Symapthatic out flow starting from limbic system plz exaplin the sympatic ganglia and pre vertebral ganglia
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have all the essential information and diagrams needed. Let me compile a comprehensive, well-structured answer.
Sympathetic Outflow: From Limbic System to End Organs
1. The Hierarchy: Where It All Begins
The sympathetic nervous system does not operate in isolation - it is under higher cortical and limbic control. The chain of command flows top-down:
Limbic System (Amygdala, Hippocampus, Cingulate Cortex)
↓
Hypothalamus (Integration Center)
↓
Brainstem (Medulla - cardiovascular/respiratory centers)
↓
Intermediolateral Cell Column (IML) - Spinal Cord T1–L2/L3
↓
Sympathetic Ganglia (Paravertebral / Prevertebral)
↓
End Organs
Limbic System → Hypothalamus
The limbic system (amygdala, cingulate cortex, hippocampus, prefrontal limbic cortex) generates emotional and stress responses. Signals from limbic structures project to the hypothalamus, which acts as the master integrator of autonomic output. As Guyton and Hall states:
"The autonomic nervous system is activated mainly by centers located in the spinal cord, brain stem, and hypothalamus. In addition, portions of the cerebral cortex, especially of the limbic cortex, can transmit signals to the lower centers and in this way can influence autonomic control."
- Guyton and Hall Textbook of Medical Physiology
When the hypothalamus is activated by fright, severe pain, or emotional stress, it can trigger a mass sympathetic discharge - the classic "fight-or-flight" or alarm response.
Hypothalamus → Spinal Cord
Hypothalamic projections descend through the brainstem (specifically the rostral ventrolateral medulla - RVLM) and the reticulospinal tracts to reach the intermediolateral (IML) cell column of the spinal cord.
2. The First-Order Neuron: Preganglionic Sympathetic Neurons
- Location: Intermediolateral (lateral) horn of the spinal cord, at levels T1 to L2 (or L3)
- These neurons lie in Lamina VII, between the dorsal and ventral horns - this is why the lateral horn appears at T1-L2 only (not at cervical or lower lumbar/sacral levels)
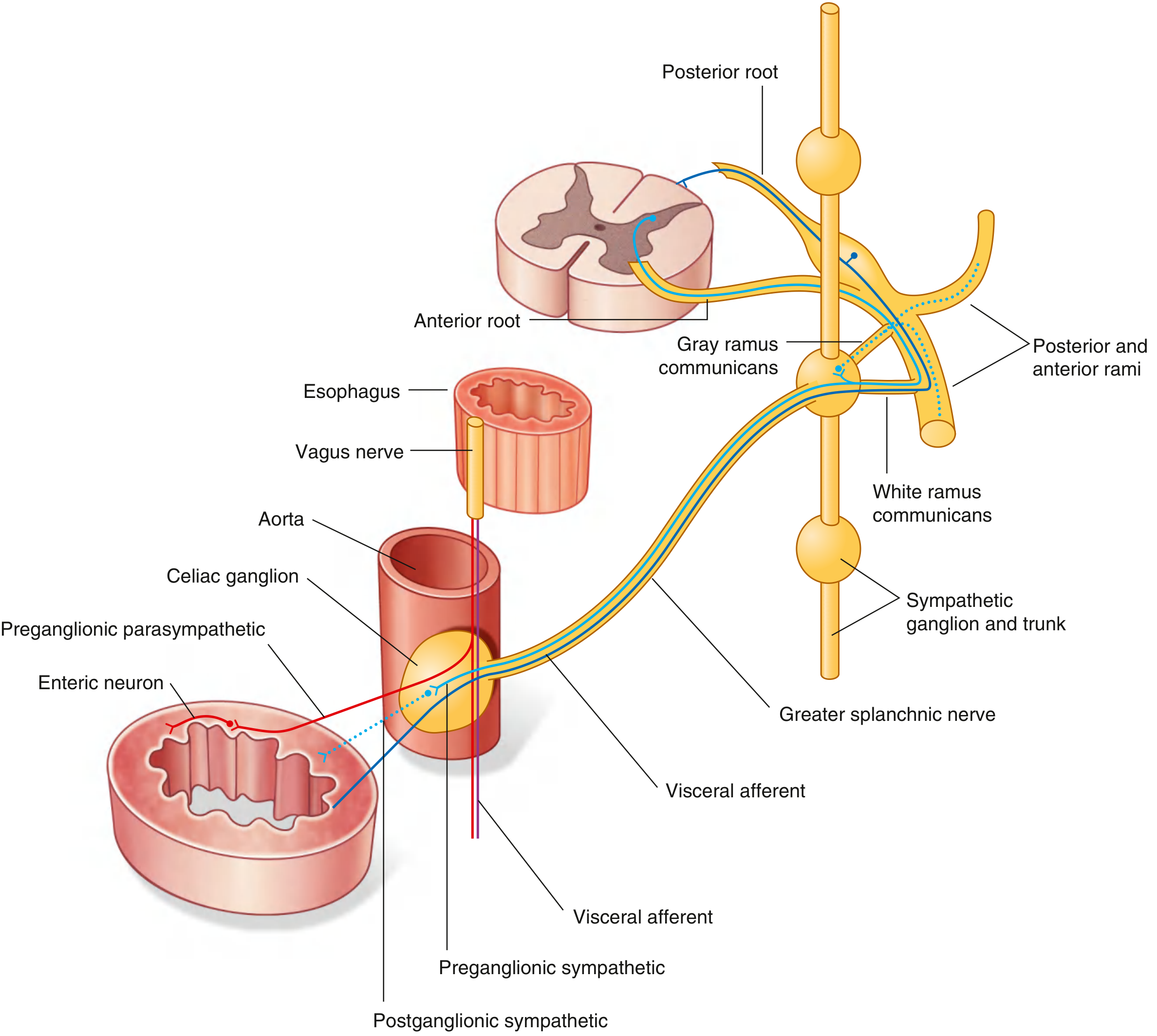
- Axon route: Exits via the ventral root → enters the spinal nerve → diverges into the white ramus communicans → enters the sympathetic chain ganglion
The white ramus is myelinated (hence white). White rami are found only at T1-L2 because preganglionic fibers only emerge at these levels.
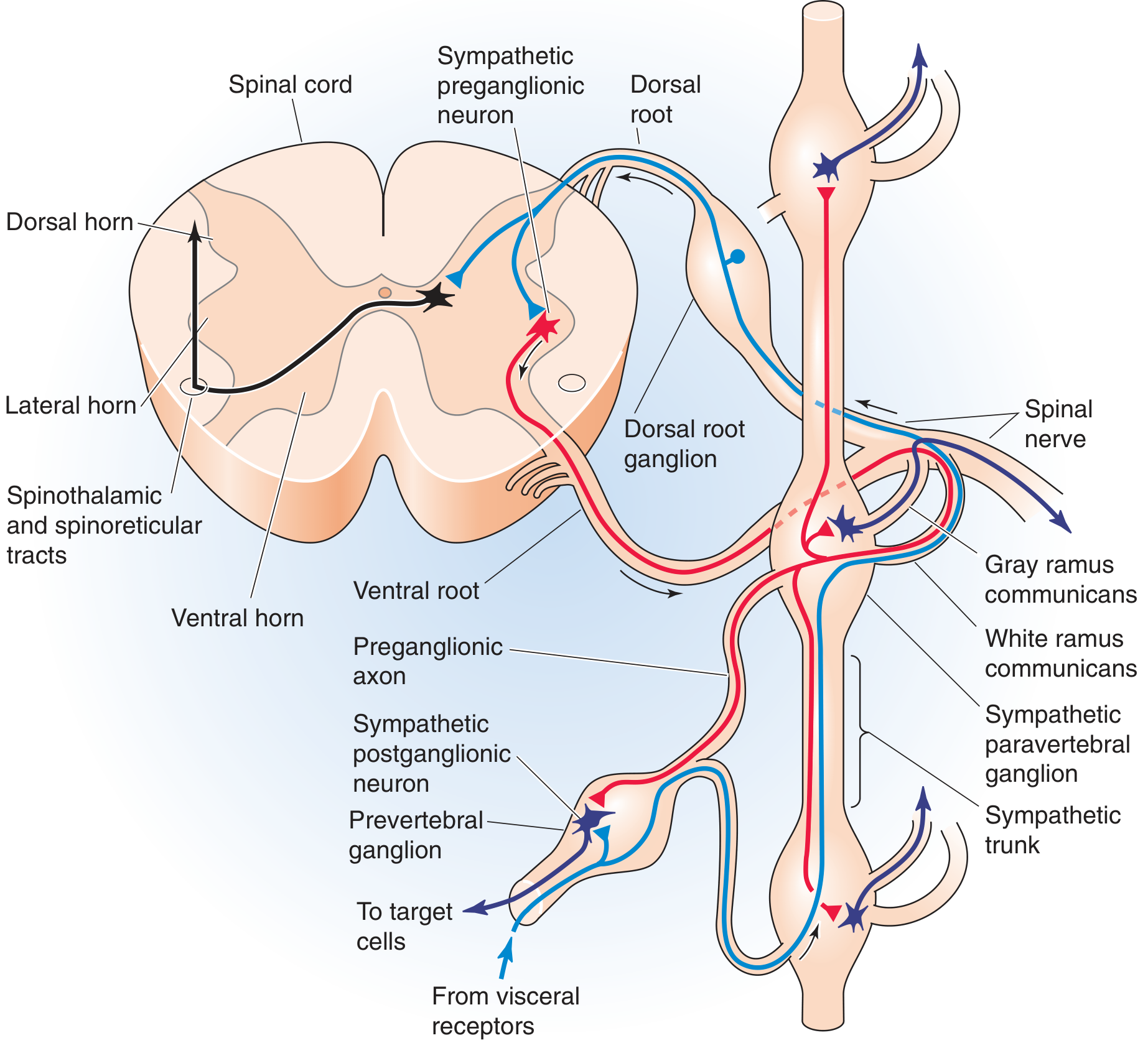
Figure: Cross-section of thoracic spinal cord showing the preganglionic sympathetic neuron (red) in the lateral horn, exiting via the ventral root, passing through the white ramus to reach the paravertebral ganglion and prevertebral ganglion. (Medical Physiology)
3. Sympathetic (Paravertebral) Ganglia
These are also called the sympathetic chain ganglia or sympathetic trunk ganglia.
