Filariasis clinica and laboratory presentation and diagnosis in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"lymphatic filariasis"[MeSH Terms] AND diagnosis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material from Harrison's 22e, Tietz Lab Medicine, Robbins Pathology, Bailey & Love, and Park's. Let me compile the full, detailed answer.
Filariasis: Clinical Presentation, Laboratory Features, and Diagnosis
1. Overview and Causative Organisms
Lymphatic filariasis is caused by three closely related threadlike nematodes:
- Wuchereria bancrofti - responsible for ~90% of all cases; distributed throughout tropics/subtropics worldwide (Africa, Asia, Pacific Islands, South America, Caribbean)
- Brugia malayi - restricted to eastern India, Southeast Asia, Indonesia, Malaysia, Philippines
- Brugia timori - limited to islands of southeastern Indonesia
Other filariae affecting humans include Loa loa (loiasis), Onchocerca volvulus (onchocerciasis/river blindness), and Mansonella spp., each with distinct clinical and laboratory features.
Adult worms are long slender nematodes (up to 20 cm) that reside in afferent lymphatics and lymph node sinuses, where they may remain viable for more than two decades. - Harrison's Principles of Internal Medicine 22e
2. Epidemiology and Transmission
| Organism | Periodicity | Distribution | Vector |
|---|---|---|---|
| W. bancrofti | Nocturnal (subperiodic in Pacific) | Global tropics | Culex, Anopheles mosquitoes |
| B. malayi | Nocturnal / subperiodic | Southeast Asia, India | Mansonia, Anopheles |
| B. timori | Subperiodic | Indonesia | Coquillettidia, Mansonia |
| Loa loa | Diurnal | West/Central Africa | Chrysops deerflies |
| O. volvulus | None (aperiodic) | Africa, S. America | Simulium blackflies |
Approximately 120 million people are infected worldwide; 40 million have symptomatic lymphedema or elephantiasis. Over 893 million people live in at-risk areas across 49 countries. - Park's Textbook of Preventive and Social Medicine
Nocturnal periodicity means microfilariae are scarce in peripheral blood by day and increase at night - blood collection must be timed accordingly (optimally 10 PM to 2 AM for W. bancrofti and Brugia spp.).
3. Pathogenesis
The principal pathologic changes result from inflammatory damage to lymphatics caused by adult worms, not microfilariae. Key mechanisms include:
- Adult worms in afferent lymphatics cause lymphatic dilation and vessel wall thickening
- Infiltration of plasma cells, eosinophils, and macrophages, plus endothelial/connective tissue proliferation, leads to tortuosity and incompetent lymph valves
- Th1-mediated granuloma formation around adult parasites causes direct lymphatic damage
- Th2-mediated responses (IL-4, IL-5) drive IgE production and eosinophilia - associated with tropical pulmonary eosinophilia
Filarial parasites actively evade immunity via:
-
Elastases and trypsin-like proteases (tissue invasion)
-
Surface glycoproteins with antioxidant function (resistance to reactive oxygen species)
-
Cystatin homologues (impair MHC class II antigen processing)
-
Serpins (inhibit neutrophil proteases)
-
TGF-β and macrophage migration inhibition factor homologues (dampen immune response)
-
Wolbachia endosymbionts - intracellular bacteria required for nematode development and reproduction; their release contributes to inflammatory reactions
-
Robbins, Cotran & Kumar Pathologic Basis of Disease
4. Clinical Presentation
4a. Spectrum of Disease
Filariasis produces a clinical spectrum ranging from completely asymptomatic to severely disabling:
-
Asymptomatic microfilaremia - the most common state; microfilariae circulate in blood without clinical manifestations. However, even these patients typically show subclinical lymphatic damage on lymphoscintigraphy, plus hematuria and proteinuria on investigation.
