Today is my jc presentation and I am 2 nd yr general surgery pg resident ,this is my ppt suggest me questions which can be asked by my professor duringpresentation
Good luck with your presentation today! Here are the likely questions your professor will ask, organized by category:
🔬 Study Design & Methodology
-
Why was a meta-analysis chosen over a narrative review? What are the advantages and limitations of pooling such heterogeneous studies?
-
What is PRISMA? Walk me through the PRISMA flowchart — how many studies were screened, and how many finally included?
-
What is PROSPERO registration, and why is it important? (Answer: prospective registration prevents outcome reporting bias)
-
What statistical model was used, and why? (Answer: random-effects model — because of expected heterogeneity between studies)
-
What does I² mean? How do you interpret I² = 86.1% for bile leak? (Answer: high heterogeneity — >75% is considered substantial)
-
What is a leave-one-out sensitivity analysis? Why was it performed?
-
What is meta-regression? What were the key moderators identified?
-
What tool was used for risk of bias assessment? (Answer: ROBINS-I) What were the main sources of bias in included studies? (Answer: confounding and selective reporting)
-
Why were only observational studies included? Were there any RCTs?
⚕️ Clinical Fundamentals
-
Define the "critical view of safety" (CVS). What are its two criteria? (This is a very high-yield question)
-
What is a subtotal cholecystectomy? What are the two techniques — explain fenestrating vs reconstituting STC in detail.
-
What is the difference between a "difficult gallbladder" and a routine case? Name the classification systems used to grade difficulty. (Nassar, Parkland, AAST, Tokyo Guidelines — know grades for each)
-
What is the Tokyo Guidelines classification of acute cholecystitis? (Grades 1, 2, 3 — mild, moderate, severe)
-
When should you decide intraoperatively to convert to STC? What are your bailout options? (STC, conversion to open, fundus-first, cholecystostomy)
-
What is Mirizzi syndrome? How does it relate to the difficult gallbladder?
📊 Results & Interpretation
-
What was the BDI rate in STC? (0.3%) How does this compare to standard laparoscopic cholecystectomy? (0.3–0.5% for routine LC — STC actually reduces this risk)
-
What was the bile leak rate in STC? (13.5%) What was the risk ratio compared to total cholecystectomy? (RR 6.07 — 6× higher)
-
What were the rates of readmission, reoperation, and ERCP after STC? (17.8%, 6.3%, 16.2%)
-
Was there a difference in mortality between STC and TC? (No — RR 1.52, p = 0.166)
-
Which technique — f-STC or r-STC — had better outcomes? (r-STC: significantly lower bile leak and shorter LOS) Which would you prefer intraoperatively and why?
-
Why was diabetes mellitus a significant risk modifier? What pathophysiology explains worse outcomes in diabetics?
-
Why did conversion to open surgery paradoxically show fewer overall complications? (Early judicious decision allows better operative control)
🧐 Critical Appraisal
-
What are the major limitations of this study? (No standardized definition of "difficult gallbladder," selection bias, no RCTs, limited QoL data, heterogeneity)
-
Why is selection bias particularly problematic here? (STC patients represent more complex anatomy — direct comparison with TC arm is not apples-to-apples)
-
Why could BDI not be directly compared between STC and TC groups statistically? (Model nonconvergence due to extremely low event rates in STC — actually a point in STC's favor)
-
The paper says publication year was paradoxically associated with rising complication rates — how do you explain this? (Better reporting, registries like NSQIP, longer follow-up, more complex cases being captured over time)
🏥 Practical / Scenario-Based
-
You are operating on a patient with Grade 3 acute cholecystitis. You cannot achieve CVS after 30 minutes of dissection. What do you do? (Expect a structured decision-making answer — call for help, consider STC/conversion/cholecystostomy)
-
A diabetic male patient undergoes fenestrating STC. On POD 3 he has bile in the drain. How do you manage this? (Conservative first; if persistent → ERCP with stenting)
-
A patient comes back 6 months after STC with right upper quadrant pain and jaundice. What do you suspect and how do you manage? (Retained stones — ERCP ± completion cholecystectomy; MRCP first)
-
What is the role of percutaneous cholecystostomy vs EUS-guided gallbladder drainage in patients unfit for surgery? (EUS-GBD with LAMS has Level I evidence over PCT from RCTs — DRAC 1 trial)
💡 Tips for Your Defense
- For every complication (bile leak, retained stones), know the management algorithm
- Be ready to draw the Calot's triangle and explain CVS
- Know the SSAT, WSES, and AAST guidelines on STC as endorsed bailout
- Frame STC as: "trading the catastrophic risk of BDI for a more manageable but significant set of postoperative morbidities" — this is the paper's central thesis
All the best for your JC today! 🎯
Answer above questions so that I can answer them all and use diagrams as well
Reading File
Finding Sources
Finding Sources
Searching Images
critical view of safety laparoscopic cholecystectomy Calot's triangle
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching Images
subtotal cholecystectomy fenestrating reconstituting technique diagram
Reading File
Reading File
Reading File
Searching Images
Mirizzi syndrome bile duct compression gallstone anatomy diagram
Reading File
Finding Sources
Finding Sources
Searching Images
Tokyo Guidelines severity grading acute cholecystitis table
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Here is your complete JC defence guide with answers and images for every question:
📖 Journal Club Defence Guide
Subtotal Cholecystectomy — Complete Q&A with Diagrams
🔬 SECTION A: Study Design & Methodology
Q1. Why was a meta-analysis chosen? What are its advantages and limitations?
