Heart failure definition , classification, etiology, clinical Features, diagnosis, treatment .
Reading File
Finding Sources
Finding Sources
Searching PubMed
"heart failure"[MeSH Terms] AND "guidelines"[pt]
Reading File
Reading File
Searching PubMed
"heart failure"[MeSH Terms] AND "guidelines"
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have extensive, authoritative content from multiple top-tier textbooks. Let me compile the comprehensive answer.
Heart Failure: A Comprehensive Overview
1. Definition
Heart failure (HF) is a clinical syndrome resulting from the inability of the heart to meet the metabolic requirements of the body at normal filling pressures. It encompasses a broad range of functional and structural cardiac abnormalities that impair the ability of the ventricle to fill with or eject blood.
Because pulmonary congestion may be absent in many HF patients, the term "heart failure" is preferred over the older term "congestive heart failure."
- Textbook of Family Medicine 9e, p. 566
2. Classification
A. By Ejection Fraction (EF-Based)
| Type | EF | Mechanism |
|---|---|---|
| HFrEF (HF with Reduced EF) | < 40-50% | Reduced LV contraction (systolic dysfunction) |
| HFmrEF (HF with Mildly Reduced EF) | 40-49% | Intermediate, mixed features |
| HFpEF (HF with Preserved EF) | ≥ 50% | Impaired LV filling/relaxation (diastolic dysfunction) |
| HFimpEF (HF with Improved EF) | Previously reduced, now ≥ 40% | Response to therapy |
Important randomized clinical trials to date have enrolled mainly patients with LVEF ≤35-40%, so most evidence-based therapies are proven specifically for HFrEF.
- Fuster and Hurst's The Heart, 15th Edition, p. 1511
B. NYHA Functional Classification (Symptom-Based)
| Class | Description |
|---|---|
| Class I | No limitation of physical activity. Ordinary activity does not cause symptoms. |
| Class II | Slight limitation. Comfortable at rest; ordinary activity causes fatigue, dyspnea, or palpitations. |
| Class III | Marked limitation. Comfortable at rest; less-than-ordinary activity causes symptoms. |
| Class IV | Unable to carry out any physical activity without discomfort; symptoms at rest. |
First introduced in 1928, the NYHA classification remains in widespread use due to its simplicity at the bedside.
C. ACC/AHA Staging (Progression-Based)
| Stage | Description |
|---|---|
| A | High risk for HF; no structural heart disease or symptoms (e.g., hypertension, diabetes, CAD) |
| B | Structural heart disease; no symptoms of HF (e.g., asymptomatic LV dysfunction after MI) |
| C | Structural heart disease WITH prior or current HF symptoms |
| D | Refractory HF requiring specialized interventions (transplant, LVAD, palliation) |
Stages are progressive and not reversible in classification. This system emphasizes prevention at stage A and B.
- Goodman & Gilman's Pharmacological Basis of Therapeutics, p. 670; Fuster and Hurst's The Heart, 15th Edition
D. Hemodynamic Classification (Bedside)
Based on perfusion and volume status:
- Warm & Dry - compensated, normal perfusion, no congestion
- Warm & Wet - congested but adequate perfusion
- Cold & Dry - low output, hypovolemia
- Cold & Wet - low output AND congestion (worst prognosis)
Indicators of congestion: orthopnea, JVD, rales, hepatojugular reflux, ascites, peripheral edema.
Indicators of low perfusion: narrow proportional pulse pressure (<25%), pulsus alternans, cool extremities, impaired mentation.
- Fuster and Hurst's The Heart, 15th Edition, p. 1511
E. By Side of Failure
| Type | Primary mechanism | Consequences |
|---|---|---|
| Left-sided HF | Reduced LV output, elevated left-sided pressures | Pulmonary congestion, pulmonary edema |
| Right-sided HF | Often secondary to left HF or pulmonary hypertension | Systemic venous congestion, peripheral edema, hepatomegaly |
| Biventricular HF | Both ventricles affected | Combined features |
3. Etiology
Common Causes of Left-Sided HF:
- Ischemic heart disease (IHD)/Coronary artery disease - most common cause
- Systemic hypertension - causes pressure overload and LV hypertrophy
- Mitral or aortic valve disease - volume/pressure overload
- Primary myocardial disease - cardiomyopathies (dilated, hypertrophic, restrictive, amyloidosis)
- Diabetes mellitus
- Congenital heart defects
Common Causes of Right-Sided HF:
- Left-sided HF (most common cause of RHF)
- Pulmonary hypertension (primary or secondary)
- Pulmonary embolism
- Chronic obstructive pulmonary disease / cor pulmonale
- Tricuspid or pulmonic valve disease
- Right ventricular MI
Other/Less Common Causes:
- Anemia (high-output HF)
- Thyrotoxicosis (high-output HF)
- Alcoholic cardiomyopathy
- Viral myocarditis
- Peripartum cardiomyopathy
- Toxins (anthracycline chemotherapy, cocaine)
- Infiltrative disease (amyloidosis, sarcoidosis, hemochromatosis)
- Arrhythmias (tachycardia-induced cardiomyopathy)
- Sleep-disordered breathing (obstructive/central sleep apnea)
- Robbins & Kumar Basic Pathology, p. 345; Textbook of Family Medicine 9e, p. 577
4. Pathophysiology
The hemodynamic model of HF has been replaced by the concept of LV remodeling - stretching and dilation with reduction in LV function. Regardless of the initiating injury, neurohormonal mechanisms are activated:
- RAAS activation: Angiotensin II promotes myocyte apoptosis, hypertrophy, and fibrosis. Aldosterone augments these effects and promotes adverse remodeling.
