“Massive transfusion protocol“ from emergency medicine with detailed and stepwise explanation including viva based questions !
Reading File
Finding Sources
Finding Sources
Searching PubMed
"massive transfusion protocol" emergency
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile a thorough, detailed answer.
Massive Transfusion Protocol (MTP) - Emergency Medicine
The Denver Health MTP Flowchart (Schwartz's Surgery)
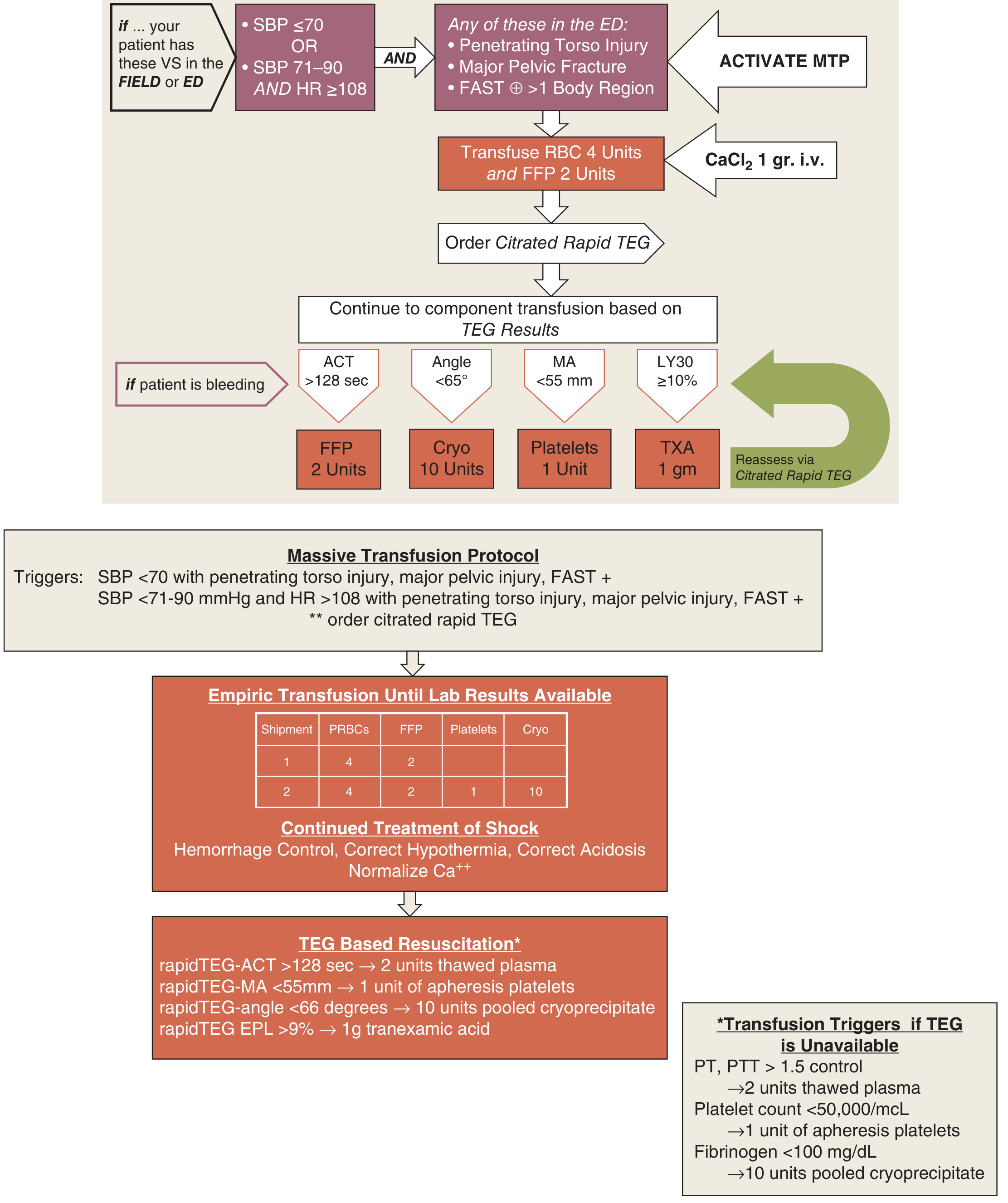
Figure: Denver Health Medical Center MTP - triggers, empiric blood product ratios, TEG-based reassessment (Schwartz's Principles of Surgery, 11th ed.)