Answer:
A meta-analysis was chosen because multiple individual studies on STC exist but each had small sample sizes and varying outcomes. Pooling them increases statistical power to detect differences in rare events (like BDI, which occurs in <1% of cases). A meta-analysis also generates overall effect estimates with confidence intervals.
Advantages:
- Increases sample size → greater power
- Reduces random error
- Can identify consistency or heterogeneity across studies
- Generates quantitative summary estimates (Risk Ratios, pooled rates)
Limitations:
- Garbage in = garbage out (quality depends on included studies)
- Cannot overcome selection bias in original observational studies
- High heterogeneity (I² = 86.1% for bile leak) limits direct pooling
- No RCTs available — all observational data
Q2. What is PRISMA and what does the flowchart show?
Answer:
PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses. It is a 27-item checklist + flow diagram ensuring transparent, complete reporting of systematic reviews.
The PRISMA flowchart has 4 stages:
- Identification — Records identified through database search
- Screening — Titles/abstracts screened; duplicates removed
- Eligibility — Full-text articles assessed for inclusion criteria
- Included — Final studies included in quantitative synthesis
When asked, walk through each stage using the actual numbers from your paper's flowchart.
Q3. What is PROSPERO registration and why is it important?
Answer:
PROSPERO is an international register for systematic review protocols (prospective registration before data collection begins).
Importance:
- Prevents outcome reporting bias — researchers can't selectively report only favourable outcomes after seeing the data
- Increases transparency and reproducibility
- Registration number is publicly verifiable
- Required by many journals for systematic review submission
Q4. What statistical model was used and why?
Answer:
A random-effects model (DerSimonian-Laird method) was used.
Why random-effects vs fixed-effects?
| Feature | Fixed-Effects | Random-Effects |
|---|---|---|
| Assumption | All studies estimate same true effect | Each study has its own true effect |
| When to use | Low heterogeneity (I²<25%) | High heterogeneity (I²>50%) |
| Effect of outliers | Heavily influenced | Less influenced |
Since STC studies differ in patient population, technique (f-STC vs r-STC), time period, and case complexity — heterogeneity is expected → random-effects is the correct choice.
Q5. What does I² mean? How do you interpret I² = 86.1% for bile leak?
Answer:
I² quantifies the proportion of total variation between studies due to heterogeneity (not chance).
| I² Value | Interpretation |
|---|---|
| 0–25% | Low heterogeneity |
| 25–50% | Moderate |
| 50–75% | Substantial |
| >75% | Considerable/High |
I² = 86.1% for bile leak = considerable heterogeneity. This means 86.1% of the variability in bile leak rates across studies is due to true differences between studies (different populations, operative technique, follow-up duration, reporting standards), not sampling error. This is why the pooled estimate must be interpreted cautiously, and why subgroup and meta-regression analyses were performed to explore sources.
Q6. What is leave-one-out sensitivity analysis?
Answer:
A sensitivity analysis where you remove one study at a time and recalculate the pooled result to see if any single study is driving the overall finding.
Purpose:
- Tests robustness of the pooled estimate
- If the result changes dramatically when one study is removed, that study has disproportionate influence
- If the result is stable across all iterations → the finding is robust
In this paper, it was used to check whether any single center's outlier outcomes were distorting the overall BDI or bile leak rates.
Q7. What is meta-regression?
Answer:
Meta-regression is a statistical technique that examines whether study-level covariates (moderators) explain heterogeneity between studies.
It is analogous to regular regression, but the unit of analysis is the study, not the individual patient.