Structure
- A bilateral chain of ganglia running on either side of the vertebral column
- Extends from the upper cervical region all the way down to the coccyx, where the two chains merge as the coccygeal (ganglion impar)
- Although preganglionic fibers only emerge at T1-L2, the chain itself spans C1 to coccyx - this is how sympathetics reach the head, neck, and lower limbs
Named Cervical Ganglia (rostral fusions)
| Ganglion | Spinal Levels Fused | Supplies |
|---|---|---|
| Superior cervical ganglion | C1-C4 | Head, neck, eye (pupil dilation, lid retraction), salivary glands |
| Middle cervical ganglion | C5-C6 (often absent) | Heart, lungs |
| Inferior cervical ganglion (usually fused with T1 = Stellate ganglion) | C7-C8 + T1 | Heart, lungs, bronchi, upper limb |
The stellate ganglion is clinically important - stellate ganglion blockade is used for conditions like long QT syndrome, refractory ventricular arrhythmias, and pain management.
What happens to a preganglionic fiber entering a chain ganglion?
Once the preganglionic axon enters a paravertebral ganglion through the white ramus, it has three possible fates:
- Synapse in that same segmental ganglion - then the postganglionic fiber exits via the gray ramus
- Travel up or down the sympathetic chain to synapse in a ganglion at a different level (this is how T1 reaches the head via the superior cervical ganglion)
- Pass straight through without synapsing - continuing as a splanchnic nerve to reach a prevertebral ganglion
Postganglionic fibers from paravertebral ganglia
- Exit via the gray ramus communicans (unmyelinated, hence gray) → rejoin the spinal nerve → distribute to the body wall, skin, blood vessels, sweat glands, piloerector muscles
- Gray rami are present at every spinal level (C2 to coccyx), even though white rami only exist at T1-L2
- Some postganglionic fibers travel directly to target organs (heart, lungs) along blood vessels
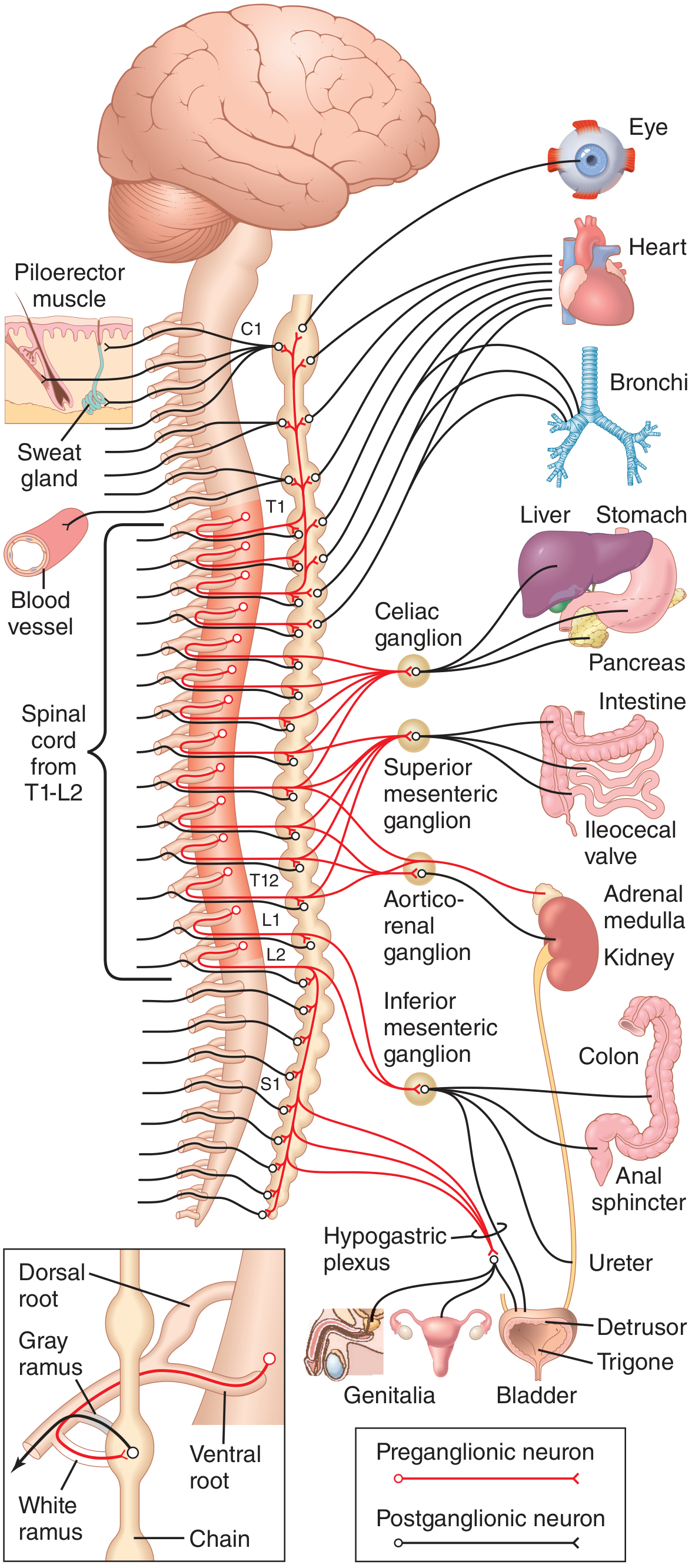
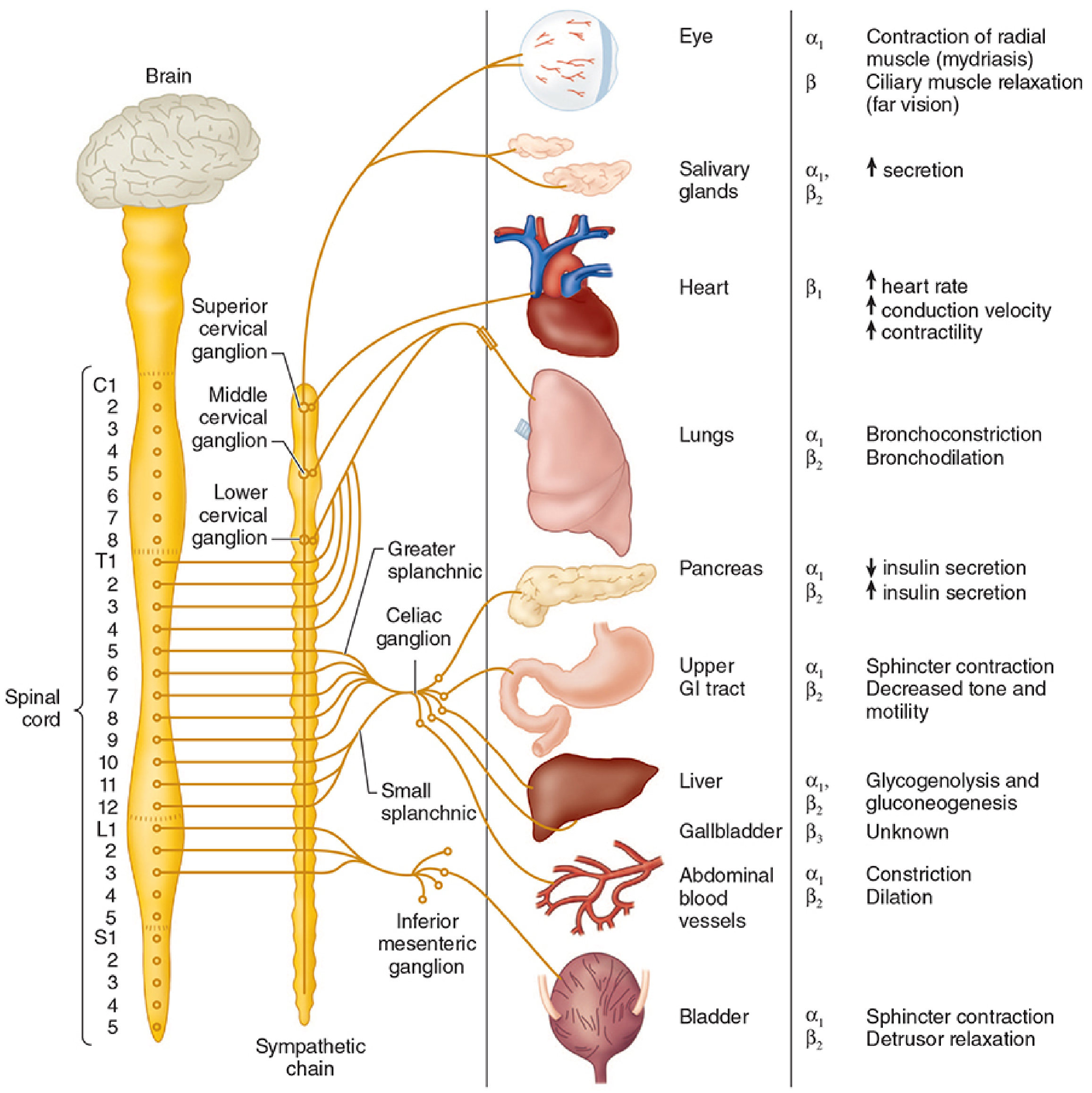
Figure: The complete sympathetic system (Guyton & Hall). Red = preganglionic fibers. Black = postganglionic fibers. Note the prevertebral ganglia (celiac, superior mesenteric, aorticorenal, inferior mesenteric) and the hypogastric plexus supplying abdominal and pelvic organs.