1. DEFINITION
Massive transfusion has three accepted definitions (all in clinical use):
| Definition | Threshold |
|---|---|
| Classic (24-hour) | Replacement of >10 units of PRBCs within 24 hours (equivalent to ~1 blood volume in an adult) |
| Rate-based | Ongoing blood loss of >150 mL/min |
| Time-compressed | Transfusion of ≥3 units PRBCs within 1 hour, or 4 blood components within 30 minutes |
The classic definition is being replaced in clinical practice by the rate-based and time-compressed definitions because they are more actionable and do not require waiting 24 hours.
Mortality correlation (Rosen's Emergency Medicine):
- <5 units transfused: ~10% mortality
- 6-9 units: ~20% mortality
- ≥10 units: >50% mortality
2. PATHOPHYSIOLOGY - "THE LETHAL TRIAD"
Massive hemorrhage triggers a self-reinforcing cycle of three interconnected abnormalities:
ACIDOSIS ←――――――――――――――――――――→ HYPOTHERMIA
↘ ↙
――――→ COAGULOPATHY ←――――――
a) Hypothermia
- Hemorrhagic shock impairs perfusion and metabolic heat production
- Cold PRBCs and room-temperature crystalloids exacerbate this
- Temperatures <34°C aggravate coagulopathy and provoke myocardial irritability
- Clotting factor enzymatic activity falls significantly below 35°C
b) Acidosis
- Anaerobic metabolism from poor perfusion generates lactic acid
- Base deficit > -6 mEq/L = 72% chance of requiring transfusion
- Base deficit < -6 mEq/L = only 18% chance of requiring PRBCs
- Acidosis impairs thrombin generation and platelet function
c) Coagulopathy (Trauma-Induced Coagulopathy, TIC)
Multifactorial - caused by:
- Dilution - crystalloid/PRBC resuscitation without clotting factors
- Consumption - factor consumption from tissue trauma, DIC
- Dysfunction - hypothermia and acidosis inhibit enzyme activity
- Fibrinolysis - systemic activation of plasmin
After transfusion of 2 blood volumes, only ~10% of original coagulation elements remain (Roberts & Hedges' Clinical Procedures in Emergency Medicine).
3. TRIGGERS FOR MTP ACTIVATION
Clinical Prediction Tools
ABC Score (Assessment of Blood Consumption) - most widely validated, bedside tool:
| Parameter | Points |
|---|---|
| Penetrating mechanism of injury | 1 |
| SBP <90 mmHg | 1 |
| HR >120 bpm | 1 |
| Positive FAST exam | 1 |
- Score ≥2 = Activate MTP
- Sensitivity 75%, Specificity 86% for predicting massive transfusion
- <5% of patients who will require massive transfusion are missed
- 85% of major trauma patients correctly identified
(Barash Clinical Anesthesia 9e; Schwartz's Surgery 11e)
Additional triggers (Rosen's Emergency Medicine):
- Elevated INR + base deficit, even without meeting the classic 10-unit threshold
- Alternative: transfusion of 3 units PRBCs in 1 hour or 4 components in 30 minutes
Other scoring systems (Sabiston Surgery):
- Shock Index (SI) = HR ÷ SBP (normal <1.0; >1.0 suggests hemodynamic compromise)
- Modified SI (MSI) = HR ÷ MAP (better than SI for stroke volume and SVR assessment)
- ALERT score - accounts for prehospital + admission variables (SBP, DBP, HR, RR, SpO2, motor GCS, penetrating mechanism, FAST)
4. STEPWISE MANAGEMENT
Step 1 - Immediate Actions on MTP Activation
- Call the blood bank immediately - alert for ongoing product demand
- Establish large-bore IV access (2 x 16G or larger, or IO)
- Draw blood samples early - type & crossmatch, CBC, PT/INR, aPTT, fibrinogen, TEG/ROTEM, metabolic panel, ABG