Key moderators identified in this paper:
- Publication year — paradoxically associated with rising complication rates (better reporting over time)
- Diabetes mellitus — significant predictor of worse postoperative outcomes
- Conversion to open surgery — associated with paradoxically fewer overall complications (early judicious decision → better operative control)
- Type of STC (f-STC vs r-STC) — r-STC had significantly better outcomes
Q8. What tool was used for risk of bias assessment? What were the main sources of bias?
Answer:
ROBINS-I (Risk Of Bias In Non-randomised Studies – of Interventions) was used.
It assesses 7 domains:
- Confounding
- Selection of participants
- Classification of interventions
- Deviations from intended interventions
- Missing data
- Measurement of outcomes
- Selection of reported results
Main biases in this paper:
- Confounding: STC patients inherently have more complex anatomy than TC patients — direct comparison is not like-for-like
- Selective reporting: Older studies may under-report complications
- Selection bias: STC chosen for the most difficult cases, inflating complication rates compared to TC group
Q9. Why were only observational studies included? Were there any RCTs?
Answer:
No RCTs exist comparing STC to total cholecystectomy — and ethically, this is difficult. You cannot randomise a patient intraoperatively to STC vs TC; the decision is made in real-time based on what the surgeon encounters (bleeding, anatomy, inflammation). An RCT would require prospective randomisation at the time of port placement before seeing the anatomy, making it logistically and ethically challenging.
