also called a relative afferent pupillary defect, RAPD) is a sign of decreased light sensitivity in one eye due to a lesion of the retina or optic nerve on the afferent ("in-going") side of the pupillary light reflex pathway.
Anatomy and Mechanism
The pupillary light reflex has two limbs:
- Afferent: light signal travels from the retina → optic nerve → optic chiasm → pretectal nucleus (midbrain). Fibers cross here to both Edinger-Westphal nuclei.
- Efferent: parasympathetic signal from Edinger-Westphal → CN III → ciliary ganglion → iris sphincter → pupillary constriction in both eyes (direct and consensual responses).
Because crossing occurs at multiple levels (chiasm + pretectum), a unilateral afferent lesion weakens the light signal to the brain from that eye, but the efferent pathway to both eyes remains intact. The result is:
- Reduced direct AND consensual response when light is shone in the affected eye
- Normal response (both pupils constrict briskly) when light is shone in the healthy eye
Key point: Because both pupils still respond together (via the consensual response), an RAPD does not cause resting anisocoria. The pupils appear equal at baseline.
Key point: Lesions at or behind the optic chiasm affect inputs from both eyes and therefore do NOT produce a Marcus Gunn pupil.
The Swinging Flashlight Test
This is the bedside test used to elicit the RAPD:
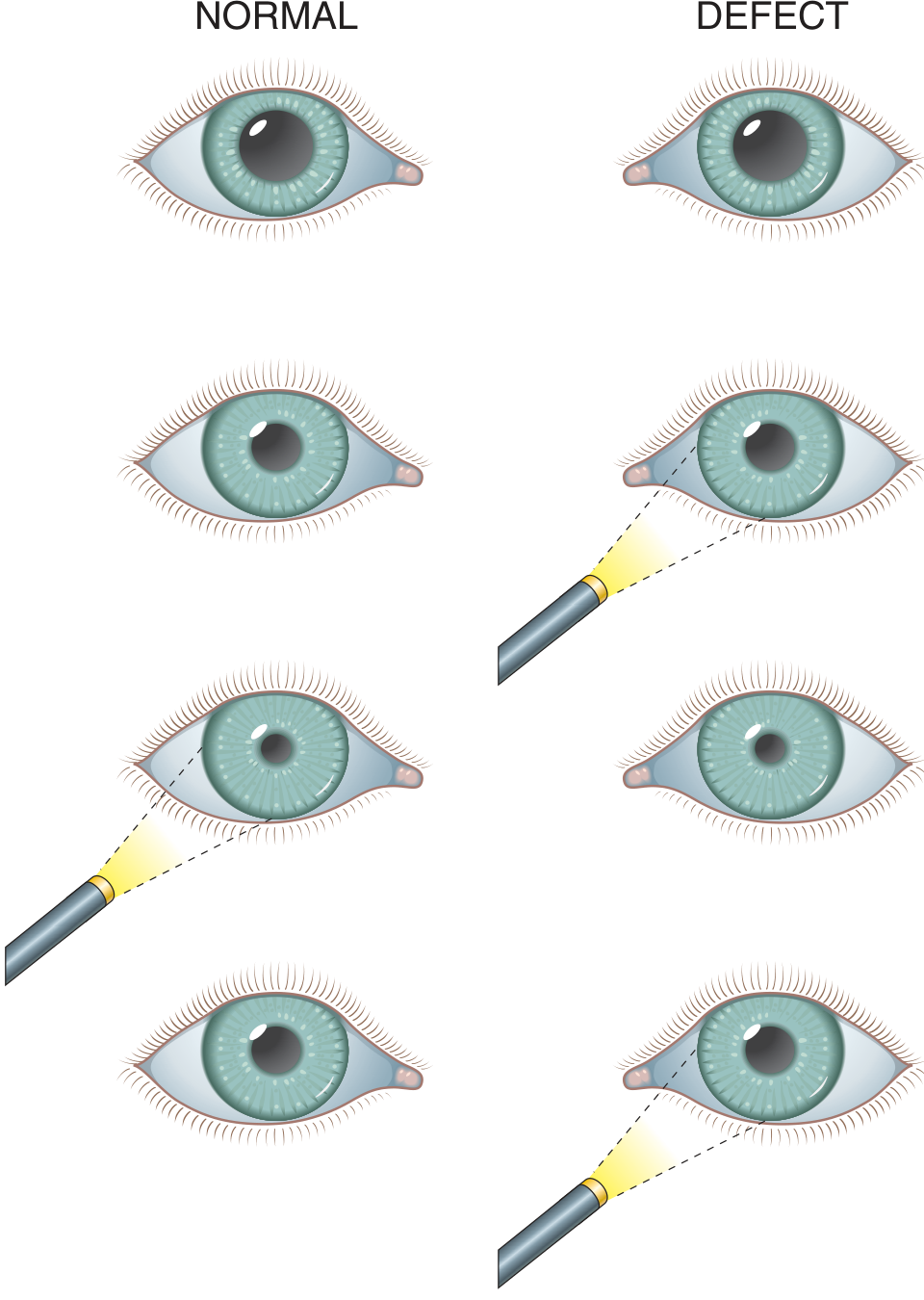
How to perform it:
- Dim the room lights. Ask the patient to fix on a distant target.
- Shine a bright light in one eye for 2-3 seconds; observe direct and consensual constriction.
- Swing the light to the other eye; observe response.
- Repeat back and forth until the pattern is clear.
Positive result (RAPD): When the light swings from the normal eye to the affected eye, the affected pupil dilates (paradoxical dilation) instead of maintaining constriction. This happens because the weaker afferent signal from the affected eye is perceived by the brain as "less light," so both pupils relax slightly.
Distinguish from hippus: Hippus is a normal, brief oscillation of pupil size in response to light and should not be confused with a true RAPD.
Causes
| Category | Examples |
|---|---|
| Optic nerve disease | Optic neuritis (MS-related), ischemic optic neuropathy, optic nerve compression (tumor, retrobulbar hematoma), optic nerve trauma |
| Severe retinal disease | Central retinal artery or vein occlusion, severe retinal detachment |
| Vitreous opacification | Dense vitreous hemorrhage (blocks light from reaching the retina) |
| Orbital pathology | Orbital tumor compressing the optic nerve |
A special note on optic neuritis: the presence of an RAPD combined with eye pain aggravated by movement and blurred vision is strongly indicative of demyelinating disease (e.g., multiple sclerosis). In retrobulbar optic neuritis, the RAPD may be the sole objective finding on examination.
What an RAPD Does NOT Indicate
- It is not caused by lesions posterior to the optic chiasm (visual cortex, optic radiations) - those affect both eyes' input and cancel out
- It does not indicate an efferent (CN III) problem - such a lesion would cause a dilated, unreactive pupil with anisocoria, not an RAPD
- It does not cause a baseline difference in pupil size (no resting anisocoria)
Clinical Significance
- It is an extremely useful objective sign in retrobulbar optic neuritis, where the fundus may look entirely normal and the RAPD is the only positive finding
- In bilateral optic neuropathy, no RAPD will be present if both optic nerves are equally affected (the defects cancel out)
- In orbital trauma, an RAPD indicating retrobulbar hematoma is one of the indications for emergency lateral canthotomy
Sources:
- Neuroanatomy through Clinical Cases, 3rd Ed. (Blumenfeld), p. 609
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025)
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide
This is a shared conversation. Sign in to Orris to start your own chat.