4. Prevertebral (Collateral) Ganglia
These are the second set of sympathetic ganglia. They differ fundamentally from paravertebral ganglia:
| Feature | Paravertebral Ganglia | Prevertebral Ganglia |
|---|---|---|
| Location | Bilateral, beside vertebral column | Anterior to aorta and its branches |
| Paired? | Yes (bilateral chain) | Unpaired (midline) |
| Level | Cervical to coccyx | Abdominal/pelvic only |
| Reach | Somatic structures, head/neck, heart/lungs | Abdominal and pelvic viscera |
How preganglionic fibers reach them
Preganglionic fibers pass through the sympathetic chain without synapsing, forming the splanchnic nerves:
- Greater splanchnic nerve (T5-T9) → celiac ganglion
- Lesser splanchnic nerve (T10-T11) → superior mesenteric ganglion / aorticorenal ganglion
- Least splanchnic nerve (T12) → aorticorenal ganglion
- Lumbar splanchnic nerves (L1-L2) → inferior mesenteric ganglion
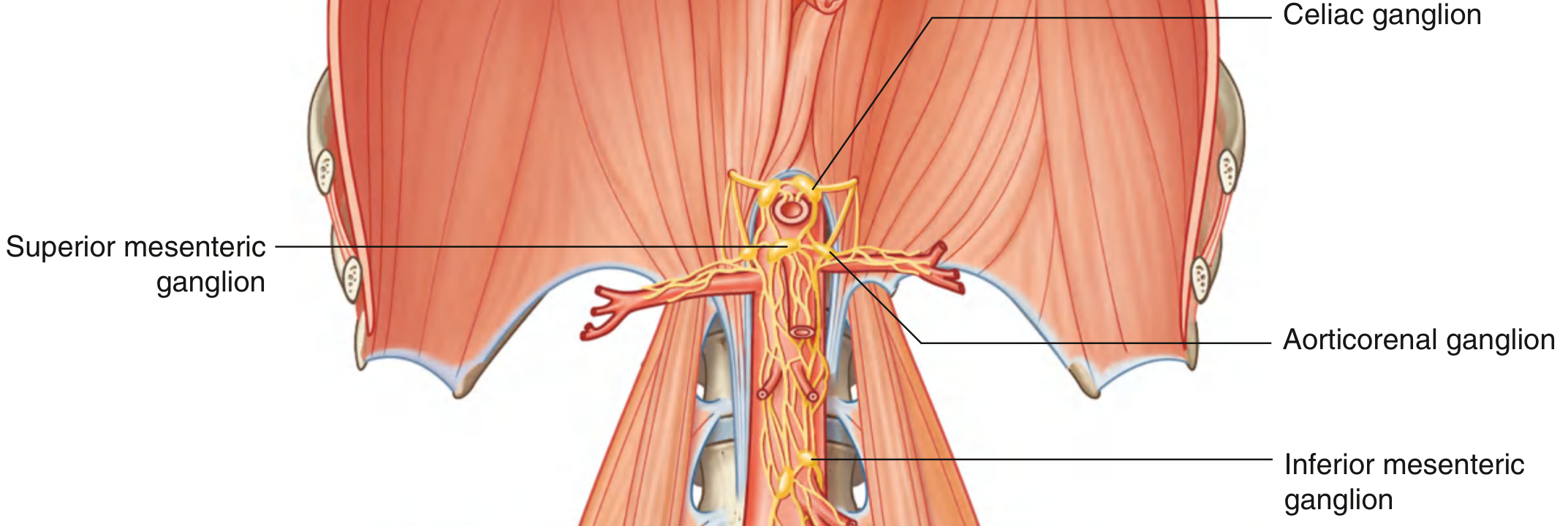
The Four Major Prevertebral Ganglia
| Ganglion | Artery it lies near | Supplies |
|---|---|---|
| Celiac ganglion | Celiac artery | Stomach, liver, gallbladder, spleen, pancreas, small intestine (proximal) |
| Superior mesenteric ganglion | Superior mesenteric artery | Small intestine, ascending and transverse colon |
| Aorticorenal ganglion | Renal artery origin | Kidney, ureter (upper) |
| Inferior mesenteric ganglion | Inferior mesenteric artery | Descending and sigmoid colon, rectum, bladder, genitalia |
The hypogastric plexus (from inferior mesenteric + lumbar splanchnic input) is also included in some classifications as a plexus associated with pelvic organ innervation.
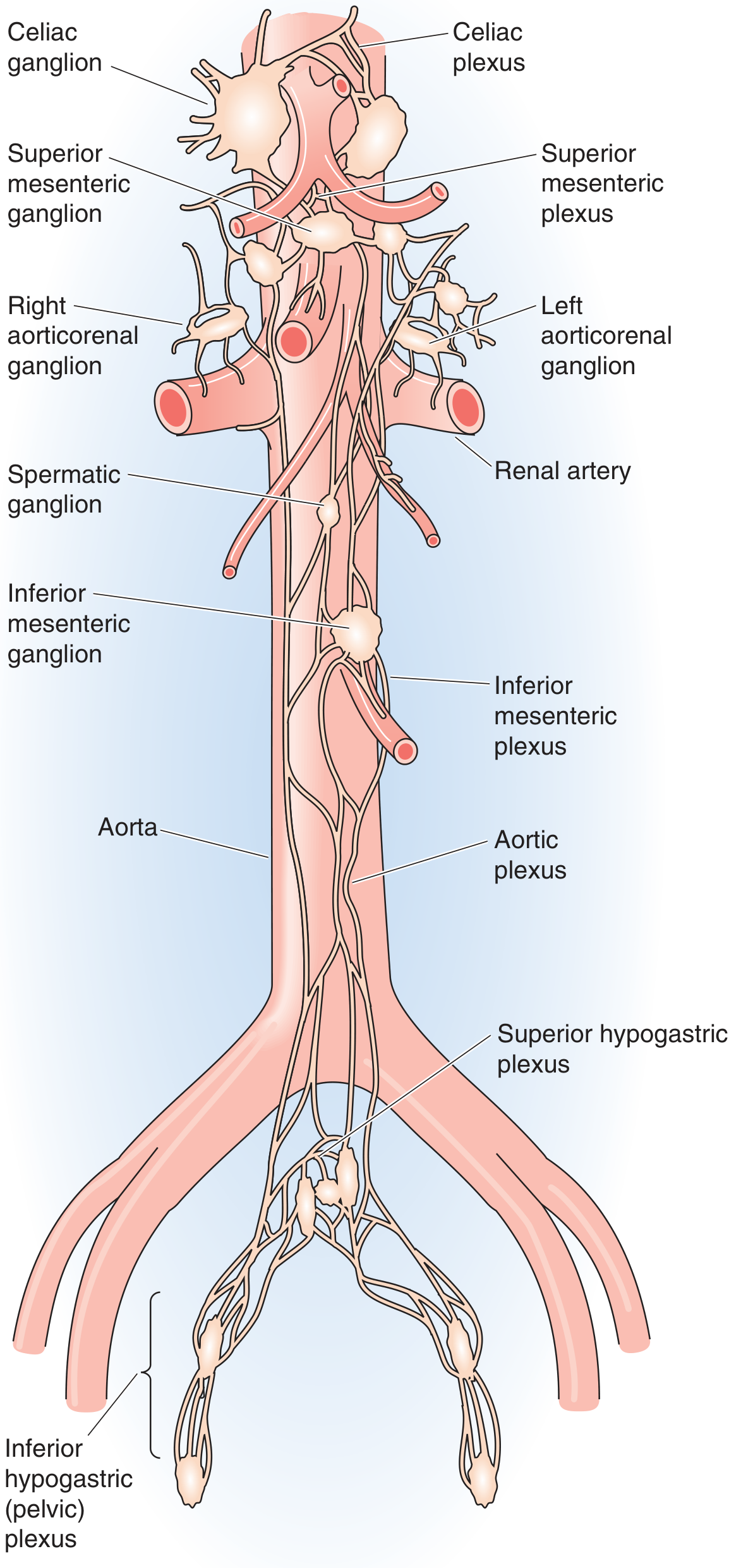
Figure: Prevertebral sympathetic plexus - each ganglion is named after the artery it sits adjacent to. (Medical Physiology)
5. The Postganglionic Neuron - Final Leg
- Cell bodies in paravertebral or prevertebral ganglia send long unmyelinated (type C) postganglionic axons to target organs
- Postganglionic fibers travel either along blood vessels or within peripheral nerves
- Neurotransmitter: Norepinephrine (noradrenaline) at most end organs - acting on α1, α2, β1, β2, β3 receptors
- Exception: Sweat glands and some blood vessels receive sympathetic postganglionic fibers that release acetylcholine (cholinergic sympathetic fibers)
Special Case: Adrenal Medulla
- Preganglionic fibers pass without synapsing all the way through the sympathetic chain and the splanchnic nerves directly to the adrenal medulla
- The adrenal medullary cells are essentially modified postganglionic neurons
- They release epinephrine (80%) and norepinephrine (20%) directly into the bloodstream
- This is why adrenal medulla stimulation = systemic sympathetic amplification
6. Divergence: Why Sympathetics Are "Widespread"
Each preganglionic sympathetic neuron synapses on approximately 200 postganglionic neurons (in contrast to the parasympathetic system which is far more localized). This divergence:
- Enables mass discharge (alarm/stress response)
- Explains why emotional/stress activation from the limbic system leads to widespread body-wide effects (tachycardia + hypertension + mydriasis + bronchodilation + sweating - all simultaneously)
7. Summary Pathway
LIMBIC SYSTEM (Amygdala, Cingulate Cortex)
↓ (via limbic-hypothalamic projections)
HYPOTHALAMUS (Posterior/Lateral hypothalamic areas)
↓ (via reticulospinal / hypothalamospinal tracts, through brainstem RVLM)
INTERMEDIOLATERAL HORN, T1-L2/L3
(Preganglionic neuron - myelinated B fiber, releases ACh → nicotinic receptor)
↓
WHITE RAMUS COMMUNICANS
↓
SYMPATHETIC CHAIN (PARAVERTEBRAL GANGLIA)
├─ Synapse here → postganglionic exits via GRAY RAMUS → body wall, skin, head/neck
├─ Travel up/down chain → synapse at different level (e.g., T1→ superior cervical ganglion → head)
└─ Pass through as SPLANCHNIC NERVES →
↓
PREVERTEBRAL GANGLIA (Celiac / Sup. Mesenteric / Aorticorenal / Inf. Mesenteric)
(Postganglionic neuron - unmyelinated C fiber, releases NE → α/β receptors)
↓
VISCERAL ORGANS (Gut, liver, kidney, bladder, genitalia, adrenal medulla)
Sources:
- Guyton and Hall Textbook of Medical Physiology - Chapter 61, Autonomic Nervous System
- Medical Physiology (Boron & Boulpaep) - Chapter 14, Autonomic Nervous System
- Neuroanatomy through Clinical Cases, 3rd Edition - Chapter 6, Autonomic Nervous System
Explain all three pathways loke how symapthatic outflow stimulates paraveryerbal ganglia prevertebral ganglia and adrenal medulla.
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
I now have everything needed for a detailed, well-illustrated explanation. Let me compile the full answer.
The Three Pathways of Sympathetic Outflow
All three pathways begin at the same starting point: the preganglionic neuron in the intermediolateral (IML) horn of T1-L2/L3. The pathway the preganglionic fiber then takes determines which of the three destinations it reaches. Here is each pathway explained in full detail.
Common Starting Point for All Three Pathways
Preganglionic neuron:
- Cell body in the lateral horn (intermediolateral cell column) of the spinal cord, T1 to L2/L3
- Axon exits via the ventral root → enters the spinal nerve → leaves via the white ramus communicans (myelinated, hence white)
- Enters the nearest sympathetic chain ganglion
Once inside the chain ganglion, the preganglionic axon has three possible fates - and each fate defines one of the three pathways:
"After entering a paravertebral ganglion, a preganglionic sympathetic axon has one or more of three fates. It may (1) synapse within that segmental paravertebral ganglion, (2) travel up or down the sympathetic chain to synapse within a neighboring paravertebral ganglion, or (3) enter the greater or lesser splanchnic nerve to synapse within one of the ganglia of the prevertebral plexus."