Therefore, the best available evidence comes from observational cohort studies and case series, which is why only these were included.
⚕️ SECTION B: Clinical Fundamentals
Q10. Define the Critical View of Safety (CVS). What are its TWO criteria?
Answer (Strasberg & Soper, 1990s):
CVS is the gold standard intraoperative safety technique before any clipping or division during laparoscopic cholecystectomy.
The THREE criteria for CVS (often stated as "two structures + clear plate"):
- The hepatocystic triangle is cleared of all fibrofatty tissue — only the cystic duct and cystic artery remain
- The lower one-third of the gallbladder is separated from the cystic plate (liver bed) — confirming the gallbladder is partially detached
- Two (and only two) structures are seen entering the gallbladder — cystic duct and cystic artery
The "two criteria" formulation commonly tested: (1) clear hepatocystic triangle, (2) only two structures into GB.
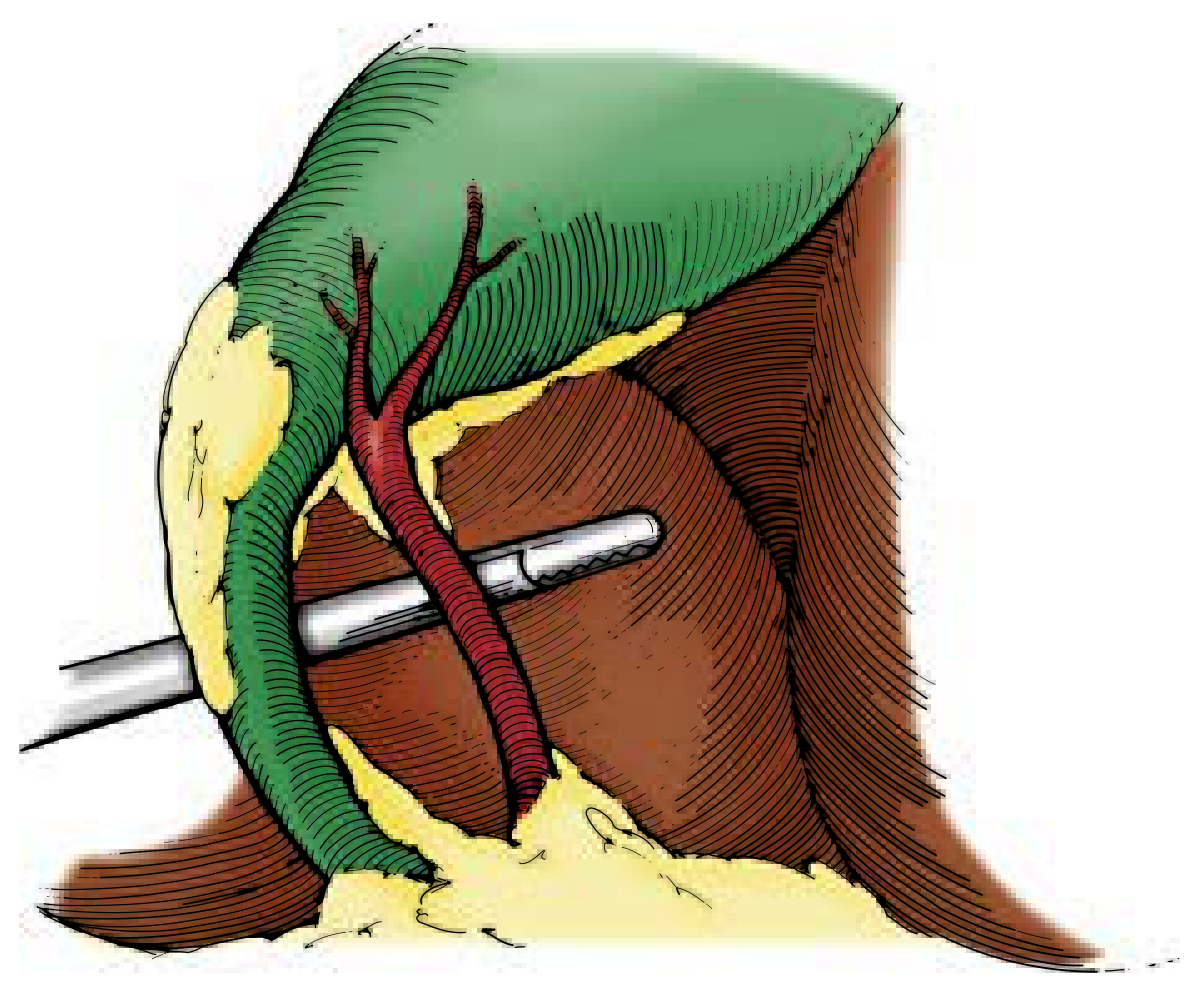
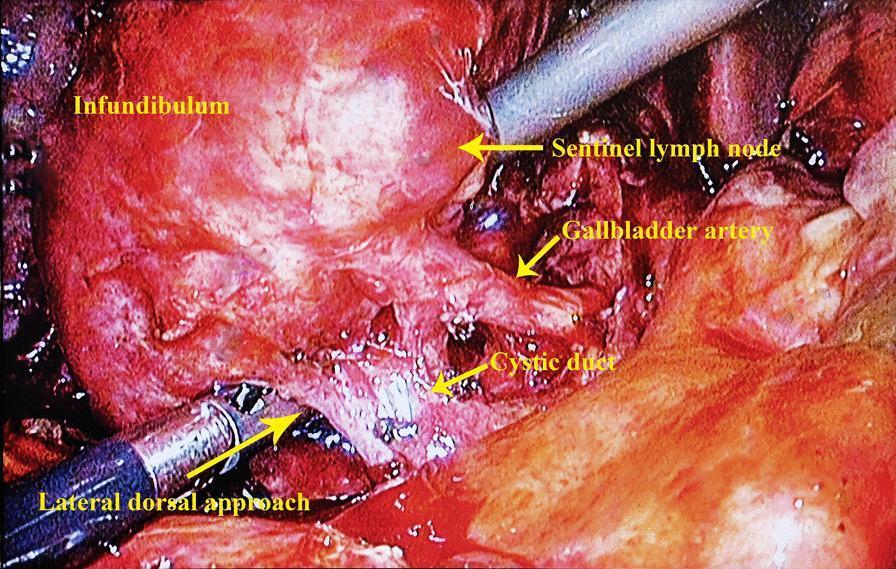
Key point: Dissection should begin on the infundibulum of the gallbladder, NOT on the triangle of Calot itself — to avoid inadvertently starting on the medial side of the CBD and misidentifying it as the cystic duct.
— Current Surgical Therapy 14e; Mulholland & Greenfield Surgery 7e
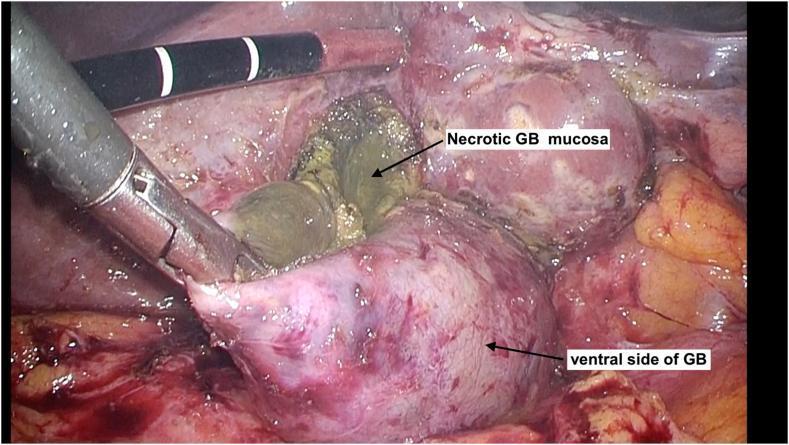
Q11. What is subtotal cholecystectomy? Explain fenestrating vs reconstituting STC in detail.