- Sympathetic nervous system (SNS) activation: Elevated catecholamines cause direct myocardial toxicity and downregulate adrenergic receptors.
- Endothelin-1: Produced by dysfunctional endothelium; contributes to vasoconstriction.
- Inflammatory cytokines: Exacerbate endothelial dysfunction.
- MMPs/TIMPs: Lead to cardiac fibrosis and collagen deposition.
- Calcium flux abnormalities and metabolic shifts (glycolysis replacing fatty acid oxidation).
Remodeling is a reversible process with appropriate therapy - this is the basis for using neurohormonal blockers.
5. Clinical Features
Left Heart Failure:
Symptoms (in order of progression):
- Dyspnea on exertion - earliest and most significant symptom
- Orthopnea - dyspnea in the recumbent position (relieved by sitting/standing); patients sleep semi-upright; measured in "number of pillows"
- Paroxysmal nocturnal dyspnea (PND) - dramatic, awakens from sleep with extreme breathlessness
- Cough - due to fluid transudation into airspaces
- Fatigue and exercise intolerance
- Reduced urine output / nocturia
Signs:
- Displaced apex beat (LV enlargement)
- S3 gallop (volume overload, systolic HF)
- S4 gallop (diastolic dysfunction)
- Bilateral basal rales/crackles (pulmonary edema)
- Pleural effusions (more commonly right-sided)
- Tachycardia, narrow pulse pressure
- Cool, clammy extremities (low-output states)
- Pulsus alternans (severe HF)
- Cheyne-Stokes respiration
Right Heart Failure:
Symptoms:
- Lower extremity edema
- Abdominal distension (ascites)
- Vague abdominal pain (hepatic congestion)
- Anorexia, nausea
- Weight gain
Signs:
- Elevated JVP / JVD
- Hepatojugular reflux (HJR)
- Pitting peripheral edema (ankles, sacrum)
- Hepatomegaly (passive congestion), progressing to cardiac cirrhosis, jaundice
- Ascites, anasarca
- Right-sided S3
- Robbins & Kumar Basic Pathology, p. 346-347; Goldman-Cecil Medicine; Frameworks for Internal Medicine
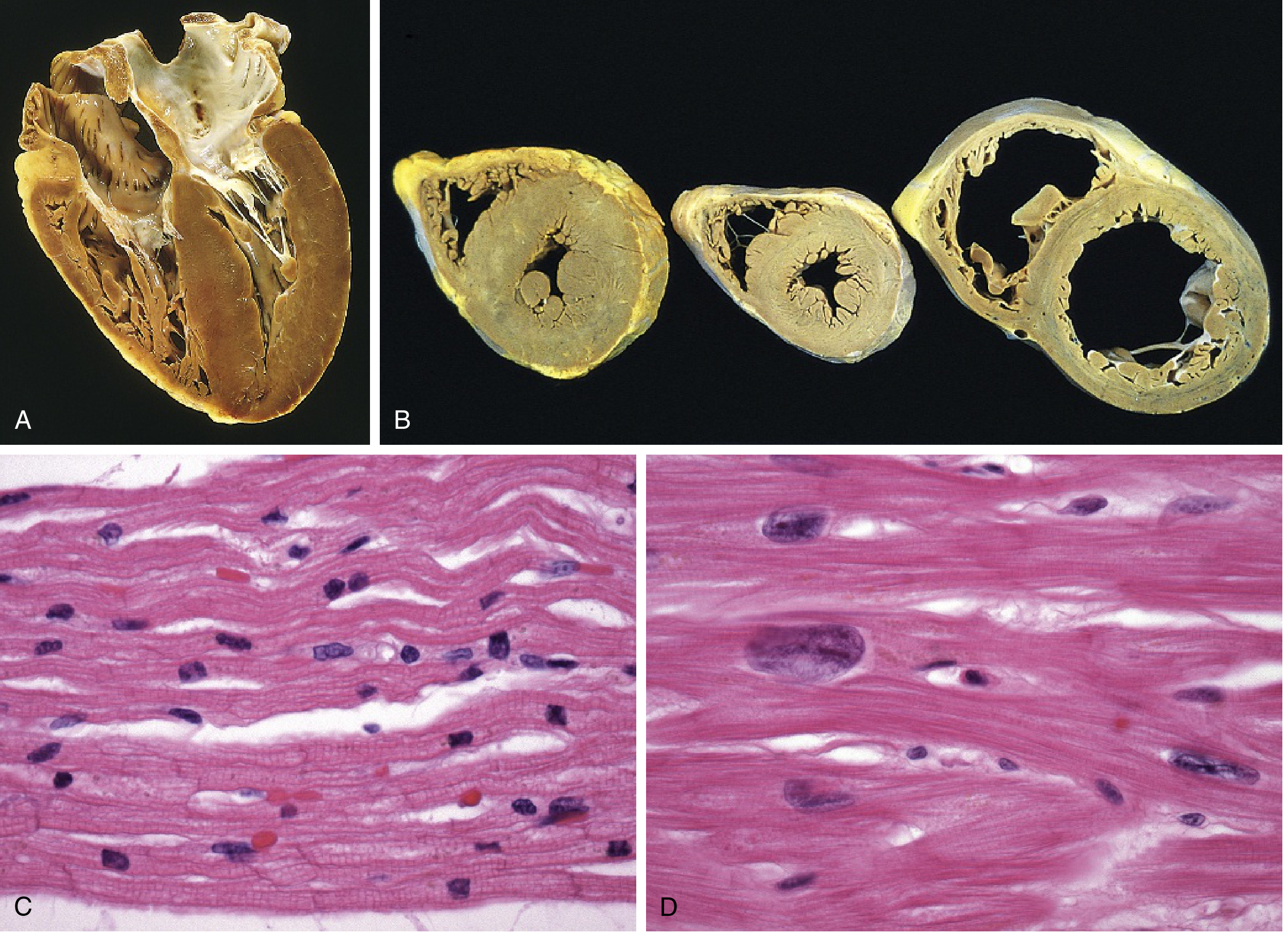
6. Morphological Changes (Pathology)
Heart: LV hypertrophy, often with dilation. LV dilation can cause secondary mitral insufficiency and left atrial enlargement (increasing AF risk). Microscopy shows myocyte hypertrophy with variable interstitial fibrosis.
Lungs: Pulmonary congestion and edema, pleural effusion. Chronic HF produces "heart failure cells" - hemosiderin-laden alveolar macrophages from phagocytosis of extravasated red cells.
7. Diagnosis
Diagnostic Criteria (Framingham Criteria)
Diagnosis requires 2 major or 1 major + 2 minor criteria:
Major criteria:
- PND or orthopnea