- Medical Physiology (Boron & Boulpaep)
PATHWAY 1 - To the Paravertebral (Sympathetic Chain) Ganglia
Step-by-Step Route
IML Horn (T1-L2)
↓ ventral root
Spinal nerve
↓ white ramus communicans (myelinated)
Sympathetic chain ganglion at the same level
↓ [SYNAPSE HERE - ACh → nicotinic receptor]
Postganglionic neuron (unmyelinated C fiber, releases NE)
↓ gray ramus communicans
Re-joins spinal nerve → body wall, skin, blood vessels
OR
↓ travels directly to thoracic organs
Heart / lungs / bronchi
Two sub-routes within Pathway 1
Sub-route 1a: Synapse at the same level
The preganglionic fiber synapses right inside the ganglion it first enters. The postganglionic fiber then exits via the gray ramus communicans (unmyelinated, hence gray) back into the spinal nerve. It travels out to the body wall, skin, sweat glands, piloerector muscles, and peripheral blood vessels. This is how sympathetics control thermoregulation and cutaneous vasomotor tone.
Sub-route 1b: Travel up or down the chain first, then synapse
The preganglionic fiber does NOT synapse at its entry level. Instead it ascends or descends within the sympathetic chain to reach a ganglion at a different level, and synapses there. This is the mechanism by which preganglionic fibers originating at T1-T3 can reach the cervical ganglia to supply the head, neck, and heart.
The Cervical Ganglia (key named ganglia of the chain)
| Ganglion | Formation | Spinal levels supplying it | Key targets |
|---|---|---|---|
| Superior cervical ganglion | Fusion of C1-C4 | T1-T3 ascending | Eye (pupil dilation, lid elevation), face, salivary glands, sweat glands of head |
| Middle cervical ganglion | Fusion of C5-C6 (often absent) | T1-T3 ascending | Heart, thyroid |
| Inferior cervical ganglion fused with T1 = Stellate ganglion | C7-C8 + T1 | T1-T4 | Heart, lungs, bronchi, upper limb |
| Thoracic ganglia (T2-T12) | Individual or paired | T2-T12 | Heart, lungs, aorta, esophagus |
| Lumbar ganglia (L1-L4) | Individual | T12-L2 | Lower limbs, skin, blood vessels |
| Sacral ganglia (S1-S4) | Individual | T12-L2 ascending | Pelvic viscera, lower limbs |
| Ganglion impar (coccygeal) | Fusion of both chains at coccyx | - | Perineum |
Key rule about white vs. gray rami
- White rami (myelinated, preganglionic) - found only at T1-L2 (where the preganglionic fibers emerge)
- Gray rami (unmyelinated, postganglionic) - found at every level from C2 to coccyx, because each chain ganglion sends out postganglionic fibers regardless of level
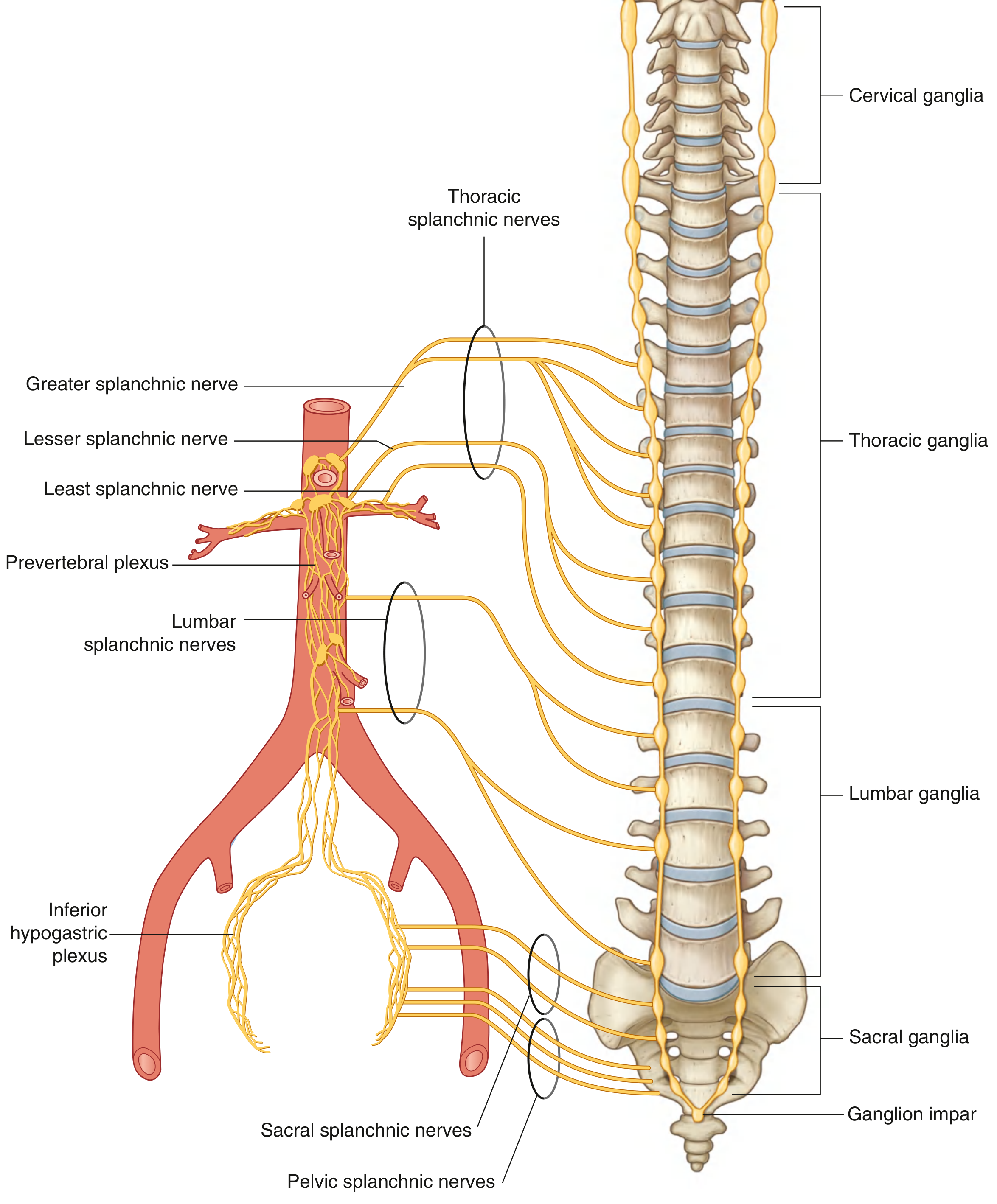
PATHWAY 2 - To the Prevertebral (Collateral) Ganglia via Splanchnic Nerves
Step-by-Step Route
IML Horn (T5-L2)
↓ ventral root → white ramus
Sympathetic chain ganglion
↓ PASSES THROUGH WITHOUT SYNAPSING
Splanchnic nerve (preganglionic fibers bundled together)
↓ crosses the diaphragm into abdomen
Prevertebral ganglion (celiac / superior mesenteric / aorticorenal / inferior mesenteric)
↓ [SYNAPSE HERE - ACh → nicotinic receptor]
Postganglionic neuron (unmyelinated, releases NE)
↓ travels along arterial branches
Abdominal and pelvic viscera
The Splanchnic Nerves - the "Highways" to Prevertebral Ganglia
This is a critically important concept: the preganglionic fiber passes right through the sympathetic chain without synapsing and bundles with other preganglionic fibers to form the splanchnic nerves. The first synapse happens only at the prevertebral ganglion.
| Splanchnic Nerve | Origin from chain | Destination ganglion | Organs supplied |
|---|---|---|---|
| Greater splanchnic nerve | T5-T9 (or T5-T10) thoracic ganglia | Celiac ganglion | Stomach, liver, gallbladder, spleen, pancreas, duodenum, small intestine (proximal) |
| Lesser splanchnic nerve | T9-T10 (or T10-T11) thoracic ganglia | Aorticorenal ganglion (+ superior mesenteric) | Kidney, upper ureter |
| Least splanchnic nerve | T12 thoracic ganglion (when present) | Renal plexus | Kidney |
| Lumbar splanchnic nerves (2-4 in number) | Lumbar sympathetic trunk/ganglia, L1-L2 | Inferior mesenteric ganglion + aortic plexus | Descending colon, sigmoid, rectum, bladder, uterus, genitalia |
| Sacral splanchnic nerves | Sacral sympathetic trunk | Inferior hypogastric (pelvic) plexus | Pelvic viscera |
The Four Prevertebral Ganglia
These ganglia lie anterior to the aorta, named after the artery they accompany:
| Ganglion | Artery | Receives input from | Supplies |
|---|---|---|---|
| Celiac ganglion | Celiac trunk | Greater splanchnic nerve (T5-T9) | Stomach, liver, gallbladder, pancreas, spleen, proximal duodenum |
| Superior mesenteric ganglion | Superior mesenteric artery | Greater/lesser splanchnic (T9-T11) | Small intestine, cecum, appendix, ascending and transverse colon |
| Aorticorenal ganglion | Renal artery origin | Lesser/least splanchnic (T10-T12) | Kidney, adrenal gland, upper ureter |
| Inferior mesenteric ganglion | Inferior mesenteric artery | Lumbar splanchnic (L1-L2) | Descending and sigmoid colon, rectum, bladder, internal genitalia |
Pathway 2 diagram - the full route (Gray's Anatomy for Students)
PATHWAY 3 - To the Adrenal Medulla (The "Endocrine Limb")
This pathway is unique and is the most direct way the sympathetic system produces a systemic, hormonal effect.
Step-by-Step Route
IML Horn (T5-T9, some say T11-L2)
↓ ventral root → white ramus
Sympathetic chain ganglion
↓ PASSES THROUGH WITHOUT SYNAPSING
Greater splanchnic nerve (preganglionic fibers)
↓ passes through celiac ganglion WITHOUT SYNAPSING
Adrenal medulla
↓ [SYNAPSE HERE - ACh → nicotinic receptor on chromaffin cells]
Chromaffin cells (= modified postganglionic neurons)
↓ release catecholamines INTO the bloodstream
Epinephrine (80%) + Norepinephrine (20%) → systemic circulation → all organs
Why the Adrenal Medulla is Unique
The adrenal medulla is essentially a modified sympathetic ganglion that has lost its axons and instead secretes directly into the blood. This makes it a neuroendocrine organ.
"The adrenal medulla is a specialized ganglion in the sympathetic division of the autonomic nervous system... the chromaffin cells of the adrenal medulla secrete catecholamines (epinephrine and norepinephrine) into the general circulation."
- Costanzo Physiology, 7th Edition
"Pharmacologically, anatomically, and embryologically, the chromaffin cells of the adrenal medulla resemble a collection of postganglionic sympathetic nerve cells."
- Goodman & Gilman's Pharmacological Basis of Therapeutics
Why epinephrine, not norepinephrine?
Regular sympathetic postganglionic neurons release norepinephrine because they lack the enzyme PNMT (phenylethanolamine-N-methyltransferase).