-
Acute filarial episodes (Acute Dermato-Lymphangio-Adenitis, ADLA) - episodes of fever, malaise, and acute inflammation of lymph nodes and vessels
-
Chronic lymphatic disease - lymphedema, elephantiasis, hydrocele, chyluria
-
Tropical pulmonary eosinophilia (TPE) - a hypersensitivity syndrome
-
Atypical forms - filarial arthritis, filarial orchitis, rare presentations
4b. Asymptomatic Microfilaremia
- Large numbers of microfilariae in blood with no overt symptoms
- Subclinical lymphatic dilation and dysfunction demonstrable by lymphoscintigraphy
- Microscopic hematuria and proteinuria may be present on urinalysis
4c. Acute Manifestations
Acute Adenolymphangitis (ADL):
- Recurrent episodes of high fever, rigors, myalgia, and headache
- Painful lymphadenopathy (typically inguinal, axillary)
- Retrograde lymphangitis (spreading distally from lymph node, unlike bacterial ascending lymphangitis)
- Episodes last days to weeks; resolve spontaneously but recur
- Scrotal involvement: acute filarial epididymo-orchitis, funiculitis - very common with W. bancrofti
Filarial fever:
- High-grade fever with intense sweating
- May occur without apparent lymphangitis
- Associated with death of adult worms
4d. Chronic Manifestations
Lymphedema and Elephantiasis:
- Progressive, non-pitting edema of extremities (legs > arms), scrotum, penis, vulva, breast
- Initially soft and pitting; over years becomes non-pitting, fibrotic
- End-stage elephantiasis: massive limb enlargement with rough, hyperkeratotic, fissured "elephant" skin
- Secondary bacterial and fungal superinfections accelerate progression
Histopathology of elephantoid skin:
- Dilated dermal lymphatics
- Widespread lymphocytic infiltrates
- Focal cholesterol deposits
- Thickened, hyperkeratotic epidermis
Hydrocele:
- Most common manifestation of W. bancrofti in males
- Hydrocele fluid contains cholesterol crystals, red cells, hemosiderin; induces thickening/calcification of tunica vaginalis
Chyluria:
- Lymphatic fistula into the renal pelvis or bladder
- Milky-white urine due to chyle (lymph + fat) in urine
- Associated with chylous ascites or chylothorax in severe cases
Scrotal elephantiasis:
 Scrotal and penile elephantiasis due to filariasis - Bailey & Love's Short Practice of Surgery
Scrotal and penile elephantiasis due to filariasis - Bailey & Love's Short Practice of Surgery
4e. Tropical Pulmonary Eosinophilia (TPE)
A distinct hyperresponsive syndrome, more common in India and Southeast Asia:
- Paroxysmal nocturnal cough and wheeze (asthma-like)
