Fever
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"fever of unknown origin" diagnosis management
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile a thorough, well-organized response.
Fever of Unknown Origin (FUO)
Definition
FUO should be distinguished from any febrile illness lacking an obvious initial cause. The classic Petersdorf & Beeson (1961) definition required fever for at least 3 weeks, temperature ≥38.3°C (≥101°F) on at least two occasions, and 1 week of inpatient evaluation without a diagnosis. The modern, widely accepted criteria are:
- Fever ≥38.3°C (≥101°F) on at least two occasions
- Illness duration ≥ 3 weeks
- No known immunocompromised state (immunocompromised patients require a separate, more aggressive approach)
- Diagnosis uncertain despite a minimum standard workup
- Harrison's Principles of Internal Medicine 22E, p. 198
Causes and Epidemiology
FUO etiologies fall into five broad domains. Their relative proportions have shifted over decades as imaging and molecular diagnostics have improved (e.g., fewer intra-abdominal abscesses and cases of infective endocarditis now reach FUO workup because CT and echocardiography catch them earlier).
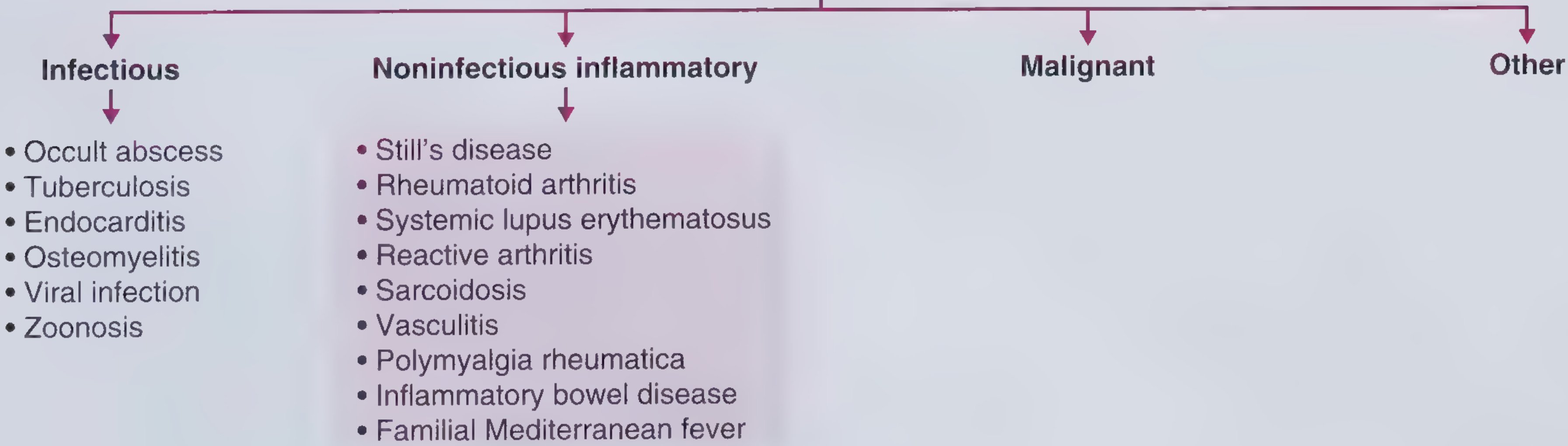
1. Infectious (most common in Asia; ~15-35% in Western Europe)
| Cause | Key Features |
|---|---|
| Intra-abdominal abscess | Most common infectious FUO in industrialized world; liver, spleen, peritoneum; CT abdomen is high-yield early test |
| Tuberculosis | Extrapulmonary or miliary TB most likely to go undetected; check TST/IGRA, cultures, bronchoscopy |
| Culture-negative endocarditis | Due to prior antibiotics, or atypical organisms (Bartonella, Brucella, Coxiella, HACEK, fungi) |
| Osteomyelitis | Vertebral osteomyelitis is the most common site in FUO presentations |
| Viral infections | EBV, CMV, HIV |
| Zoonoses | Cat scratch disease (Bartonella henselae) in young patients with regional lymphadenopathy |
2. Noninfectious Inflammatory (25-30% in Western Europe)
| Disease | Classic Clue |
|---|---|
| Adult-onset Still's disease (AOSD) | Ferritin often >2,000 ng/mL; quotidian fever ≥39°C; salmon-colored evanescent rash; nonsuppurative pharyngitis |
| Rheumatoid arthritis | Symmetric polyarthritis of wrists, MCPs, PIPs |
| SLE | Pancytopenia, low complement; young women |
| Giant cell arteritis (GCA) | Accounts for ~1/5 of FUO in the elderly; headache, jaw claudication, elevated ESR; confirm with temporal artery biopsy |
| Polymyalgia rheumatica | Shoulder/pelvic girdle stiffness; often co-exists with GCA; dramatic glucocorticoid response |
| Sarcoidosis | Bilateral hilar lymphadenopathy |
| IBD | Rare FUO presentation; colonoscopy required |
| Familial Mediterranean Fever (FMF) | Autosomal recessive; Mediterranean ancestry; periodic attacks of fever + serositis; colchicine is treatment of choice |
| Vasculitis / Polyarteritis nodosa | Hepatitis B association, livedo reticularis, testicular pain |
3. Malignancy (~11% in Western Europe)
| Malignancy | Notes |
|---|---|
| Lymphoma | Most common malignant cause of FUO |
| Leukemia | Often with macrocytosis (MDS) |
| Solid tumors | Renal cell carcinoma (hematuria + polycythemia), hepatocellular (cirrhosis), colon (S. gallolyticus endocarditis), breast, lung, pancreatic |
| Atrial myxoma | "Tumor plop" on auscultation |
In patients with known malignancy, infection (not the tumor itself) accounts for most FUO cases.