Answer:
STC is a bailout procedure used when standard total cholecystectomy cannot be safely completed — the gallbladder is opened above the neck, stones are removed, and the neck/infundibulum is left in situ to protect the CBD.
Two techniques:
| Feature | Fenestrating STC (f-STC) | Reconstituting STC (r-STC) |
|---|---|---|
| What is done | GB opened, ventral wall removed, posterior wall may be left on liver bed; neck left open — cystic duct closed with purse-string suture | GB opened, stones removed; neck and infundibulum closed with suture or stapler |
| Bile leak risk | Higher (open cystic duct stump → biliary fistula) | Lower |
| Stone recurrence | Lower (cystic duct closed) | Higher (residual GB remnant → stone formation) |
| Reintervention | ~32% overall | ~26% overall |
| Completion cholecystectomy needed | ~9% | ~4% |
| This paper's finding | Worse outcomes (higher bile leak, longer LOS) | Better outcomes |
Post-STC management: Always place a closed-suction drain in the gallbladder fossa — bile leaks usually resolve spontaneously with drainage.
— Mulholland & Greenfield Surgery 7e, p. 3067
Q12. What is a "difficult gallbladder"? Name the grading systems.
Answer:
A difficult gallbladder is one where standard dissection and achievement of CVS is impaired due to anatomical, pathological, or patient factors.
Causes:
- Acute/chronic inflammation, fibrosis
- Cirrhosis / portal hypertension
- Mirizzi syndrome
- Previous upper abdominal surgery
- Morbid obesity
- Impacted stone at Hartmann's pouch/cystic duct
Classification systems:
| System | Key Features |
|---|---|
| Nassar Scale (1–4) | Grade 1: easy; Grade 4: requires conversion/STC |
| Parkland Scale (1–5) | Based on degree of adhesions and inflammation at Calot's triangle |
| AAST EGS Scale (1–5) | American Association for Surgery of Trauma — based on anatomical distortion, ischaemia, perforation |
| Tokyo Guidelines | Grade I (mild), II (moderate), III (severe) — based on organ dysfunction |
Q13. Tokyo Guidelines — Acute Cholecystitis Grades
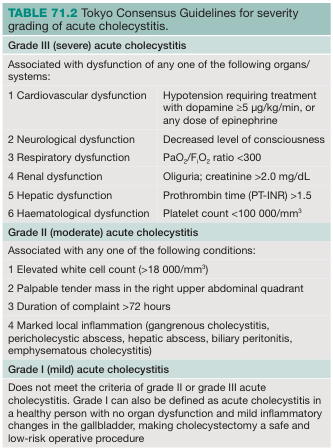
Summary:
Grade I (Mild): Healthy patient, no organ dysfunction, mild GB changes → Early lap-C safe (CCI ≤5, ASA ≤2)
Grade II (Moderate): ANY of:
- WBC >18,000/mm³
- Palpable RUQ tender mass
- Symptoms >72 hours
- Marked local inflammation (gangrenous cholecystitis, pericholecystic abscess, biliary peritonitis, emphysematous cholecystitis) → Early lap-C by experienced surgeon if CCI ≤5, ASA ≤2; otherwise GB drainage then delayed lap-C
Grade III (Severe): Organ dysfunction in ANY of:
- Cardiovascular: hypotension requiring vasopressors
- Neurological: decreased consciousness
- Respiratory: PaO₂/FiO₂ <300
- Renal: oliguria or creatinine >2 mg/dL
- Hepatic: PT-INR >1.5
- Haematological: platelets <100,000/mm³ → Urgent GB drainage; surgery only after organ support in experienced centres
— Mulholland & Greenfield Surgery 7e; Bailey & Love 28th Ed.
Q14. When should you decide to convert to STC intraoperatively?
Answer:
The decision is based on the "Time-out" rule and the SSAT/WSES safe-cholecystectomy framework.
Indications to abandon CVS and proceed to STC:
- Cannot clearly identify the two structures entering the GB after reasonable dissection
- Dense fibrosis obliterating Hartmann's pouch/cystic duct junction
- Grade II/III acute cholecystitis with frozen Calot's triangle
- Bleeding obscuring the field
- Impacted stone at infundibulum preventing identification of cystic duct
Bailout hierarchy (CULTURE of safety):
- Call for help / experienced colleague
- Attempt CVS again from a different approach (fundus-first/dome-down)
- Subtotal cholecystectomy (f-STC or r-STC depending on anatomy)
- Conversion to open cholecystectomy (note: less safe if surgeon not trained in open technique)
- Cholecystostomy tube if patient too unstable for extended procedure
Q15. What is Mirizzi Syndrome?