- Bilateral interstitial infiltrates on chest X-ray
- Extremely high blood eosinophil count (>3000/μL)
- Very high serum IgE (often >1000 IU/mL)
- Absence of microfilaremia in peripheral blood (microfilariae trapped in lungs)
- Meyers-Kouwenaar bodies on lung biopsy: dead microfilariae surrounded by stellate, hyaline, eosinophilic precipitates within small epithelioid granulomas
5. Laboratory Findings
5a. Peripheral Blood
| Finding | Detail |
|---|---|
| Eosinophilia | Very common; often 15-30% in early/active infection; extremely elevated in TPE (>3000/μL absolute) |
| Microfilaremia | Microfilariae detectable in peripheral blood (nocturnal sample required) |
| Elevated IgE | Especially in TPE; total IgE often >1000 IU/mL |
| Filarial antigen | Detectable by immunochromatographic tests (ICT) |
| Lymphocytosis | May be seen in active lymphatic involvement |
| Elevated ESR | Non-specific; raised in active disease |
Urinalysis in Bancroftian filariasis:
- Microhematuria (even in asymptomatic microfilaremia)
- Proteinuria
- Chyluria: milky urine with fat droplets and lymphocytes
5b. Microfilarial Morphology - Key Differentiating Features
The principal characteristics used to identify microfilaria species are:
- Size (length and width in micrometers)
- Presence or absence of a sheath and its staining characteristics
- Shape of the tail
- Appearance and column of internal nuclei
- Distribution of nuclei in head and tail regions
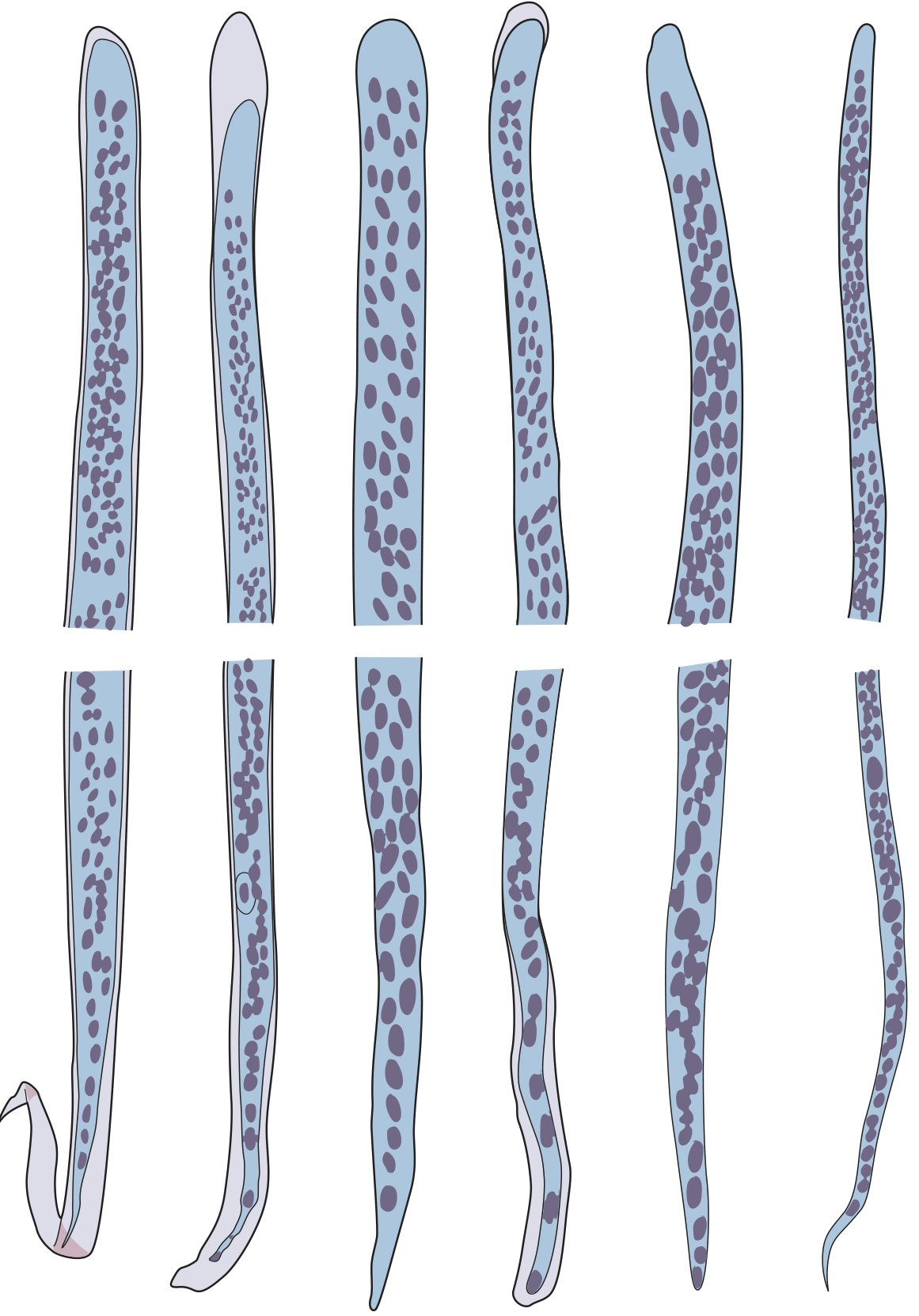
Species-specific morphology:
| Species | Sheath | Sheath stain | Length (~μm) | Tail nuclei | Periodicity |
|---|---|---|---|---|---|
| W. bancrofti | Present | Unstained/pale | 244-296 | Do NOT reach tail tip | Nocturnal |
| B. malayi | Present | Deep pink (Giemsa) | 220-260 | Two discrete nuclei in tail (subterminal + terminal) | Nocturnal |
| B. timori | Present | Unstained | 310-325 (larger than B. malayi) | Similar to B. malayi | Nocturnal |
| Loa loa | Present | Unstained/pale | 250-300 | Nuclei extend to tip of tail | Diurnal |
| O. volvulus | Absent | - | 150-287 (in skin) | Nuclei do NOT reach tail tip | Aperiodic |
| M. perstans | Absent | - | 190-200 (blood smear) | Blunt tail; nuclei reach tail tip | Aperiodic |
| M. ozzardi | Absent | - | 163-203 (blood smear) | Tapered, often hooked tail; nuclei do NOT reach tip | Aperiodic |
The sheath is a remnant of the egg membrane and is a critical identifying feature:
- Sheathed species: W. bancrofti, B. malayi, B. timori, Loa loa
- Unsheathed species: O. volvulus, Mansonella spp.