4. Miscellaneous
Drug fever, pulmonary embolism, subacute thyroiditis (de Quervain's), adrenal insufficiency, IgG4 disease, Kikuchi's disease, hemophagocytic lymphohistiocytosis (HLH), Sweet's syndrome, and many others.
5. No Diagnosis (~40% in Western Europe, ~20% in Asia)
The proportion remaining undiagnosed is 2-5x higher in European vs. Asian cohorts. The large majority of these patients eventually become symptom-free spontaneously, and FUO-related mortality is concentrated in the initial admission.
- Frameworks for Internal Medicine, p. 282-283; Harrison's 22E, p. 198
Diagnostic Approach
General principle: Atypical presentations of common diseases (e.g., extrapulmonary TB) are far more likely than classic presentations of rare diseases.
Tier 1 - History and Physical Exam (guided by clues)
- Travel history, animal exposures, sexual history, medications, family history (FMF)
- Symptoms: morning stiffness, rash, arthralgias, jaw claudication, weight loss, lymphadenopathy
- Medications that cause drug fever: antibiotics, anticonvulsants, allopurinol, antithyroid drugs
Tier 2 - Core Laboratory and Imaging Workup
| Category | Tests |
|---|---|
| Infection | Blood cultures x3, CBC with diff, CRP/ESR, ANA, urine culture, HIV, CMV/EBV serologies, TB (TST or IGRA) |
| Inflammatory | ANA, ANCA, RF, ferritin, complement levels |
| Malignancy | LDH, SPEP, peripheral smear |
| Imaging | CT chest/abdomen/pelvis (high yield early - detects abscesses, lymphadenopathy, masses) |
Tier 3 - Advanced Workup
-
FDG-PET/CT: Can identify a cause in 30-60% of cases when core workup is unrevealing. It can be directly diagnostic (e.g., large-vessel vasculitis) or identify a metabolically active focus for biopsy.
-
Tissue biopsy: Lymph node, liver, bone marrow, or temporal artery - guided by PET/CT findings.
-
Metagenomic next-generation sequencing (mNGS): A 2024 meta-analysis (PMID: 39059148) confirmed increasing utility of mNGS in identifying pathogens missed by conventional workup in FUO.
-
Goldman-Cecil Medicine, p. 2941; Harrison's 22E, p. 198
Management
Empirical therapy is generally discouraged unless the patient is deteriorating, because it can obscure the diagnosis (especially antibiotics and glucocorticoids masking lymphoma or infection).
| Situation | Treatment |
|---|---|
| Hemodynamic instability / neutropenia | Empirical antibiotics justified |
| Positive TST/IGRA or miliary pattern | Empirical anti-TB therapy (after cultures and PCR collected); reassess at 6 weeks if no response |
| Symptomatic relief (persistent undiagnosed FUO) | Acetaminophen or NSAIDs |
| FMF suspected | Colchicine trial (effective prophylactically; response not fully reliable acutely) |
| Still's disease | NSAIDs (can be dramatic); IL-1 inhibitors (anakinra) highly effective |
| GCA / PMR | Glucocorticoids (dramatic response; but glucocorticoids should be withheld until lymphoma/infection adequately excluded) |
| Autoinflammatory syndromes | Anakinra (IL-1Ra) - effective for FMF, CAPS, TRAPS, MKD, Schnitzler's, Still's |
Glucocorticoid caution: They mask fever while allowing spread of infection or lymphoma. Reserve for cases where both have been sufficiently excluded and inflammatory disease is probable and debilitating.
- Harrison's Principles of Internal Medicine 22E, p. 198-199
Key Points Summary
- FUO = fever ≥38.3°C x2, duration ≥3 weeks, no immunocompromise, standard workup unrevealing
- The four main categories: Infections, Noninfectious inflammatory, Malignancy, Miscellaneous (plus Undiagnosed)
- In Western Europe, ~40% remain undiagnosed; most resolve spontaneously
- Start with CT abdomen and core labs; escalate to FDG-PET/CT if unrevealing
- Avoid empirical glucocorticoids or antibiotics unless clearly indicated
- Common diagnoses to always consider: TB, occult abscess, lymphoma, Still's disease, GCA
Fever Everything
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"fever" AND "pathophysiology" AND "management"
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.