The adrenal medulla does have PNMT, which converts norepinephrine → epinephrine. PNMT requires cortisol for its activity, supplied via venous drainage from the overlying adrenal cortex to the medulla (the "cortico-medullary portal system").
- This is why a pheochromocytoma (tumor of chromaffin cells), when located away from the adrenal gland (ectopic), secretes predominantly norepinephrine - it lacks cortisol stimulation of PNMT.
| Regular Postganglionic Neuron | Adrenal Chromaffin Cell | |
|---|---|---|
| Stimulated by | Preganglionic ACh → nicotinic | Preganglionic ACh → nicotinic |
| Releases | Norepinephrine | Epinephrine (80%) + NE (20%) |
| Route of delivery | Synaptic cleft (local) | Bloodstream (systemic) |
| Has PNMT? | No | Yes (cortisol-dependent) |
| Has axon? | Yes (long postganglionic axon) | No (releases into blood directly) |
Side-by-Side Comparison of All Three Pathways
| Feature | Pathway 1 (Paravertebral) | Pathway 2 (Prevertebral) | Pathway 3 (Adrenal Medulla) |
|---|---|---|---|
| Where preganglionic originates | T1-L2 IML horn | T5-L2 IML horn | T5-T9 IML horn |
| Does it synapse in chain? | YES | NO (passes through) | NO (passes through) |
| Nerve carrying preganglionic | White ramus → chain | White ramus → chain → splanchnic nerve | White ramus → chain → greater splanchnic nerve |
| Ganglion location | Beside vertebral column | Anterior to aorta | Inside adrenal gland |
| Where synapse occurs | Paravertebral chain ganglion | Prevertebral ganglion | Adrenal medullary chromaffin cell |
| Postganglionic fiber | Long unmyelinated C fiber | Long unmyelinated C fiber | No axon - chromaffin cell releases into blood |
| Neurotransmitter at effector | Norepinephrine (mostly) | Norepinephrine | Epinephrine (80%) + NE (20%) bloodstream |
| Targets | Head, neck, limbs, body wall, heart, lungs | Abdominal/pelvic viscera | All organs (hormonal, systemic) |
| Preganglionic fiber length | Short | Long (travels to abdomen) | Very long (travels to adrenal gland) |
| Postganglionic fiber length | Long | Long | None (directly into blood) |
Memory Aid
Think of it in terms of where the preganglionic fiber stops:
- Stops at the chain = Pathway 1 (paravertebral) → postganglionic goes to body wall, skin, head/neck
- Passes through chain, stops at prevertebral ganglion = Pathway 2 → postganglionic goes to gut/viscera
- Passes through chain AND prevertebral ganglion, stops at adrenal medulla = Pathway 3 → hormonal (systemic)
The further the preganglionic travels without synapsing, the more systemic the effect.
Sources:
- Medical Physiology (Boron & Boulpaep) - Chapter 14
- Costanzo Physiology, 7th Edition - Chapter 2
- Gray's Anatomy for Students - Chapter 4 (Splanchnic Nerves & Prevertebral Ganglia)
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Neuropharmacology section
- Guyton and Hall Textbook of Medical Physiology - Chapter 61
Effect of sympathetic stimulation
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have all the data needed for a complete, detailed answer. Let me compile it.
Effects of Sympathetic Stimulation
The sympathetic nervous system is the body's "fight-or-flight" system. All its effects are mediated through adrenergic receptors (α1, α2, β1, β2, β3) activated by norepinephrine from postganglionic fibers, and by epinephrine + norepinephrine released from the adrenal medulla into the bloodstream.
Understanding the Receptors First
Before going organ by organ, it helps to know what each receptor type does - because the same organ can have multiple receptor types giving opposing effects depending on which is dominant:
| Receptor | G-protein | Second messenger | General effect |
|---|---|---|---|
| α1 | Gq | ↑ IP3/DAG → ↑ intracellular Ca²⁺ | Smooth muscle contraction (vasoconstriction, mydriasis, sphincter closure) |
| α2 | Gi | ↓ cAMP | Presynaptic inhibition of NE release; CNS sedation; some vasoconstriction |
| β1 | Gs | ↑ cAMP | Heart - ↑ rate, conduction, contractility |
| β2 | Gs | ↑ cAMP | Smooth muscle relaxation (bronchodilation, vasodilation, uterine relaxation); glycogenolysis |
| β3 | Gs | ↑ cAMP | Lipolysis in adipose, bladder relaxation, thermogenesis in brown fat |
Effects Organ by Organ
1. HEART
| Effect | Receptor | Mechanism |
|---|---|---|
| ↑ Heart rate (positive chronotropy) | β1 | SA node fires faster |
| ↑ Conduction velocity (positive dromotropy) | β1 | AV nodal conduction speeds up → shorter PR interval |
| ↑ Contractility (positive inotropy) | β1 | Increased Ca²⁺ entry and troponin phosphorylation |
| ↑ Automaticity | β1 | Risk of arrhythmias during sympathetic overdrive |
"Stimulation of these receptors activates adenylyl cyclase... Initiation of the cascade has positive chronotropic (increased heart rate), dromotropic (increased conduction), and inotropic (increased contractility) effects." - Morgan & Mikhail's Clinical Anesthesiology
Net cardiac effect: Increased cardiac output, increased oxygen demand on the myocardium.
2. BLOOD VESSELS
This is the most nuanced organ system because different vessels have different receptor densities:
| Vessel bed | Receptor | Effect |
|---|---|---|
| Skin, splanchnic, renal, mucosal | α1 (dominant) | Vasoconstriction → blood diverted away |
| Skeletal muscle vessels | β2 (+ α1) | Vasodilation via β2 (epinephrine); vasoconstriction via α1 (NE) |
| Coronary arteries | β2 (dominant) | Vasodilation → increased coronary perfusion |
| Cerebral vessels | Minimal innervation | Little direct effect |
| Pulmonary vessels | α1 | Mild vasoconstriction |
The most important cardiovascular effect of α1 stimulation is vasoconstriction, which increases peripheral vascular resistance, left ventricular afterload, and arterial blood pressure. - Morgan & Mikhail
Net vascular effect: Blood pressure rises; blood is redistributed from gut/skin/kidneys to skeletal muscles and heart - perfectly designed for physical exertion.
3. LUNGS / BRONCHI
| Effect | Receptor | Mechanism |
|---|---|---|
| Bronchodilation | β2 | Relaxation of bronchial smooth muscle → airway widens |
| Decreased mucus secretion | α1 | Reduced glandular secretion |
| Vasoconstriction of pulmonary vessels | α1 | Mild effect |
Net pulmonary effect: Wider airways, more air into lungs during fight-or-flight. This is why β2 agonists (salbutamol) are used in asthma.
4. EYE
| Effect | Receptor | Mechanism |
|---|---|---|
| Mydriasis (pupil dilation) | α1 | Contraction of radial (dilator) muscle of iris |
| Relaxation of ciliary muscle | β | Slight flattening of lens → far vision adjustment |
Net ocular effect: Wide pupils for better visual field and distance vision - useful for spotting threats.
"α1-agonists are associated with mydriasis (pupillary dilation due to contraction of the radial eye muscles)." - Morgan & Mikhail
5. GASTROINTESTINAL TRACT
| Effect | Receptor | Mechanism |
|---|---|---|
| ↓ Motility / peristalsis | α2, β2 | Relaxation of gut wall smooth muscle |
| Sphincter contraction (pylorus, ileocecal, internal anal) | α1 | Contraction of sphincter smooth muscle |
| ↓ Secretions (gastric acid, intestinal juice) | α2 | Reduced glandular activity |
| ↑ Salivary secretion | β1 | Thick, viscous saliva (unlike watery parasympathetic saliva) |
Net GI effect: GI activity is essentially shut down during sympathetic activation - digestion is a low priority during stress. Blood is rerouted away from the gut.
6. LIVER
| Effect | Receptor | Mechanism |
|---|---|---|
| Glycogenolysis | α1, β2 | Breakdown of glycogen → glucose released into blood |
| Gluconeogenesis | β2 | New glucose synthesis from amino acids/lactate |
Net hepatic effect: Blood glucose rapidly rises, providing fuel for muscles and brain during emergency.
7. PANCREAS
| Effect | Receptor | Mechanism |
|---|---|---|
| ↓ Insulin secretion | α1 (dominant) | Inhibits β-cell secretion |
| ↑ Insulin secretion | β2 | Minor opposing effect |
| ↑ Glucagon secretion | β2 | From α-cells → promotes glycogenolysis |
Net pancreatic effect: Reduced insulin + increased glucagon → hyperglycemia during stress (part of the metabolic response).
8. URINARY BLADDER
| Effect | Receptor | Mechanism |
|---|---|---|
| Detrusor muscle relaxes | β2 | Bladder wall relaxes → accommodates more urine |
| Internal urethral sphincter contracts | α1 | Prevents micturition |
Net bladder effect: Bladder fills up without urinating - "holding it in" during emergency. Clinically, α1 blockers (tamsulosin) are used in BPH to relax the sphincter and improve urine flow.
9. MALE GENITALIA
| Effect | Receptor | Mechanism |
|---|---|---|
| Ejaculation | α | Contraction of vas deferens, seminal vesicles, prostate |
(Erection is parasympathetic - "point and shoot" mnemonic: Parasympathetic = Point = erection; Sympathetic = Shoot = ejaculation)
10. UTERUS
| Effect | Receptor | Mechanism |
|---|---|---|
| Contraction | α1 | Pregnant uterus |
| Relaxation | β2 | Non-pregnant uterus; also pregnant uterus at term |
Clinically: β2 agonists (ritodrine, terbutaline) are used as tocolytics to stop premature labor.
11. SKIN
| Effect | Receptor | Mechanism |
|---|---|---|
| Sweating (thermoregulatory) | Muscarinic (cholinergic sympathetic) | Eccrine sweat glands are the exception - sympathetic but use ACh |
| Piloerection ("goosebumps") | α1 | Contraction of arrector pili muscles |
| Cutaneous vasoconstriction | α1 | Skin becomes cold and pale during fear/stress |
12. ADIPOSE TISSUE
| Effect | Receptor | Mechanism |
|---|---|---|
| Lipolysis | β1, β3 | Breakdown of triglycerides → free fatty acids released into blood |
Free fatty acids serve as additional fuel source for muscles during prolonged stress.
13. KIDNEY
| Effect | Receptor | Mechanism |
|---|---|---|
| Renin secretion ↑ | β1 | Juxtaglomerular cells release renin → activates RAAS → ↑ angiotensin II → ↑ BP and aldosterone |
| Renal vasoconstriction | α1 | ↓ renal blood flow |
14. ADRENAL MEDULLA
| Effect | Receptor | Mechanism |
|---|---|---|
| Release of epinephrine (80%) + norepinephrine (20%) | Nicotinic (N) | Preganglionic ACh stimulates chromaffin cells → catecholamines poured into bloodstream |
This amplifies and sustains all sympathetic effects systemically - even in organs with sparse direct innervation.