- Neck vein distension
- Rales
- Cardiomegaly on chest X-ray
- Acute pulmonary edema
- S3 gallop
- Increased venous pressure (>16 cmH₂O)
- Circulation time >25 sec
- Hepatojugular reflux
Minor criteria:
- Bilateral ankle edema
- Nocturnal cough
- Dyspnea on exertion
- Hepatomegaly
- Pleural effusion
- Decrease in vital capacity by 1/3 from maximal
- Tachycardia (>120 bpm)
Investigations
Laboratory Tests:
| Test | Significance |
|---|---|
| BNP / NT-proBNP | Key biomarker; elevated in HF; used for diagnosis and monitoring. BNP >100 pg/mL or NT-proBNP >300 pg/mL is supportive |
| CBC | Detect anemia (contributing cause) |
| Renal function (BUN/Creatinine) | Baseline; monitor for cardiorenal syndrome |
| Electrolytes | Especially K⁺ (affected by diuretics/RAAS blockers) |
| LFTs | Assess hepatic congestion |
| Thyroid function (TSH) | Rule out thyroid cause |
| Urinalysis | Proteinuria in advanced HF |
| Cardiac enzymes (troponin) | Ischemic etiology |
| HbA1c, lipids | Assess risk factors |
ECG:
- May show: LVH, old MI changes, LBBB, atrial fibrillation, arrhythmias
- Normal ECG makes HF less likely
Chest X-Ray:
- Cardiomegaly (cardiothoracic ratio >0.5)
- Upper lobe blood diversion
- Kerley B lines (interstitial edema)
- Bat-wing pulmonary edema
- Pleural effusions
Echocardiography (most important investigation):
- Gold standard for assessing structure and function
- Determines LVEF (differentiates HFrEF vs HFpEF)
- Assesses wall motion, valvular disease, pericardial disease
- Diastolic function parameters: E/e' ratio >15 indicates high LV filling pressure; e' <8 cm/s (septal) indicates impaired relaxation
- Left atrial volume index >34 mL/m² indicates elevated filling pressures
Key echo parameters:
| Parameter | Abnormal Value | Implication |
|---|---|---|
| LVEF | <50% | Systolic dysfunction |
| LV end-diastolic diameter | ≥60 mm | Volume overload |
| E/e' ratio | >15 | High filling pressure |
| LA volume index | >34 mL/m² | Chronic elevated filling pressures |
| TAPSE | <16 mm | RV dysfunction |
| Tricuspid regurgitation velocity | >3.4 m/s | Pulmonary hypertension |
- Fuster and Hurst's The Heart, 15th Edition, p. 1511
Additional Investigations (when indicated):
- Cardiac MRI - gold standard for myocardial characterization, scar assessment
- Coronary angiography - if ischemic etiology suspected
- Endomyocardial biopsy - for myocarditis, infiltrative diseases
- 6-minute walk test / Cardiopulmonary exercise test - functional assessment
- Holter monitoring - arrhythmia evaluation
8. Treatment
General Principles: ABCDE Approach