- Critical: once the patient has received ~1 blood volume of transfused products, new specimens will contain donor blood and confuse crossmatching
- Administer calcium - CaCl₂ 1 g IV at MTP activation (citrate chelates calcium)
- Begin warming - blood warmers for all products, warming blankets, warmed IV fluids, maintain ambient OR temperature
Step 2 - Empiric Blood Product Resuscitation (Damage Control Resuscitation)
The 1:1:1 Ratio (PRBCs : FFP : Platelets) is the current standard:
"We recommend a 1:1:1 ratio of blood products when a MTP is initiated." - Rosen's Emergency Medicine
The PROPPR trial (multicenter RCT, the landmark study) compared 1:1:1 vs. 2:1:1 ratios and found:
- No difference in 24-hour or 30-day mortality overall
- Fewer patients in the 1:1:1 group died of exsanguination at 24 hours
- More patients in the 1:1:1 group achieved hemostasis
Empiric shipment example (Denver Health MTP):
| Shipment | PRBCs | FFP | Platelets | Cryo |
|---|---|---|---|---|
| Pack 1 | 4 units | 2 units | - | - |
| Pack 2 | 4 units | 2 units | 1 unit | 10 units |
Rationale for components:
| Component | Dose | Key Points |
|---|---|---|
| PRBCs | 1 unit/10 kg | Give O-negative (females of childbearing age) or O-positive (others) when type unknown. Each unit raises Hgb ~1 g/dL |
| FFP (Fresh Frozen Plasma) | 15 mL/kg (~4 units in 70 kg adult) | Contains all clotting factors. Each unit raises factor levels 2-3%. Cannot achieve INR <1.5 with FFP alone. Thaw time 45-60 min (use pre-thawed if available) |
| Platelets | 1 apheresis unit or 6-pack | Each unit raises platelet count 5,000-10,000; a 6-pack raises by 30,000-60,000 |
| Cryoprecipitate | 10-20 bags | Give when fibrinogen <100 mg/dL; contains fibrinogen, Factor VIII, vWF, XIII |
Step 3 - Adjuncts: Tranexamic Acid (TXA)
- Dose: 1 g IV over 10 minutes, followed by 1 g IV over 8 hours
- Window: Must be given within 3 hours of injury (CRASH-2 trial; benefit lost and possible harm after 3 hours)
- Mechanism: Antifibrinolytic - inhibits plasminogen activation, prevents premature clot lysis
- Included in most MTPs; in TEG-guided MTP, TXA is triggered when LY30 ≥10% (indicating fibrinolysis)
Step 4 - TEG/ROTEM-Guided Goal-Directed Therapy
Once rapid TEG or ROTEM results are available, shift from empiric 1:1:1 to targeted therapy:
| TEG Parameter | Abnormality | Product Given |
|---|---|---|
| ACT (Activated Clotting Time) | >128 seconds | FFP 2 units |
| Angle | <65° | Cryoprecipitate 10 units (fibrinogen deficiency) |
| MA (Maximum Amplitude) | <55 mm | Platelets 1 apheresis unit |
| LY30 (Lysis at 30 min) | ≥10% | TXA 1 g IV |
If TEG/ROTEM is unavailable, use conventional triggers:
- PT or aPTT >1.5x control → FFP 2 units
- Platelet count <50,000/µL → platelets
- Fibrinogen <100 mg/dL → cryoprecipitate 10 units
(Schwartz's Surgery, 11th Ed.; Barash Clinical Anesthesia 9e)
Step 5 - Concurrent Hemorrhage Control
MTP is a bridge - definitive management requires source control:
- Permissive hypotension (target SBP 80-90 mmHg in trauma, NOT in TBI) until hemorrhage control is achieved
- Surgical hemorrhage control / damage control surgery
- REBOA (Resuscitative Endovascular Balloon Occlusion of the Aorta) for pelvic/junctional hemorrhage
- Interventional radiology embolization for non-compressible hemorrhage