Summary Table (Fight-or-Flight at a Glance)
| Organ | Sympathetic Effect | Receptor | Teleological Purpose |
|---|---|---|---|
| Heart rate | ↑ | β1 | Pump more blood |
| Heart contractility | ↑ | β1 | Stronger contractions |
| AV conduction | ↑ | β1 | Faster electrical conduction |
| Coronary vessels | Dilate | β2 | Feed the heart |
| Skin/gut/renal vessels | Constrict | α1 | Redirect blood to muscles |
| Skeletal muscle vessels | Dilate | β2 | More blood to working muscles |
| Blood pressure | ↑ | α1 (↑ SVR) + β1 (↑ CO) | Perfuse vital organs |
| Bronchi | Dilate | β2 | More O2 in |
| Pupils | Dilate (mydriasis) | α1 | Better vision |
| GI motility | ↓ | α2, β2 | Not needed now |
| GI sphincters | Contract | α1 | Close off GI |
| Liver | Glycogenolysis + gluconeogenesis | α1, β2 | Raise blood glucose |
| Pancreas | ↓ Insulin, ↑ glucagon | α1, β2 | Maintain high blood glucose |
| Bladder wall | Relax | β2 | Fill, don't void |
| Bladder sphincter | Contract | α1 | Don't void |
| Ejaculation | Triggered | α | Reproductive function |
| Sweat glands | Secrete (thermal) | M (cholinergic) | Thermoregulation |
| Piloerection | ↑ | α1 | Appear larger (vestigial) |
| Adipose | Lipolysis | β1, β3 | Release fuel |
| Kidney | ↑ Renin | β1 | Raise BP via RAAS |
| Adrenal medulla | ↑ Epi + NE release | Nicotinic | Systemic amplification |
The "Alarm/Stress" (Mass Sympathetic Discharge) Response
When the hypothalamus is activated by fright, extreme pain, or rage, the entire sympathetic system discharges simultaneously. Guyton lists the net body effects:
- Increased arterial pressure
- Increased blood flow to active muscles, decreased flow to gut/kidneys
- Increased cellular metabolic rate throughout the body
- Increased blood glucose
- Increased glycolysis in liver and muscle
- Increased muscle strength
- Increased mental activity
- Increased rate of blood coagulation
"The sum of these effects permits a person to perform far more strenuous physical activity than would otherwise be possible." - Guyton and Hall Textbook of Medical Physiology
Sources:
- Costanzo Physiology, 7th Edition - Table 2.3
- Morgan & Mikhail's Clinical Anesthesiology, 7th Edition - Chapter 14, Adrenoceptor Physiology
- Guyton and Hall Textbook of Medical Physiology - Chapter 61
- Medical Physiology (Boron & Boulpaep) - Chapter 14
Explain the molecular mechanism of cAMP and IP3 signaling
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have all necessary content and diagrams. Let me compile a thorough, well-illustrated explanation.
Molecular Mechanisms of cAMP and IP3 Signaling
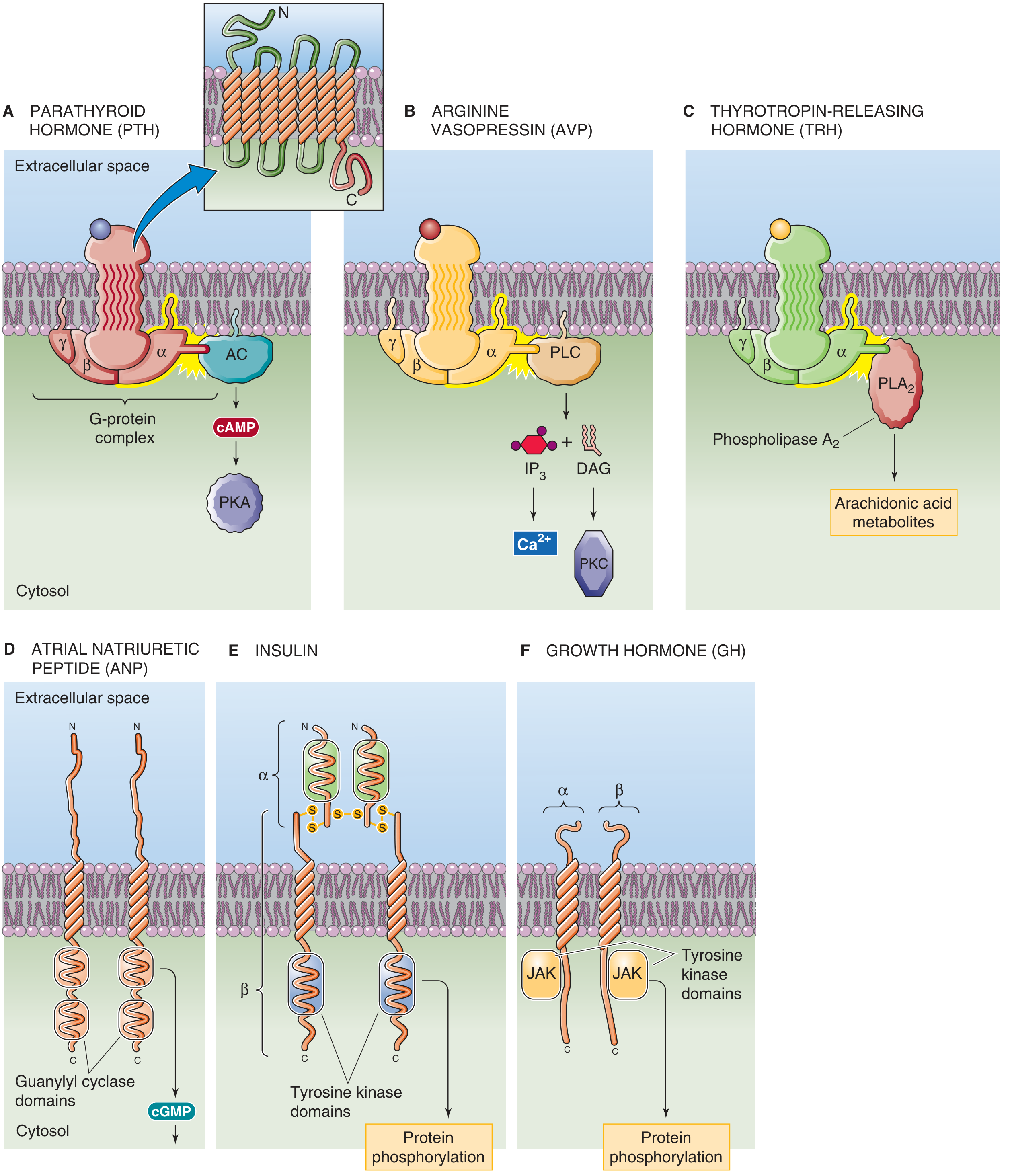
Both pathways are activated by G protein-coupled receptors (GPCRs) - the most abundant class of membrane receptors in the human body. The critical difference is which G protein subtype is activated:
| Pathway | G protein | Enzyme activated | Second messengers |
|---|---|---|---|
| cAMP pathway | Gs (stimulatory) | Adenylyl cyclase | cAMP |
| IP3/DAG pathway | Gq | Phospholipase C (PLC) | IP3 + DAG |
| Inhibitory cAMP | Gi (inhibitory) | Adenylyl cyclase (inhibited) | ↓ cAMP |
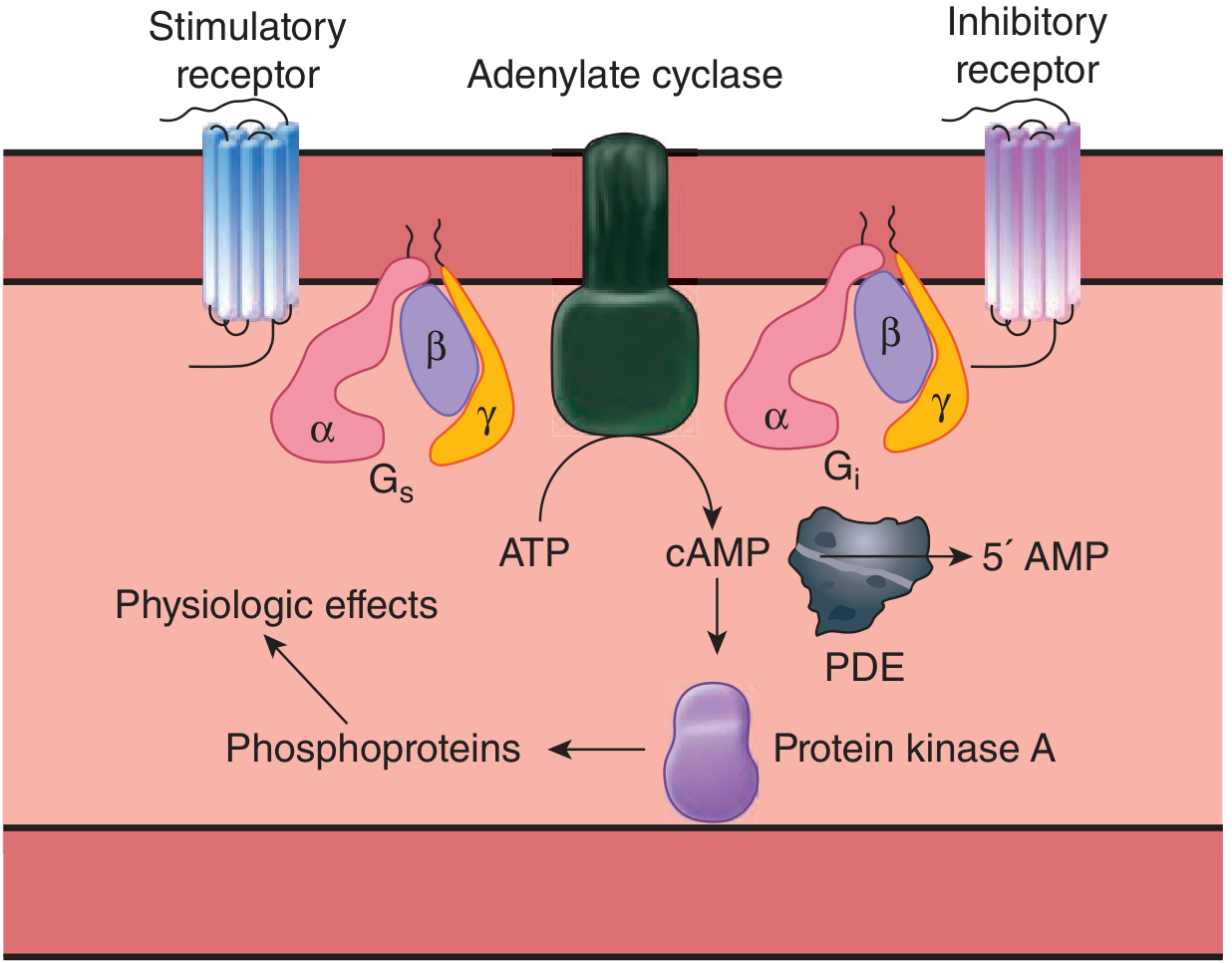
PART 1: The cAMP Signaling Pathway
Overview
Step-by-Step Molecular Cascade
Step 1: Ligand Binds to GPCR
An agonist (e.g., norepinephrine at β1 receptor, glucagon at its receptor, PTH, ADH at V2, adrenaline at β2) binds to a 7-transmembrane GPCR on the cell surface. This causes a conformational change in the receptor's intracellular domain.