Answer:
Mirizzi syndrome is external compression of the common hepatic duct (CHD) or common bile duct (CBD) by a stone impacted in the cystic duct or Hartmann's pouch, causing obstructive jaundice.
Types:
| Type | Description |
|---|---|
| Type I | Extrinsic compression of CHD/CBD by impacted stone in cystic duct — NO fistula |
| Type II | Cholecystobiliary fistula involving <1/3 circumference of CBD |
| Type III | Fistula involving 1/3 to 2/3 circumference of CBD |
| Type IV | Fistula involving complete destruction of CBD wall |
Incidence: ~1% of all patients undergoing cholecystectomy
Presentation: Repeated bouts of pain, fever, jaundice; elevated bilirubin; intrahepatic ductal dilatation on USS
Why it causes a difficult cholecystectomy: The impacted stone distorts and inflames the hepatocystic triangle — the GB appears fused to the CBD, making CVS impossible and drastically raising BDI risk
Management:
- Type I: Cholecystectomy (open preferred; lap by experienced surgeon)
- Type II–IV: Often require biliary reconstruction (hepaticojejunostomy) after stone clearance
— Mulholland & Greenfield Surgery 7e; Sleisenger & Fordtran GI & Liver Disease
📊 SECTION C: Results & Interpretation
Q16. BDI rate in STC vs standard LC?
Answer:
- STC BDI rate: 0.3% — this is equal to or lower than standard laparoscopic cholecystectomy (0.3–0.6%)
- This is the paper's most powerful finding — STC, performed in the most difficult gallbladders, achieves the SAME BDI rate as routine lap-C
- Direct statistical comparison was not possible (model nonconvergence due to extremely low event rates) — but descriptively, STC is highly protective against BDI when CVS cannot be achieved
Key message: "STC trades the catastrophic risk of BDI for a more manageable set of postoperative morbidities."
Q17. Bile leak rate in STC?
Answer:
- Overall bile leak rate: 13.5% in STC
- Risk Ratio vs Total Cholecystectomy: RR = 6.07 (6× higher risk of bile leak with STC)
- Most leaks resolve with conservative management (drain in situ)
- High I² (86.1%) for this outcome — significant heterogeneity between studies
Mechanism: The cystic duct stump (fenestrating) or the closed infundibulum (reconstituting) can leak bile postoperatively. This is WHY a drain is mandatory after STC.
Q18. Readmission, reoperation, ERCP rates after STC?
| Outcome | Rate |
|---|---|
| Readmission | 17.8% |
| Reoperation | 6.3% |
| ERCP requirement | 16.2% |
ERCP is needed for retained stones migrating into the CBD or persistent bile leak not resolving with drainage alone. The 16.2% ERCP rate reflects the significant retained stone burden in patients undergoing STC (stones may be left behind in the cystic duct remnant or migrate).
Q19. Was there a difference in mortality between STC and TC?
Answer:
- No statistically significant difference in mortality: RR 1.52, p = 0.166
- This means STC does NOT increase mortality compared to total cholecystectomy
- Combined with the equivalent BDI rate, this supports STC as a safe bailout procedure
- The non-significant finding despite numerically higher RR is likely due to the low absolute mortality rates and insufficient power to detect a small difference
Q20. Which technique — f-STC or r-STC — had better outcomes? Which would you choose?
Answer:
r-STC (reconstituting) had significantly better outcomes:
- Lower bile leak rate
- Shorter length of stay
- Lower need for ERCP
Choice in practice:
- r-STC is preferred when the infundibulum can be safely closed (closed stump prevents biliary fistula)
- f-STC is chosen when the infundibulum is too necrotic, inflamed, or adherent to safely suture — leaving it open with a drain is safer than a failed closure
- The operative decision must be individualised based on the anatomy found
Q21. Why was diabetes mellitus a significant risk modifier?
Answer:
In meta-regression, DM was a significant predictor of worse outcomes after STC.
Pathophysiological explanation:
- Impaired wound healing — poor collagen synthesis, reduced angiogenesis
- Microvascular disease — ischaemia of the GB wall makes necrosis and gangrene more likely; tissue doesn't heal after STC
- Immune dysfunction — neutrophil dysfunction, impaired phagocytosis → higher infection rates, delayed resolution of bile leaks
- Neuropathy — blunted pain response → delayed presentation → more severe cholecystitis at time of surgery
- Susceptibility to Clostridium → emphysematous cholecystitis more common in diabetics
Clinical implication: In diabetic patients undergoing STC, have a lower threshold for prolonged drainage and closer follow-up.
Q22. Why did conversion to open surgery paradoxically show fewer overall complications?