- Pelvic binder for pelvic fractures
Step 6 - Termination / Transition
- MTP is de-escalated when hemostasis is achieved
- Transition to TEG/ROTEM-guided targeted replacement
- Monitor for complications (see below)
5. WHOLE BLOOD RESUSCITATION (Emerging Evidence)
- Whole blood (1 unit = ~500 mL) contains RBCs, plasma, and platelets in their natural ratio
- Avoids the "storage lesion" seen in individual components
- Some centers now use whole blood when ABC score ≥2
- A 2024 meta-analysis and EAST practice guideline (PMID: 38531812) examined this evidence - showing survival benefits in injured patients requiring transfusion
6. COMPLICATIONS OF MASSIVE TRANSFUSION
Metabolic Complications
| Complication | Mechanism | Management |
|---|---|---|
| Hypocalcemia | Citrate (preservative) chelates ionized calcium | CaCl₂ 1 g IV; monitor iCa |
| Hyperkalemia | K⁺ leaks from stored RBCs (especially old blood) | Monitor; treat if symptomatic |
| Hypomagnesemia | Dilutional | Replace Mg²⁺ |
| Metabolic alkalosis | Citrate converted to bicarbonate by liver | Usually self-resolves |
| Hypothermia | Cold blood products + vasoconstriction | Blood warmers, active external warming |
Hematologic Complications
| Complication | Details |
|---|---|
| Dilutional thrombocytopenia | >5 units PRBCs mandates platelet count check |
| DIC | Consumption of factors + platelets + fibrinogen; elevated PT, aPTT, D-dimers; low fibrinogen |
| Coagulopathy | Multifactorial (dilution + hypothermia + acidosis) |
Immunologic and Organ Complications
| Complication | Key Features |
|---|---|
| TRALI (Transfusion-Related Acute Lung Injury) | Non-cardiogenic pulmonary edema within 6 hours; anti-HLA antibodies in donor plasma; most common cause of transfusion-related death |
| TACO (Transfusion-Associated Circulatory Overload) | Cardiogenic pulmonary edema; high BNP; treated with diuresis |
| Febrile Non-Hemolytic Reaction (FNHTR) | Temp rise ≥1°C; cytokines from stored leukocytes; treat with paracetamol, discard unit |
| Acute Hemolytic Reaction | ABO incompatibility; fever, flank pain, hemoglobinuria; stop transfusion immediately, IV fluids |
| Transfusion-Associated GVHD | Donor T-lymphocytes attack recipient; use irradiated blood in immunocompromised patients |
| Multi-organ dysfunction | ARDS, AKI, hepatic dysfunction from prolonged shock + inflammatory cascade |
7. SPECIAL POPULATIONS
- Pediatric: Massive transfusion = >0.5 blood volumes in 24h; blood volume = 80 mL/kg; use 1:1:1 ratio
- Obstetric (PPH): Uterotonic agents + MTP; fibrinogen often drops early; cryoprecipitate or fibrinogen concentrate critical
- Hepatic disease (variceal bleeding): Coagulopathy pre-exists; use FFP + platelets + recombinant Factor VIIa as salvage
- Anticoagulated patients: Add 4-factor PCC + Vitamin K 10 mg IV slow infusion for warfarin; andexanet alfa for Factor Xa inhibitors
8. VIVA QUESTIONS AND ANSWERS
Q1. Define massive transfusion. What are the three accepted definitions?
A. Massive transfusion is traditionally defined as replacement of >10 units PRBCs within 24 hours (one blood volume). Two more practical definitions are: ongoing blood loss at >150 mL/min, and transfusion of ≥3 units PRBCs in 1 hour or 4 blood components in 30 minutes. The time-compressed definitions allow earlier MTP activation.