6. Diagnostic Methods
6a. Microscopic Detection of Microfilariae (Gold Standard)
Timing of sample collection is critical:
- W. bancrofti, B. malayi, B. timori: collect between 10 PM and 2 AM (nocturnal periodicity)
- Loa loa: collect between 10 AM and 2 PM (diurnal periodicity)
- Mansonella spp., O. volvulus: any time (aperiodic)
Specimen types:
- Blood (lymphatic filariasis, loiasis): thick and thin blood films; Giemsa stain
- Skin snip (onchocerciasis, M. streptocerca): bloodless skin snip (avoid blood contamination), incubated in saline, microfilariae emerge within 30-60 minutes
Blood smear techniques:
- Thick blood film (Giemsa-stained) - standard; allows morphologic study of sheath and nuclear column
- Wet film - motile microfilariae seen immediately; no staining required; does not allow species ID
- Knott's concentration method - lyse 1 mL blood in 9 mL of 2% formalin; centrifuge; examine sediment; significantly increases sensitivity
- Nuclepore (polycarbonate) membrane filtration - pass blood through 3 μm or 5 μm polycarbonate filter; fix and stain filter; highest sensitivity
- Tietz Textbook of Laboratory Medicine 7e
6b. Antigen Detection (Immunochromatographic Card Test / ICT)
- Detects circulating filarial antigen (CFA) of W. bancrofti
- BinaxNOW Filariasis and Og4C3 ELISA are the standard tests
- Sensitivity: ~96-100%, Specificity: ~99% for W. bancrofti
- Can be performed at any time of day - no need for nocturnal sampling
- Does NOT require concentration techniques
- Not applicable for Brugia spp. (no equivalent approved antigen test)
- WHO recommends ICT as the primary surveillance and diagnostic tool for W. bancrofti
6c. Antibody Detection (Serology)
- Filarial-specific IgG4 antibodies are the most useful serologic marker
- IgG4 correlates with active infection; IgG4 titers fall after successful treatment
- Cross-reactivity with other helminths (Strongyloides, Toxocara) limits specificity
- Useful in: returning travelers from endemic regions (usually microfilaria-negative), low-intensity infections
- Cannot distinguish current from past infection in residents of endemic areas
- ELISA using Brugia recombinant antigen BmR1 has been developed for brugian filariasis
6d. Molecular Diagnosis (PCR)
- Real-time PCR targeting species-specific DNA sequences (e.g., SspI repeat for W. bancrofti)