- Identify and treat the underlying cause (ischemia, hypertension, valvular disease)
- Identify and treat precipitating factors (infections, arrhythmias, medication non-compliance, excess salt/fluid intake)
- Neurohormonal blockade is the cornerstone of HFrEF therapy
A. Non-Pharmacological Measures (All Stages)
- Salt restriction: <2-3 g sodium/day
- Fluid restriction: ~1.5-2 L/day in severe HF
- Daily weight monitoring (>2 kg gain in 3 days = seek care)
- Regular aerobic exercise (stable patients) - proven to increase exercise capacity
- Smoking cessation, alcohol abstinence
- Vaccination (influenza, pneumococcal)
- Cardiac rehabilitation
B. Pharmacological Treatment
HFrEF (LVEF <40%) - The "Fantastic Four" / GDMT (Guideline-Directed Medical Therapy)
1. ACE Inhibitors (ACEi) - First-line
Reduce mortality and morbidity. Block RAAS; prevent adverse remodeling.
| Drug | Starting dose | Target dose |
|---|---|---|
| Enalapril | 2.5 mg BID | 10-20 mg BID |
| Lisinopril | 2.5-5 mg QD | 20-40 mg QD |
| Ramipril | 2.5 mg BID | 5 mg BID |
| Captopril | 6.25-12.5 mg TID | 50 mg TID |
2. ARBs (for ACEi-intolerant patients, e.g., ACEi cough)
- Candesartan, Valsartan, Losartan
3. ARNI (Angiotensin Receptor-Neprilysin Inhibitor)
- Sacubitril/Valsartan (LCZ696) - superior to ACEi (enalapril) in reducing CV death and HF hospitalization (PARADIGM-HF trial). Replaces ACEi in tolerated patients with HFrEF. Must have a 36-hour washout from ACEi before starting.
4. Beta-Blockers (BB)
Initiated only in clinically stable patients, at very low doses (1/8 target dose), titrated every 4 weeks. Improve LV function over 3-6 months.
| Drug | Starting dose | Target dose | Notes |
|---|---|---|---|
| Carvedilol | 3.125 mg BID | 25 mg BID (50 mg if >85kg) | Non-selective; vasodilation |
| Metoprolol succinate CR/XL | 12.5 mg QD | 200 mg QD | Beta-1 selective; zero-order release required |
| Bisoprolol | 1.25 mg QD | 10 mg QD | Beta-1 selective; long t½ |
- Do NOT start in acutely decompensated HF
- If hospitalized while on BB, reduce dose or hold; restart once stable
5. Mineralocorticoid/Aldosterone Receptor Antagonists (MRA)
- Spironolactone 25-50 mg/day, Eplerenone 25-50 mg/day
- Reduce mortality in NYHA II-IV HFrEF (RALES, EPHESUS trials)
- Monitor K⁺ and renal function closely; contraindicated if K⁺ >5.0 or eGFR <30
6. SGLT2 Inhibitors (the newest pillar)
- Dapagliflozin (DAPA-HF) and Empagliflozin (EMPEROR-Reduced): Reduce CV death and HF hospitalization regardless of diabetes status. Now recommended in all HFrEF patients.