Answer:
This is a nuanced finding. In the meta-regression, conversion to open cholecystectomy was associated with fewer overall complications.
Explanation:
- Selection effect — surgeons who converted early (before injuring the CBD) showed good surgical judgment; the operation was completed safely
- Open approach allows better exposure in a difficult/frozen hepatocystic triangle — finger dissection, better tactile feedback, control of bleeding
- Early judicious conversion (before catastrophic injury) produces better outcomes than persisting laparoscopically until complications force the surgeon's hand
- Reporting bias — studies with high conversion rates may be from specialized HPB centres with better outcomes overall
The lesson: Conversion is not failure — it is sound surgical decision-making.
🧐 SECTION D: Critical Appraisal
Q23. What are the major limitations of this study?
Answer (structured for maximum marks):
- No standardised definition of "difficult gallbladder" — each study had different inclusion criteria for when STC was performed; heterogeneous patient populations
- Selection bias — STC patients represent the most complex anatomy; comparing outcomes to TC is comparing apples to oranges
- No RCTs — all observational studies; inherent confounding cannot be fully adjusted
- High heterogeneity (I² = 86.1% for bile leak) — limits reliability of pooled estimates
- Limited quality of life (QoL) data — long-term patient-reported outcomes not systematically captured
- Variable follow-up duration — some complications (retained stones, strictures) may present late; shorter follow-up studies will undercount
- Publication bias — centres with poor outcomes may not publish; likely underestimates true complication rates
- Lack of operative detail standardisation — technique variations in suturing, drain placement, and stone clearance across centres
Q24. Why is selection bias particularly problematic here?
Answer:
STC is performed precisely because the surgery is the most dangerous — Calot's triangle is frozen, the anatomy is distorted, CVS cannot be achieved. These are inherently the hardest cases with the highest baseline risk.
When you compare STC outcomes to TC outcomes, the TC group includes routine cholecystectomies for simple symptomatic cholelithiasis. The two groups are not comparable without adjustment for operative difficulty score, degree of inflammation, and comorbidities.
This selection bias artificially inflates the complication rates attributed to STC — making the 13.5% bile leak rate look worse than it really is when put in context. The correct comparison would be: "What would the BDI rate have been if these same patients had undergone TC?" — and that counterfactual is unknowable.
Q25. Why could BDI not be directly compared statistically between STC and TC?
Answer:
Model nonconvergence due to extremely low event rates in the STC group (BDI = 0.3%).
When event rates approach zero, the statistical models (particularly log-odds or log-risk models used in meta-analysis) become numerically unstable — the variance estimates become infinite, and the model cannot converge.
Paradoxically, this supports STC — the BDI rate in STC is so low that the statistical model cannot distinguish it from zero. This is the desired outcome: STC is being performed to prevent BDI, and it appears to be achieving that goal with remarkable success.
Q26. Publication year paradoxically associated with rising complication rates — explain.
Answer:
This is a classic surveillance bias / reporting quality effect:
- Better reporting over time — modern studies use standardised outcome definitions (Clavien-Dindo, ISGLS leak criteria) and report complications more systematically than older case series
- Administrative databases (NSQIP, ACS) — capture outcomes prospectively across all cases, including complications that might have been omitted in single-centre retrospective series from the 1990s–2000s
- Longer follow-up — more recent studies often include 90-day or 1-year outcomes, capturing late complications (retained stones, strictures) that older studies with 30-day follow-up missed
- Expanded indications — as STC gained acceptance, it started being applied to increasingly complex patients (cirrhosis, portal hypertension, prior surgery), raising the complication denominator
🏥 SECTION E: Scenario-Based / Practical
Q27. You are operating on Grade III acute cholecystitis. You cannot achieve CVS after 30 minutes. What do you do?
Structured answer:
Step 1 — Recognise and STOP. Do not persist blindly with dissection.
Step 2 — Call for help. Inform the anaesthetist; request a senior/HPB colleague if available.
Step 3 — Reassess anatomy:
- Try fundus-first/dome-down approach
- Try posterior/lateral approach from the right side of Calot's triangle
Step 4 — Decide on bailout:
- If anatomy still unclear → Subtotal cholecystectomy
- If infundibulum closeable → r-STC
- If gangrenous/necrotic neck → f-STC with purse-string drain
- If patient haemodynamically unstable → Cholecystostomy tube (percutaneous) and return at 6 weeks
- If intraoperative uncertainty about CBD injury → Intraoperative cholangiogram (IOC)
Step 5 — Post-procedure:
- Place a closed-suction drain in the GB fossa
- Ensure stone clearance
- Arrange MRCP at 4–6 weeks to assess CBD, identify retained stones
- Plan for completion cholecystectomy if GB remnant symptomatic
Q28. Diabetic patient undergoes f-STC. POD 3 — bile in the drain. How do you manage?