Q2. What is the ABC score and what are its parameters?
A. The Assessment of Blood Consumption score uses four immediately available, non-laboratory variables: (1) penetrating mechanism of injury, (2) SBP <90 mmHg, (3) HR >120 bpm, and (4) positive FAST. Score ≥2 triggers MTP activation. It is 75% sensitive, 86% specific.
Q3. What is the optimal blood product ratio in MTP? What trial evidence supports this?
A. The recommended ratio is 1:1:1 (PRBCs:FFP:Platelets). The PROPPR trial (multicenter RCT) compared 1:1:1 vs. 2:1:1 and found no difference in 24-hour or 30-day mortality overall, but fewer deaths from exsanguination at 24 hours in the 1:1:1 group. More patients also achieved hemostasis in the 1:1:1 group.
Q4. What is the "lethal triad" in massive hemorrhage?
A. The lethal triad is hypothermia + acidosis + coagulopathy, each element worsening the others in a vicious cycle. Prevention requires blood warmers, minimizing crystalloids, early balanced resuscitation, and damage control surgery.
Q5. What is Damage Control Resuscitation (DCR)? How does it differ from traditional resuscitation?
A. DCR has three principles: (1) permissive hypotension (target SBP 80-90 mmHg to avoid clot disruption before surgical hemorrhage control; contraindicated in TBI), (2) hemostatic resuscitation (1:1:1 ratio replacing blood volume, not crystalloids), and (3) early definitive hemorrhage control rather than protracted resuscitation. Traditional resuscitation used large volumes of crystalloid (now shown to worsen coagulopathy, edema, and outcomes by disrupting the endothelial glycocalyx layer).
Q6. What is the role of tranexamic acid (TXA) in MTP?
A. TXA is an antifibrinolytic that inhibits plasminogen activation, preventing premature clot lysis. It is given as 1 g IV over 10 min, followed by 1 g IV over 8 hours. It must be administered within 3 hours of injury - after this window, the CRASH-2 trial showed it may actually increase mortality. In TEG-guided MTP, TXA is triggered by LY30 ≥10%.
Q7. What are the TEG parameters and what does each indicate about coagulation?
A.
- R (Reaction) time / ACT - time to initial clot formation; prolonged = factor deficiency → give FFP
- Angle (α) - rate of fibrin cross-linking; low angle = low fibrinogen → give cryoprecipitate
- MA (Maximum Amplitude) - clot strength; depends on platelets and fibrin; low MA <55 mm = platelet dysfunction → give platelets
- LY30 - clot lysis at 30 minutes; ≥10% = hyperfibrinolysis → give TXA
Q8. What are the major complications of massive transfusion?
A. Three categories:
- Metabolic: Hypocalcemia (citrate chelation), hyperkalemia (RBC lysis in stored blood), hypomagnesemia, hypothermia
- Hematologic: Dilutional thrombocytopenia, DIC, coagulopathy
- Immunologic/Pulmonary: TRALI (most common cause of transfusion death - non-cardiogenic pulmonary edema within 6 hours), TACO (cardiogenic), febrile non-hemolytic reactions, acute hemolytic reaction (ABO mismatch)
Q9. Why is calcium given with MTP? What form and dose?
A. Blood products are stored with citrate as a preservative. Citrate chelates (binds) ionized calcium, causing hypocalcemia which impairs myocardial function and coagulation (calcium is required by multiple steps in the coagulation cascade). Calcium chloride 1 g IV is given at MTP activation (and may be repeated). CaCl₂ is preferred over calcium gluconate in emergency settings because it does not require hepatic conversion.
