Limphoma
Reading File
Finding Sources
Searching PubMed
lymphoma classification diagnosis treatment
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information to provide a thorough overview of lymphoma. Let me compile the full answer.
Lymphoma - A Comprehensive Overview
Lymphoma is a malignant neoplasm of the lymphoid system. It is broadly divided into two major categories: Hodgkin Lymphoma (HL) and Non-Hodgkin Lymphoma (NHL).
1. Definition and Overview
Lymphomas arise from the clonal proliferation of B lymphocytes, T lymphocytes, or NK cells at various stages of differentiation. They primarily involve lymph nodes but can affect extranodal sites (spleen, bone marrow, GI tract, skin, CNS, etc.).
2. Key Differences: HL vs. NHL
| Feature | Hodgkin Lymphoma | Non-Hodgkin Lymphoma |
|---|---|---|
| Spread pattern | Orderly, contiguous spread | Noncontiguous, unpredictable |
| Node involvement | Single axial group (cervical, mediastinal, para-aortic) | Multiple peripheral nodes |
| Extranodal presentation | Rare | Common |
| Mesenteric/Waldeyer ring | Rarely involved | Commonly involved |
| Hallmark cell | Reed-Sternberg cell | Absent |
(Robbins & Cotran Pathologic Basis of Disease, Table 13.7)
3. Hodgkin Lymphoma
Epidemiology
- Accounts for ~0.7% of all new cancers in the US (~9,000 cases/year).
- Bimodal age distribution: one peak in young adults, a second in adults >55 years.
- It was the first human cancer successfully treated with radiation therapy and chemotherapy, and is curable in most cases.
Pathology - Reed-Sternberg (RS) Cells