Structured answer:
Assess severity first:
- Volume of drainage: low (<200 mL/day) vs high output
- Clinical status: fever, RUQ pain, jaundice → suggests obstructed system
- Drain bilirubin ÷ serum bilirubin ratio — if >3:1 confirms bile leak
ISGLS Grading of Bile Leak:
- Grade A: Drain in situ, no change in management required
- Grade B: Requires active intervention (ERCP/radiology) but no reoperation
- Grade C: Requires reoperation
Management algorithm:
- Keep drain in situ — most low-output leaks resolve within 2 weeks
- MRCP — to assess CBD anatomy, confirm no BDI, identify retained stones
- If persistent or increasing → ERCP + biliary stenting (reduces transpapillary pressure, diverts bile away from the stump leak)
- If bile collection (biloma) develops → CT-guided percutaneous drainage
- If biliary peritonitis or Grade C leak → Surgical washout + drain placement ± completion cholecystectomy
In this diabetic patient: Have a lower threshold to escalate — impaired healing increases risk of Grade B/C evolution.
Q29. Patient returns 6 months after STC with RUQ pain and jaundice. What do you suspect?
Answer:
Differential diagnosis:
- Retained/recurrent common bile duct stones (most likely — 16.2% ERCP rate post-STC)
- GB remnant with stone formation (r-STC → residual mucosa continues to produce stones)
- Biliary stricture (cystic duct stump/CBD stricture from inflammation)
- Cholangitis (stones obstructing CBD → Charcot's triad)
Investigation:
- LFTs, GGT, Bilirubin — obstructive pattern (raised ALP, GGT, direct bilirubin)
- Abdominal USS — CBD dilatation, any visible stones
- MRCP (non-invasive gold standard for CBD stones) — visualise whole biliary tree
- CT abdomen — if abscess / collection suspected
Management:
- If CBD stones confirmed on MRCP → ERCP + sphincterotomy + stone extraction + biliary stent
- If GB remnant with stones → Completion cholecystectomy (laparoscopic or open)
- If biliary stricture → ERCP stenting ± surgical reconstruction (hepaticojejunostomy if tight stricture)
Q30. Role of Percutaneous Cholecystostomy vs EUS-guided gallbladder drainage in unfit patients
Answer:
For patients unfit for surgery (Grade III cholecystitis + high operative risk):
Percutaneous Cholecystostomy (PCT):
- Ultrasound or CT-guided transhepatic or transperitoneal tube drain
- Decompresses infected GB; buys time for patient optimisation
- Limitations: tube can dislodge, pain, requires patent cystic duct, tube-dependent complications, 30–40% recurrence after tube removal without interval cholecystectomy
EUS-Guided Gallbladder Drainage (EUS-GBD) with LAMS (Lumen-Apposing Metal Stent):
- Endoscopic access through stomach or duodenum into GB with a LAMS stent
- Advantages: internal drainage (no external bag), sustained patency, allows stone retrieval through stent, lower recurrence
Evidence:
The DRAC 1 trial (RCT) demonstrated EUS-GBD with LAMS was superior to PCT for:
- Technical success
- Lower adverse event rate
- Improved quality of life
- Lower readmission for recurrent cholecystitis
Current guideline position: EUS-GBD has Level I evidence over PCT in patients who are poor surgical candidates and where ERCP/lap-C is not feasible. This is endorsed by ESGE and WSES guidelines.
💡 Final Rapid-Fire Summary Card
| Topic | Key Number/Answer |
|---|---|
| BDI rate in STC | 0.3% |
| BDI rate in standard lap-C | 0.3–0.6% |
| Bile leak in STC | 13.5%, RR 6.07 |
| Readmission post-STC | 17.8% |
| Reoperation post-STC | 6.3% |
| ERCP needed post-STC | 16.2% |
| Mortality RR (STC vs TC) | 1.52, p=0.166 (NS) |
| Better STC technique | r-STC |
| I² for bile leak | 86.1% (considerable heterogeneity) |
| CVS criteria | 3: clear triangle + only 2 structures + lower 1/3 detached |
| Tokyo Grade III organ systems | 6: CVS, neuro, resp, renal, hepatic, haematological |
| Mirizzi Type I vs II | Compression vs Fistula |
All the best — you are well prepared. Own your data! 🎯
Sources: Current Surgical Therapy 14e | Mulholland & Greenfield Surgery 7e | Bailey & Love 28th Ed. | Sleisenger & Fordtran GI & Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.