Q10. What is TRALI? How does it differ from TACO?
| Feature | TRALI | TACO |
|---|---|---|
| Mechanism | Immune-mediated (anti-HLA antibodies in donor plasma) | Volume overload, hydrostatic |
| Onset | Within 6 hours of transfusion | During or shortly after |
| BNP | Normal or mildly elevated | Markedly elevated |
| CXR | Bilateral infiltrates (non-cardiogenic) | Bilateral infiltrates (cardiogenic) |
| PCWP | Normal (<18 mmHg) | Elevated (>18 mmHg) |
| Treatment | Supportive, O₂, ventilatory support | Diuretics |
| Mortality | Higher (leading cause of transfusion-related death) | Lower |
Q11. What is the "emergency transfusion score" and what variables does it use?
A. The emergency transfusion score is a point system using: SBP, presence of free fluid on FAST, unstable pelvic ring fracture, advanced age, transport from the scene, mechanism (MVC or fall), as predictors of future transfusion requirements. It is more complex than the ABC score but may be more accurate in some settings.
Q12. What blood type is given in an emergency when the patient's type is unknown?
A. O-negative (O-) PRBCs are the universal donor for females of childbearing potential (to avoid anti-D sensitization). O-positive (O+) PRBCs can be used for males and post-menopausal females. For FFP, AB plasma is the universal donor (contains no anti-A or anti-B antibodies). Platelet compatibility is preferred but not required in emergencies.
Q13. When do you switch from empiric 1:1:1 to goal-directed therapy?
A. Once point-of-care viscoelastic testing (TEG or ROTEM) results are available. Goal-directed therapy uses TEG parameters to identify which specific component is deficient and avoids unnecessary transfusion of products that are not needed, reducing exposure to blood product complications. If TEG is unavailable, conventional thresholds (PT/aPTT >1.5x, platelets <50,000, fibrinogen <100 mg/dL) guide therapy.
Q14. What is the significance of early specimen collection in MTP?
A. Once the patient has received close to one blood volume of transfused products, new blood specimens will contain so much donor blood that it confuses further crossmatching of subsequent units. Therefore, sufficient specimens must be drawn early in the course of massive transfusion for type, screen, crossmatch, and coagulation studies.
Q15. What is the role of whole blood in modern MTP?
A. Whole blood contains all components (RBCs, plasma, platelets) in physiologic ratios and avoids the storage lesion of component therapy. Some trauma centers use cold-stored low-titer group O whole blood for initial resuscitation when ABC score ≥2. A 2024 systematic review and EAST practice guideline (PMID 38531812) supports its use in injured patients requiring transfusion. It is particularly relevant in austere environments ("walking blood banks") and prehospital settings.
Summary Mnemonic: "MTP - HALT THE BLEED"
- H - Hypocalcemia: give CaCl₂
- A - ABC score ≥2: activate MTP
- L - Lethal triad (hypothermia, acidosis, coagulopathy): prevent all three
- T - TXA within 3 hours
- T - TEG/ROTEM guided: goal-directed after empiric phase
- H - Hemostatic resuscitation: 1:1:1 ratio
- E - Early samples: type & crossmatch before volumes contaminate
- B - Blood warmers: prevent hypothermia
- L - Lethal complications: TRALI, TACO, DIC
- E - Empiric then targeted: shift from fixed ratio to individualized
- E - Early hemorrhage control: MTP is a bridge, not definitive
- D - DCR (Damage Control Resuscitation): permissive hypotension + hemostatic resus
Sources: Tintinalli's Emergency Medicine (9th ed.), Rosen's Emergency Medicine (10th ed.), Schwartz's Principles of Surgery (11th ed.), Roberts & Hedges' Clinical Procedures in Emergency Medicine, Henry's Clinical Diagnosis & Management by Laboratory Methods, Sabiston Textbook of Surgery (21st ed.), Barash Clinical Anesthesia (9th ed.), Bailey & Love's Short Practice of Surgery (28th ed.)
Recent evidence update: Whole blood resuscitation meta-analysis & EAST guideline 2024 (PMID 38531812) supports whole blood use in injured patients requiring transfusion.
This is a shared conversation. Sign in to Orris to start your own chat.