- Higher sensitivity than microscopy, especially in low-density microfilaremia
- Can simultaneously identify and differentiate W. bancrofti, B. malayi, B. timori
- Used for blood, urine, and hydrocele fluid
- Not widely available outside reference laboratories
- WHO uses PCR for post-treatment surveillance
6e. Imaging
Scrotal Ultrasound ("Filarial Dance Sign"):
- High-frequency (7.5 MHz or higher) ultrasound of the scrotum
- Filarial dance sign: characteristic rapid, random movements of live adult worms within dilated lymphatics of the spermatic cord - pathognomonic of active lymphatic filariasis
- Can be performed at any time; does not require nocturnal timing
- Allows assessment of adult worm burden and treatment response
Lymphoscintigraphy:
- Radiolabeled colloid (technetium-99m) injected intradermally in foot; imaging shows lymphatic flow
- Reveals subclinical lymphatic dysfunction in asymptomatic microfilaremic individuals
- Useful for staging lymphedema and planning treatment; not routine in clinical practice
Chest X-ray (in TPE):
- Bilateral interstitial infiltrates
- Diffuse miliary or reticulonodular pattern
- May be normal despite severe symptoms
6f. Urinalysis (Chyluria workup)
- Milky white urine (chyluria): centrifuge - lymphocytes and fat globules in pellet
- Sudan III stain for fat droplets in urine
- Protein: elevated
- Microscopy: microfilariae may be present in urine in W. bancrofti infection
6g. Skin Snip (for Onchocerciasis)
- Bloodless 2-3 mg biopsy of skin (scapular, gluteal, or calf areas)
- Incubate in normal saline at room temperature for 30-60 min (or overnight)
- Emergent microfilariae counted under low-power microscopy
- Specific for O. volvulus and M. streptocerca
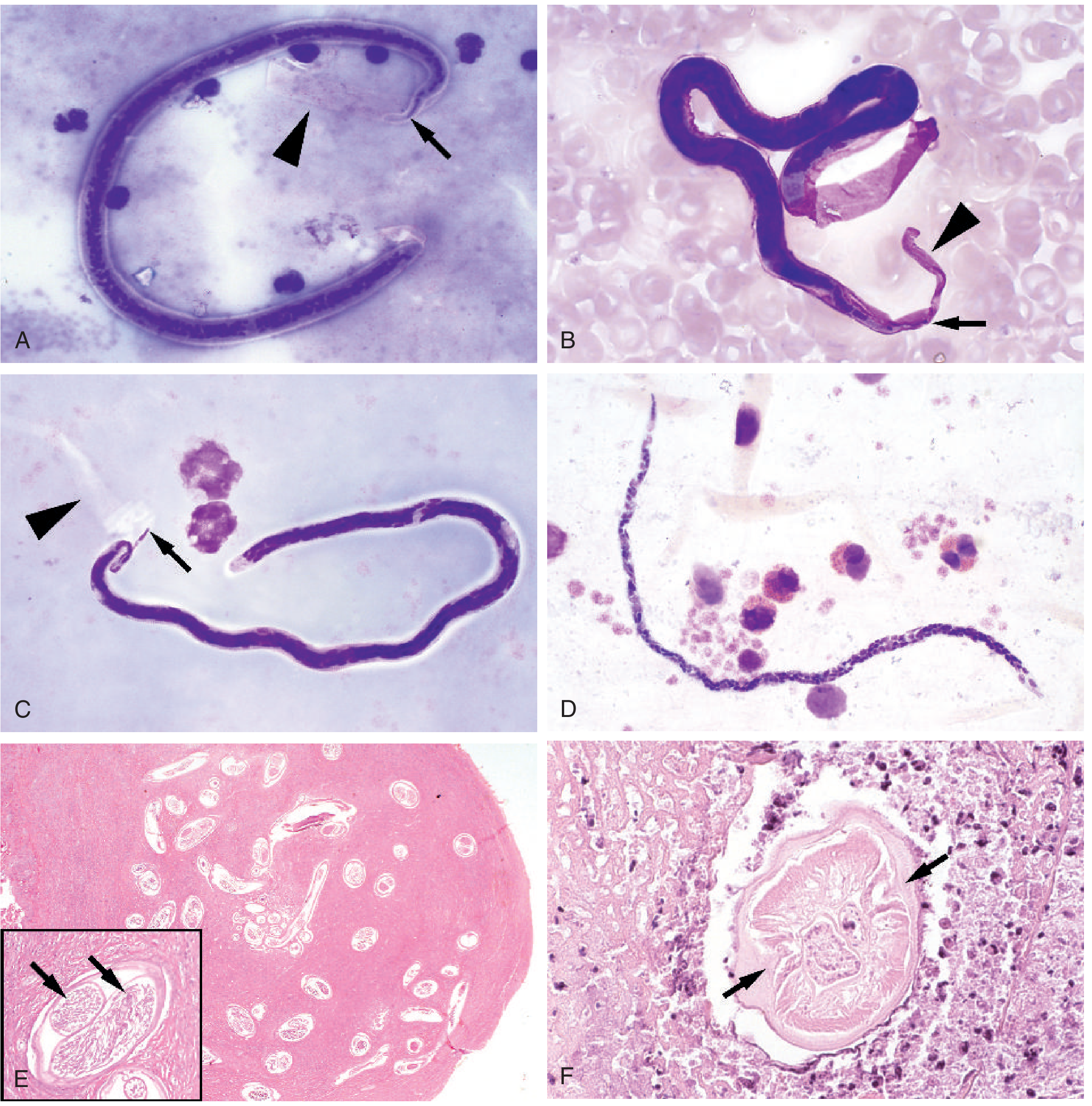
6h. Histopathology / Biopsy
- Lymph node or lymph vessel biopsy: adult worms may be found in dilated lymphatics
- Worms may be surrounded by minimal inflammation (viable), or by eosinophilic infiltrates with hemorrhage/fibrin (dying), or by granulomas (dead)
- Dilated lymphatics with polypoid infoldings over time
- Lung biopsy in TPE: Meyers-Kouwenaar bodies (stellate hyaline precipitates around dead microfilariae in epithelioid granulomas)
7. Summary of Diagnostic Approach
Suspected Filariasis
|