The defining feature of HL is the Reed-Sternberg cell - a neoplastic giant cell derived from germinal center or post-germinal center B cells. Despite their B-cell origin, RS cells in classic HL fail to express most B-cell-specific genes (including immunoglobulin genes) due to widespread epigenetic changes.
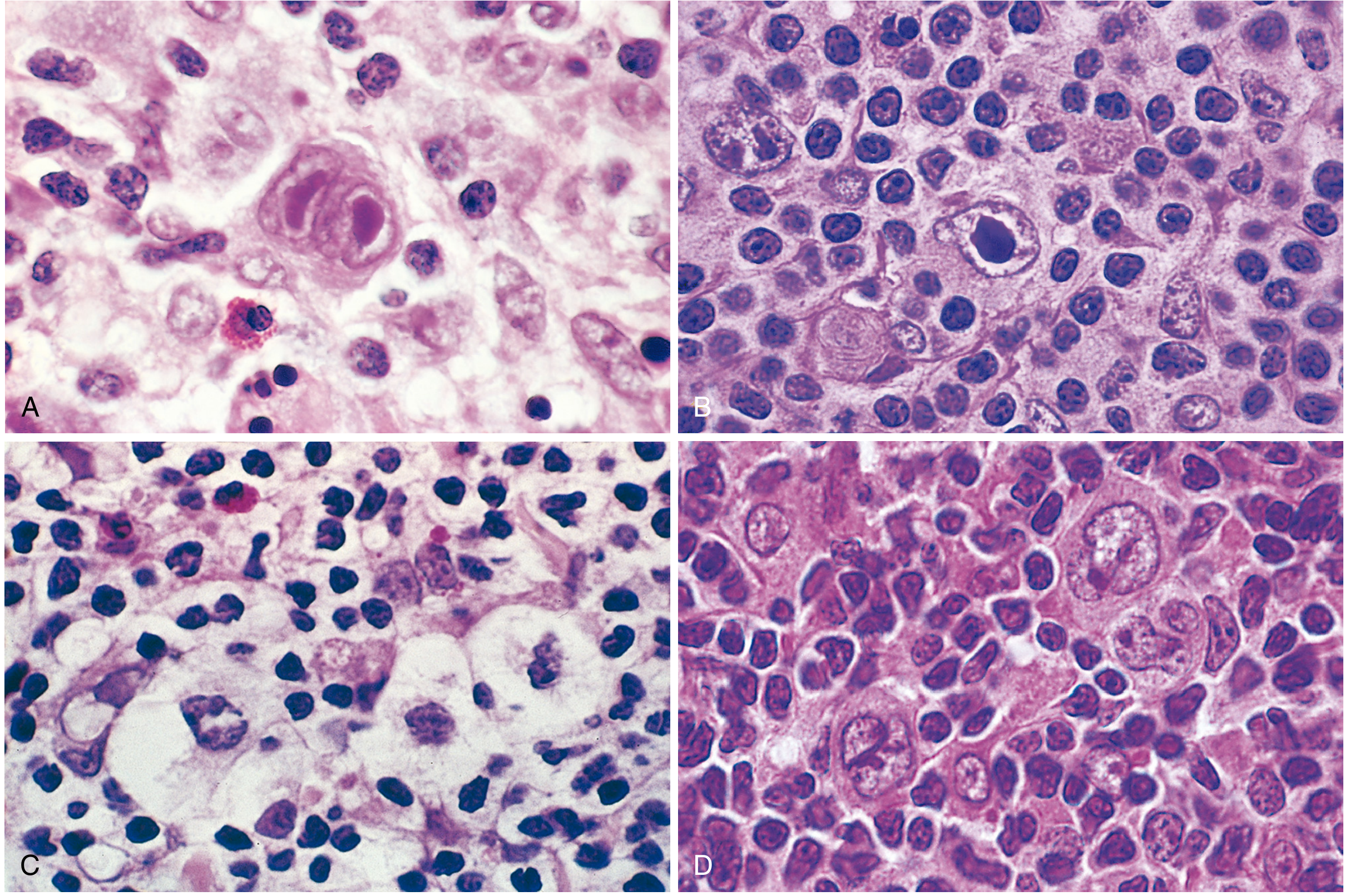
Reed-Sternberg cell variants (Robbins & Cotran)
WHO Classification - 5 Subtypes
| Subtype | Morphology / Immunophenotype | Clinical Features |
|---|---|---|
| Nodular Sclerosis (most common, ~65-70%) | Lacunar RS cells; fibrous collagen bands dividing tissue into nodules; CD15+, CD30+; EBV- | Young adults; frequently stage I/II; mediastinal involvement; equal M:F |
| Mixed Cellularity (~20-25%) | Frequent RS cells + eosinophils, plasma cells; CD15+, CD30+; 70% EBV+ | >50% present as stage III/IV; more common in males; older adults |
| Lymphocyte-Rich (uncommon) | Abundant reactive T lymphocytes; CD15+, CD30+; 40% EBV+ | More common in older males |
| Lymphocyte-Depleted (<5%) | Paucity of lymphocytes, many RS cells; CD15+, CD30+; >90% EBV+ | Older adults, HIV+ individuals, developing countries; advanced stage; worst prognosis of classic HL |
| Nodular Lymphocyte-Predominant | "Popcorn" L&H cells; CD20+, CD15-, CD30-; EBV- | Young males; cervical/axillary nodes; rarely mediastinal |
(Robbins & Cotran Pathologic Basis of Disease, Table 13.8)
Pathogenesis
- NF-κB activation is a central driver of RS cell survival.
- In EBV+ tumors: LMP-1 (Epstein-Barr virus latent membrane protein) transmits survival signals that upregulate NF-κB.
- In EBV- tumors: inactivating mutations in negative regulators of NF-κB (e.g., IκBα) or activating mutations in TNFAIP3 serve the same purpose.
4. Non-Hodgkin Lymphoma (NHL)
Epidemiology
- Much more common than HL.
- 85-90% are B-cell origin in the US and Europe.