Step 2: G Protein Activation (GDP → GTP exchange)
The receptor's conformational change exposes a binding site for the heterotrimeric G protein (Gs), which is made of three subunits: α, β, and γ.
- At rest: the αs subunit holds GDP and is inactive, associated with βγ
- Upon receptor activation: the receptor acts as a guanine nucleotide exchange factor (GEF) - it causes GDP to be replaced by GTP on the αs subunit
- GTP binding causes the αs subunit to dissociate from βγ and become active
Step 3: Activation of Adenylyl Cyclase
The free, active Gs-α-GTP subunit diffuses laterally in the membrane and binds to and activates adenylyl cyclase (also called adenylate cyclase), a 12-transmembrane domain enzyme on the inner leaflet of the plasma membrane. There are 10 isoforms of adenylyl cyclase, each with slightly different regulatory properties.
"Adenylyl cyclase is a membrane-bound protein with 12 transmembrane regions. Ten isoforms of this enzyme have been described and each can have distinct regulatory properties, permitting the cAMP pathway to be customized to specific tissue needs." - Ganong's Review of Medical Physiology
Step 4: ATP → cAMP (The Chemistry)
Adenylyl cyclase catalyzes the cyclization of ATP to cyclic AMP (3',5'-cyclic adenosine monophosphate, cAMP) with release of pyrophosphate (PPi).
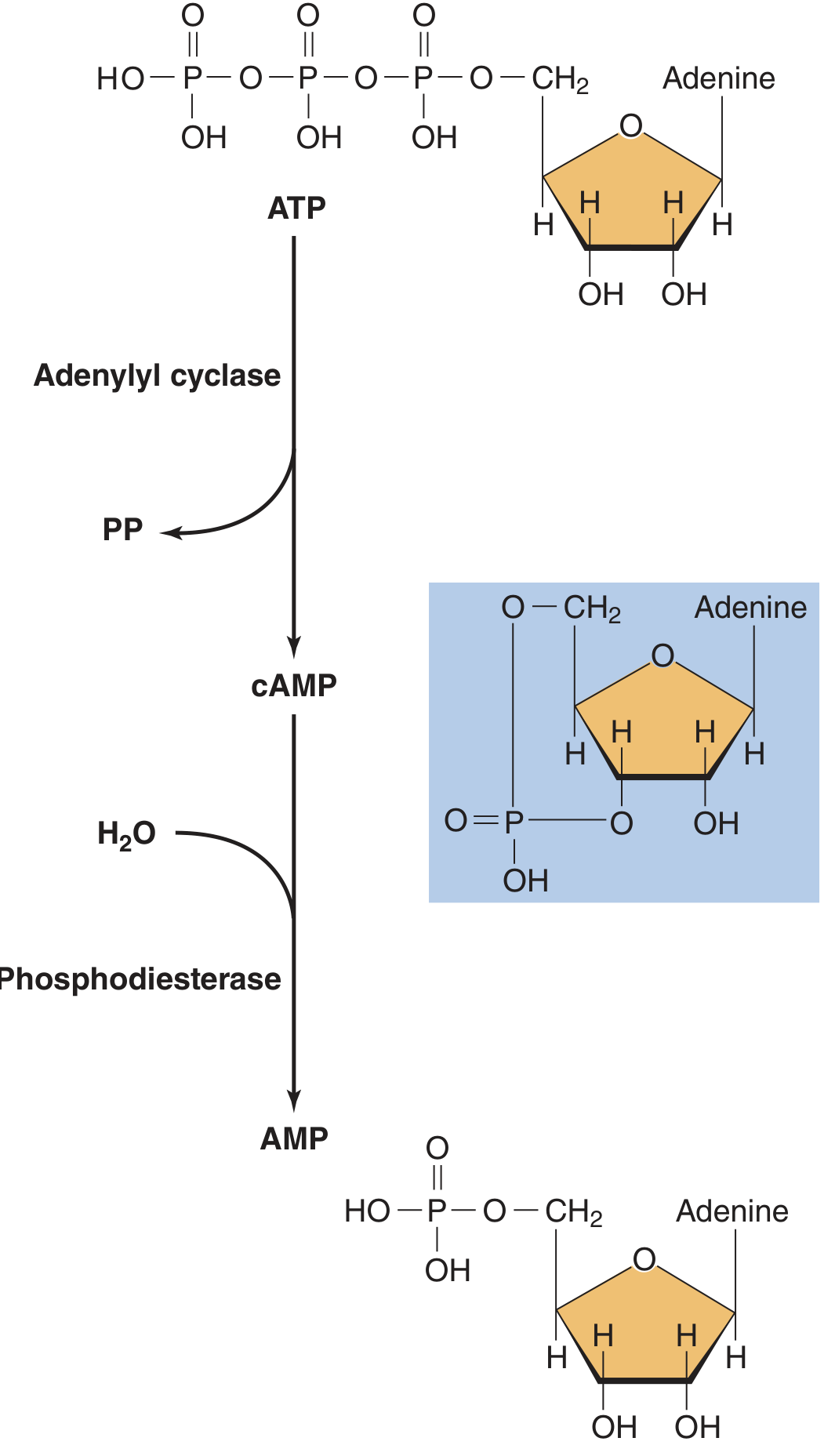
The key structural change: the phosphate group forms a cyclic ring bridging the 3' and 5' carbons of the ribose sugar - hence "cyclic" AMP.
Step 5: cAMP Activates Protein Kinase A (PKA)
cAMP acts as the "second messenger" by binding to the regulatory (R) subunits of Protein Kinase A (PKA), which is a tetramer: 2 regulatory (R) subunits + 2 catalytic (C) subunits.
- At rest: the R subunits hold the C subunits inactive
- cAMP binds to the R subunits → conformational change → R subunits release the C subunits
- The free catalytic subunits are now active kinases
Step 6: Substrate Phosphorylation
Active PKA catalytic subunits phosphorylate serine and threonine residues on dozens of target proteins, altering their activity (either activating or inhibiting depending on the substrate):
Cytoplasmic targets:
- Phosphorylase kinase → activated → activates glycogen phosphorylase → glycogenolysis
- Hormone-sensitive lipase → activated → lipolysis (fat breakdown)
- L-type Ca²⁺ channels → phosphorylated → increased Ca²⁺ entry → ↑ cardiac contractility
- Troponin I → phosphorylated → faster Ca²⁺ dissociation → faster cardiac relaxation (lusitropy)
Nuclear target (CREB):
The free catalytic subunit translocates into the nucleus and phosphorylates CREB (cAMP Response Element-Binding Protein):
"The active catalytic subunit of PKA moves to the nucleus and phosphorylates the cAMP-responsive element-binding protein (CREB). This transcription factor then binds to DNA and alters transcription of a number of genes." - Ganong's Review of Medical Physiology
This allows cAMP signaling to produce long-term gene expression changes - not just acute enzyme activation.
Step 7: Signal Termination
The cAMP signal is terminated by two mechanisms:
- Phosphodiesterase (PDE) hydrolyzes cAMP → 5'-AMP (inactive). PDEs are the "off switch." Drugs that inhibit PDEs (caffeine, theophylline, sildenafil, milrinone) prolong cAMP signaling.
- Phosphoprotein phosphatases dephosphorylate the PKA substrates, reversing their activation.
- The Gα-GTP is self-terminating: intrinsic GTPase activity on the αs subunit hydrolyzes GTP → GDP, returning it to the inactive state.
Inhibitory cAMP Pathway (Gi)
When an agonist binds to an inhibitory receptor (e.g., α2 adrenergic, muscarinic M2, opioid receptors, adenosine A1):
- The receptor couples to Gi (inhibitory G protein)
- Gi-α-GTP inhibits adenylyl cyclase → less cAMP produced
- Result: decreased PKA activity → opposite effects (e.g., decreased heart rate via M2 receptors)
cAMP Pathway Summary Diagram
Agonist (NE, Glucagon, PTH, ADH-V2, Epinephrine-β)
↓
GPCR (7-TM receptor)
↓ GDP → GTP exchange
Gs-α-GTP dissociates
↓
Adenylyl Cyclase ACTIVATED
↓ ATP → cAMP + PPi
cAMP ↑
↓ binds regulatory (R) subunits
PKA (C subunits freed)
↓
Serine/Threonine phosphorylation of substrates
├── Cytoplasm: Enzymes activated/inhibited
│ (glycogenolysis, lipolysis, cardiac effects)
└── Nucleus: CREB phosphorylated → gene transcription
TERMINATION:
PDE: cAMP → 5'-AMP
GTPase: Gα-GTP → Gα-GDP (self-terminating)
PART 2: The IP3/DAG (Phosphoinositide) Signaling Pathway
This pathway uses two second messengers from a single cleavage event - like splitting one molecule into two functional signals.
Overview
Step-by-Step Molecular Cascade
Step 1: Ligand Binds to Gq-Coupled GPCR
Agonists that activate this pathway include:
- α1 adrenergic (norepinephrine/epinephrine)
- M1, M3 muscarinic (acetylcholine)
- Angiotensin II (AT1)
- Vasopressin (V1)
- Histamine (H1)
- Endothelin, Substance P, TRH
Step 2: Gq Activation
The receptor couples to Gq protein. Like Gs, Gq is a heterotrimeric αβγ protein. Receptor binding triggers GDP → GTP exchange on the Gαq subunit, which dissociates and becomes active.