7. Diuretics (for symptom relief/congestion)
- Loop diuretics (furosemide, bumetanide, torsemide) - mainstay for decongestion
- Thiazides (metolazone) - add for diuretic resistance
- Do NOT reduce mortality; improve symptoms and exercise tolerance
8. Ivabradine
- If-channel inhibitor; reduces heart rate in sinus rhythm (HR ≥70 bpm) despite max BB therapy
- Reduces HF hospitalization
9. Hydralazine + Isosorbide Dinitrate
- For patients who cannot tolerate ACEi/ARB/ARNI (e.g., severe renal impairment)
- Proven mortality benefit specifically in Black patients (A-HeFT trial)
10. Digoxin
- Reduces HF hospitalization; no mortality benefit
- Used for rate control in AF or persistent symptoms despite optimal therapy
- Narrow therapeutic index; monitor levels
HFpEF - Limited proven therapies
- SGLT2 inhibitors (empagliflozin - EMPEROR-Preserved; dapagliflozin - DELIVER trial) - recently shown to reduce HF hospitalizations in HFpEF
- Diuretics for congestion relief
- Treat underlying causes: control hypertension, AF rate control, ischemia management
- No proven mortality-reducing pharmacotherapy equivalent to HFrEF exists for HFpEF
C. Device Therapy
1. Implantable Cardioverter-Defibrillator (ICD)
- For primary prevention of sudden cardiac death in HFrEF patients with LVEF ≤35%, NYHA II-III, on optimal medical therapy for ≥3 months, with life expectancy >1 year
2. Cardiac Resynchronization Therapy (CRT)
- For patients with LVEF ≤35%, LBBB with QRS ≥150 ms (≥130 ms in some guidelines), NYHA II-IV on optimal medical therapy
- CRT-D (defibrillator combined): for those also meeting ICD criteria
- Improves LV function, symptoms, and survival; reverses remodeling
3. Left Ventricular Assist Device (LVAD)
- Bridge to transplant or destination therapy for Stage D HF
- Continuous-flow devices are standard
4. Cardiac Transplantation
- Gold standard for end-stage HF (Stage D)
- Indication: refractory HF with poor prognosis, no contraindications
- 1-year survival ~85%; 5-year survival ~70%
D. Treatment of Acute Decompensated HF (ADHF)
Immediate measures:
- Oxygen / NIV (CPAP/BiPAP) for hypoxia/pulmonary edema
- IV loop diuretics (furosemide): rapid decongestion; double the oral dose as IV
- Vasodilators (IV nitroglycerin, nitroprusside): reduce preload/afterload in hypertensive patients
- Inotropes (dobutamine, dopamine): for cardiogenic shock / severely reduced cardiac output
- Intra-aortic balloon pump (IABP): mechanical circulatory support in cardiogenic shock
- Monitor urine output, renal function, electrolytes closely
- Treat precipitating factors (infection, ACS, arrhythmia, hypertensive crisis)
Summary Table: Drugs Proven to Reduce Mortality in HFrEF
| Drug Class | Example | Benefit |
|---|---|---|
| ACEi/ARB/ARNI | Enalapril, Sacubitril-Valsartan | ↓ Mortality ~20-30% |
| Beta-blockers | Carvedilol, Metoprolol succinate, Bisoprolol | ↓ Mortality ~30-35% |
| MRA | Spironolactone, Eplerenone | ↓ Mortality ~15-30% |
| SGLT2 inhibitors | Dapagliflozin, Empagliflozin | ↓ CV death/HF hospitalization |
| Hydralazine/Nitrate | H-ISDN | ↓ Mortality (Black patients) |
Recent Guideline Updates (2025)
The iCARDIO Alliance Global Implementation Guidelines on Heart Failure 2025 (PMID: 40533340) and updated ASE recommendations for HFpEF diagnosis (PMID: 40617625) reinforce the "fantastic four" GDMT for HFrEF (ARNI/ACEi, BB, MRA, SGLT2i) and expand SGLT2i indication to HFpEF.
Sources:
- Textbook of Family Medicine, 9th Edition (Hunt et al.)
- Robbins & Kumar Basic Pathology
- Fuster and Hurst's The Heart, 15th Edition
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
- Braunwald's Heart Disease, 2-Volume Set
- Goldman-Cecil Medicine, International Edition
This is a shared conversation. Sign in to Orris to start your own chat.