Is the patient from endemic area / returning traveler?
|
├── YES: Check microfilarial periodicity
│ ├── Nocturnal (W. bancrofti, Brugia spp.) → Night blood sample (10 PM–2 AM)
│ └── Diurnal (Loa loa) → Day blood sample (10 AM–2 PM)
|
Blood examination:
1. Thick smear + Giemsa stain → species ID by morphology
2. Knott's concentration OR Nuclepore filtration (higher sensitivity)
3. Wet prep (motility check)
|
If negative / W. bancrofti suspected:
4. CFA (Og4C3 ELISA or BinaxNOW ICT) → any time of day
5. Filarial-specific IgG4 (serology)
6. PCR (reference lab)
|
Imaging:
7. Scrotal ultrasound → Filarial dance sign (adult worms)
8. Lymphoscintigraphy (subclinical lymphatic dysfunction)
|
Special:
9. Skin snip → O. volvulus, M. streptocerca
10. Urine exam → chyluria, microfilariae
11. Lung biopsy → Meyers-Kouwenaar bodies in TPE
8. Key Laboratory Markers at a Glance
| Test | What it detects | Timing | Best use |
|---|---|---|---|
| Thick blood smear (Giemsa) | Microfilariae (species by morphology) | Nocturnal (mostly) | Standard diagnosis |
| Knott's concentration | Microfilariae (concentrated) | Nocturnal | Low-density microfilaremia |
| Nuclepore filtration | Microfilariae (most sensitive) | Nocturnal | Low-density |
| Wet film | Motile microfilariae | Nocturnal | Quick screen |
| CFA (Og4C3 / ICT) | W. bancrofti adult antigen | Anytime | W. bancrofti, any hour |
| IgG4 ELISA | Filarial antibody | Anytime | Travelers, low intensity |
| PCR | Parasite DNA | Anytime | Reference lab, post-treatment |
| Scrotal US | Adult worm motion | Anytime | Active lymphatic filariasis |
| Skin snip | O. volvulus microfilariae | Anytime | Onchocerciasis |
| Eosinophil count | Eosinophilia | Anytime | Screening, TPE |
| Total IgE | Elevated in TPE | Anytime | TPE diagnosis |
| Chest X-ray | Interstitial infiltrates | Anytime | TPE |
Sources:
- Harrison's Principles of Internal Medicine 22e (2025), Chapter 240: Lymphatic Filariasis
- Tietz Textbook of Laboratory Medicine 7e, Chapter 88: Filarial Infections
- Robbins, Cotran & Kumar Pathologic Basis of Disease, Chapter 8: Lymphatic Filariasis
- Park's Textbook of Preventive and Social Medicine: Lymphatic Filariasis (Epidemiology)
- Bailey and Love's Short Practice of Surgery 28e: Filariasis
This is a shared conversation. Sign in to Orris to start your own chat.