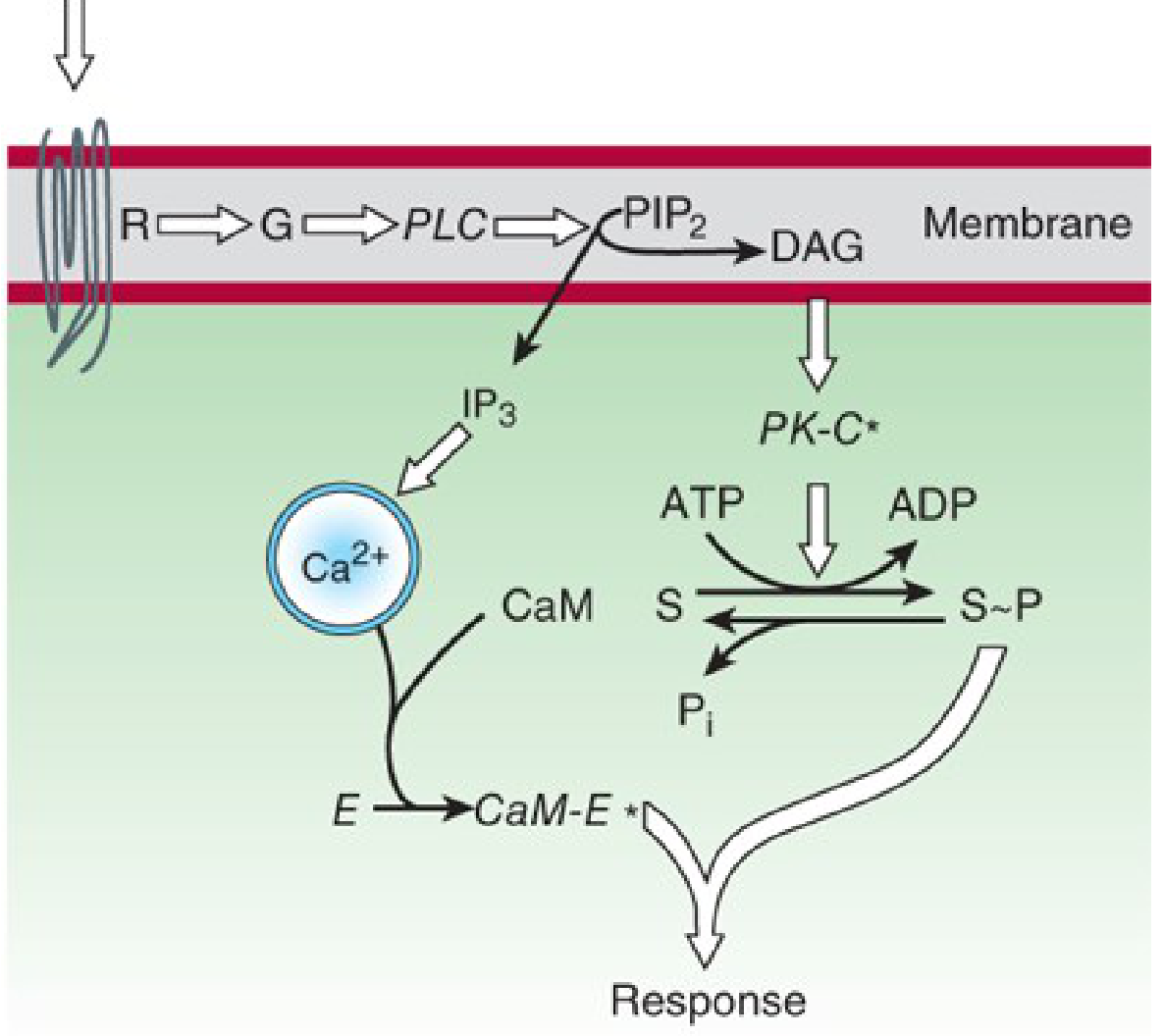
"Binding of the appropriate peptide hormone (e.g., AVP) to its receptor initiates the following cascade: (1) activation of Gαq; (2) activation of a membrane-bound phospholipase C (PLC); and (3) cleavage of PIP2 by this PLC, with the generation of IP3 and DAG." - Medical Physiology (Boron & Boulpaep)
Step 3: Activation of Phospholipase C (PLC-β)
The free Gαq-GTP binds to and activates phospholipase C-β (PLC-β), a membrane-associated enzyme.
Step 4: Hydrolysis of PIP2
PLC-β cleaves PIP2 (phosphatidylinositol-4,5-bisphosphate) - a minor phospholipid found in the inner leaflet of the plasma membrane - into two second messengers:
PIP2 ──PLC-β──→ IP3 + DAG
(membrane lipid) (water- (membrane-
soluble) bound)
"The crucial step is stimulation of a membrane enzyme, phospholipase C (PLC), which splits... phosphatidylinositol-4,5-bisphosphate (PIP2) into two second messengers, diacylglycerol (DAG) and inositol-1,4,5-trisphosphate (IP3)." - Katzung's Basic and Clinical Pharmacology
The IP3 Branch: Calcium Release
Step 5a: IP3 Diffuses to the ER
IP3 is water-soluble and diffuses through the cytoplasm to the endoplasmic reticulum (ER).
Step 6a: IP3 Binds to IP3 Receptor (IP3R)
IP3 binds to the IP3 receptor (IP3R), a ligand-gated Ca²⁺ channel on the ER membrane. This causes the channel to open, releasing Ca²⁺ from ER stores into the cytoplasm.
- Cytoplasmic [Ca²⁺] rises from ~100 nM (resting) to ~1 μM (activated) - a 10-fold increase
Step 7a: Biphasic Calcium Response
Two phases of Ca²⁺ rise occur:
- Phase 1 (IP3-mediated): Ca²⁺ released from ER stores → rapid, transient spike
- Phase 2 (store-operated): Depletion of ER Ca²⁺ activates SOCE (Store-Operated Ca²⁺ Entry) via STIM1/Orai1 channels in the plasma membrane → sustained Ca²⁺ influx from outside
Step 8a: Ca²⁺ Activates Calmodulin (CaM)
Elevated cytoplasmic Ca²⁺ binds to calmodulin, a small, ubiquitous Ca²⁺-sensing protein with 4 EF-hand Ca²⁺-binding sites.
Ca²⁺-calmodulin (Ca²⁺-CaM) complex then activates:
| Ca²⁺-CaM Target | Effect |
|---|---|
| CaM kinase II (CaMKII) | Phosphorylates synaptic proteins, synapsin → neurotransmitter release |
| Myosin light chain kinase (MLCK) | Phosphorylates myosin → smooth muscle contraction |
| Calcineurin (phosphatase) | Dephosphorylates NFAT → gene transcription (immune response) |
| Phosphodiesterase (PDE1) | Degrades cAMP - cross-talk between pathways |
| NOS (Nitric oxide synthase) | Produces NO → vasodilation |
The DAG Branch: Protein Kinase C
Step 5b: DAG Stays in the Membrane
DAG (diacylglycerol) is lipid-soluble and remains anchored in the inner leaflet of the plasma membrane, where it acts as a docking platform.
Step 6b: PKC Activation
DAG recruits and activates Protein Kinase C (PKC) - a family of at least 10 isoforms, requiring:
- DAG (membrane anchor/allosteric activator)
- Ca²⁺ (for classical PKC isoforms - α, β, γ)
- Phosphatidylserine (membrane phospholipid cofactor)
PKC translocates from cytoplasm to the plasma membrane, where DAG and Ca²⁺ lock it in the active conformation.
Step 7b: PKC Phosphorylates Target Proteins
PKC is a serine/threonine kinase that phosphorylates a broad range of substrates:
| PKC Target | Physiological Effect |
|---|---|
| Smooth muscle proteins | Contraction (vasoconstriction, sphincter closure) |
| Transcription factors (AP-1, NF-κB) | Gene expression (inflammation, growth) |
| Receptor tyrosine kinases | Receptor downregulation (negative feedback) |
| Ion channels | Altered membrane excitability |
| Enzymes (e.g., PLA2) | Arachidonic acid release → prostaglandins |
"DAG is confined to the membrane, where it activates a phospholipid- and calcium-sensitive protein kinase called protein kinase C." - Katzung
IP3/DAG Pathway Summary
Agonist (NE-α1, ACh-M1/M3, Ang II, Histamine-H1)
↓
GPCR → Gq activation (GDP → GTP)
↓
PLC-β activated
↓
PIP2 (in membrane) ─────────────────────→ cleaved into:
IP3 DAG
(water-soluble) (membrane-bound)
↓ ↓
Binds IP3R on ER Recruits + activates PKC
↓ ↓
Ca²⁺ released Phosphorylates proteins
from ER stores (smooth muscle contraction,
↓ gene expression, etc.)
↑ cytoplasmic Ca²⁺
↓
Binds Calmodulin (CaM)
↓
Ca²⁺-CaM activates:
- CaMKII → synaptic release, LTP
- MLCK → smooth muscle contraction
- Calcineurin → NFAT → gene transcription
- NOS → NO → vasodilation
PART 3: Cross-talk and Integration
These two pathways are not isolated - they interact with each other:
| Interaction | Mechanism |
|---|---|
| Ca²⁺ activates Ca²⁺-dependent PDE | Degrades cAMP → can inhibit cAMP pathway |
| PKC phosphorylates Gi protein | Reduces cAMP inhibition → potentiates cAMP |
| PKA phosphorylates IP3R | Sensitizes ER to IP3 → amplifies Ca²⁺ release |
| Ca²⁺-CaM activates adenylyl cyclase types I and VIII | Stimulates cAMP production |
This cross-talk allows cells to fine-tune their responses with great precision.
Quick Comparison: cAMP vs IP3/DAG
| Feature | cAMP Pathway | IP3/DAG Pathway |
|---|---|---|
| G protein | Gs (stimulate) / Gi (inhibit) | Gq |
| Effector enzyme | Adenylyl cyclase | Phospholipase C-β |
| Substrate cleaved | ATP | PIP2 |
| Second messengers | cAMP | IP3 + DAG |
| Location of 2nd messenger | Cytoplasm (soluble) | IP3 = cytoplasm; DAG = membrane |
| Downstream kinase | PKA | PKC |
| Ca²⁺ role | Indirect (via MLCK in some) | Direct (IP3 releases Ca²⁺ from ER) |
| Nuclear effects | CREB phosphorylation → gene expression | NFAT, AP-1, NF-κB activation |
| Terminated by | PDE (cAMP→AMP); phosphatases | Ca²⁺-ATPase pumps Ca²⁺ back; PKC internalization |
| Physiological example | β1: ↑ heart rate; Glucagon: glycogenolysis | α1: vasoconstriction; M3: gland secretion |
| Drug example that enhances it | Caffeine/theophylline (PDE inhibitors) | Phorbol esters (DAG mimic, activate PKC) |
Sources:
- Medical Physiology (Boron & Boulpaep) - Chapter 47, Endocrinology
- Katzung's Basic and Clinical Pharmacology, 16th Edition - Chapter 2
- Ganong's Review of Medical Physiology, 26th Edition - Chapter 2
- Lippincott Illustrated Reviews: Biochemistry, 8th Edition - Chapter 23
- Morgan & Mikhail's Clinical Anesthesiology, 7th Edition - Chapter 14
This is a shared conversation. Sign in to Orris to start your own chat.