Genetics and Pathogenesis
- Most NHL subtypes arise from activation of proto-oncogenes via chromosomal translocations:
| Genetic Abnormality | Associated Lymphoma |
|---|---|
| t(8;14) - MYC overexpression | Burkitt lymphoma |
| t(14;18) - BCL2 overexpression | Follicular lymphoma |
| t(11;14) - Cyclin D1 overexpression | Mantle cell lymphoma |
| MYD88 mutation | Lymphoplasmacytic lymphoma |
WHO 2016 Classification (Key Categories)
Mature B-cell Neoplasms (most common):
- Diffuse Large B-Cell Lymphoma (DLBCL) - ~30% of all NHL; most common subtype worldwide
- Follicular Lymphoma - ~20%; indolent; more frequent in North America and Western Europe
- Extranodal Marginal Zone/MALT Lymphoma - 5-10%
- Small Lymphocytic Lymphoma (SLL/CLL) - 5-10%
- Mantle Cell Lymphoma - 5-10%
- Burkitt Lymphoma - highly aggressive; t(8;14); MYC rearrangement
- Lymphoplasmacytic Lymphoma (Waldenstrom macroglobulinemia) - associated with MYD88 mutation; high IgM causing hyperviscosity
Mature T and NK-cell Neoplasms:
- Mycosis fungoides / Sézary syndrome
- Anaplastic large-cell lymphoma (ALK+ or ALK-)
- Adult T-cell leukemia/lymphoma
- Peripheral T-cell lymphoma, NOS
- Extranodal NK/T-cell lymphoma, nasal type
(Goldman-Cecil Medicine, Table 171-4 - WHO 2016 Classification)
5. Clinical Presentation
Common symptoms include:
- Painless lymphadenopathy (most frequent presenting sign)
- "B symptoms": fever >38°C, drenching night sweats, unexplained weight loss >10% body weight in 6 months
- Fatigue, pruritus (especially HL)
- Mediastinal mass - dyspnea, SVC syndrome
- Splenomegaly, hepatomegaly
6. Diagnosis
- Excision biopsy (preferred over core needle biopsy for adequate tissue for classification)
- Histopathology + immunophenotyping (flow cytometry/IHC) - required for T-cell lymphomas; confirmatory for others
- Cytogenetics/FISH - e.g., t(8;14) confirms Burkitt; t(11;14) + cyclin D1 overexpression confirms mantle cell lymphoma
- An experienced hematopathologist can classify 85%+ of patients by WHO criteria when adequate material is available.
7. Staging - Ann Arbor Classification
| Stage | Description |
|---|---|
| I | Single lymph node region or single extranodal site |
| II | Two or more nodal regions on the same side of the diaphragm |
| III | Nodal regions on both sides of the diaphragm |
| IV | Diffuse or disseminated involvement of extranodal organs (e.g., liver, bone marrow) |
- Each stage is subdivided: A (no B symptoms) or B (presence of B symptoms).
- PET/CT is the preferred imaging modality for initial staging and response assessment.
- Bone marrow biopsy may be omitted in DLBCL if PET/CT shows bone marrow involvement.
Prognostic Indices
- International Prognostic Index (IPI) - 5 adverse factors: age >60, performance status ≤2, elevated LDH, ≥2 extranodal sites, stage III/IV.
- Follicular Lymphoma International Prognostic Index (FLIPI) - tailored for indolent follicular lymphoma.
- Deauville Score (1-5) on PET/CT used to define complete remission after treatment; score ≤3 = complete response.
8. Treatment Principles
Treatment approach depends on:
- Does treatment have curative potential?
- Can treatment prolong survival?
- Will treatment alleviate symptoms?
General approaches:
- Indolent NHL (e.g., follicular lymphoma): May be observed ("watch and wait") if asymptomatic; anti-CD20 monoclonal antibody (rituximab) ± chemotherapy
- Aggressive NHL (e.g., DLBCL): R-CHOP (rituximab + cyclophosphamide, doxorubicin, vincristine, prednisone) is the standard first-line
- HL: ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine) ± radiotherapy; excellent cure rates even in advanced disease
- Targeted therapies: BTK inhibitors (ibrutinib) for mantle cell and lymphoplasmacytic lymphoma; brentuximab vedotin (anti-CD30) for relapsed HL
- Genomic profiling is now typically recommended before starting therapy to guide treatment and inform prognosis.
Summary Table
| Hodgkin Lymphoma | Non-Hodgkin Lymphoma | |
|---|---|---|
| Incidence | Less common | Much more common |
| Hallmark | Reed-Sternberg cell | No specific hallmark cell |
| B-cell origin | Yes (classic HL) | 85-90% B-cell |
| EBV association | Yes (mixed cellularity, lymphocyte-depleted) | Some subtypes (e.g., Burkitt, PTLD) |
| Spread | Contiguous, orderly | Noncontiguous |
| Curability | Most cases curable | Depends on subtype |
| Key treatment | ABVD ± RT | R-CHOP (aggressive); rituximab (indolent) |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Goldman-Cecil Medicine 26th ed.; Murray & Nadel's Respiratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.