Ovarian cyst management
Reading File
Finding Sources
Searching PubMed
"ovarian cyst" AND management
Searching the Web
ovarian cyst management guidelines 2024 2025
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive answer. Here is a structured, evidence-based overview of ovarian cyst management.
Ovarian Cyst Management
Classification
Ovarian cysts are broadly divided into functional (non-neoplastic) and neoplastic types. Management differs substantially between them.
Functional Cysts
| Type | Features | Natural History |
|---|---|---|
| Follicular cyst | Most common; rarely >8 cm; follicle fails to rupture | Resolves in 4–8 weeks with expectant management |
| Corpus luteum cyst | Less common; can hemorrhage and rupture; rupture more common on cycle days 20–26 and on the right side | Usually resolves; rupture may need surgery |
| Theca lutein cysts | Bilateral; associated with molar pregnancy, choriocarcinoma, clomiphene, hMG/hCG, GnRH analogs | Regress spontaneously once stimulus removed |
Other Benign Masses
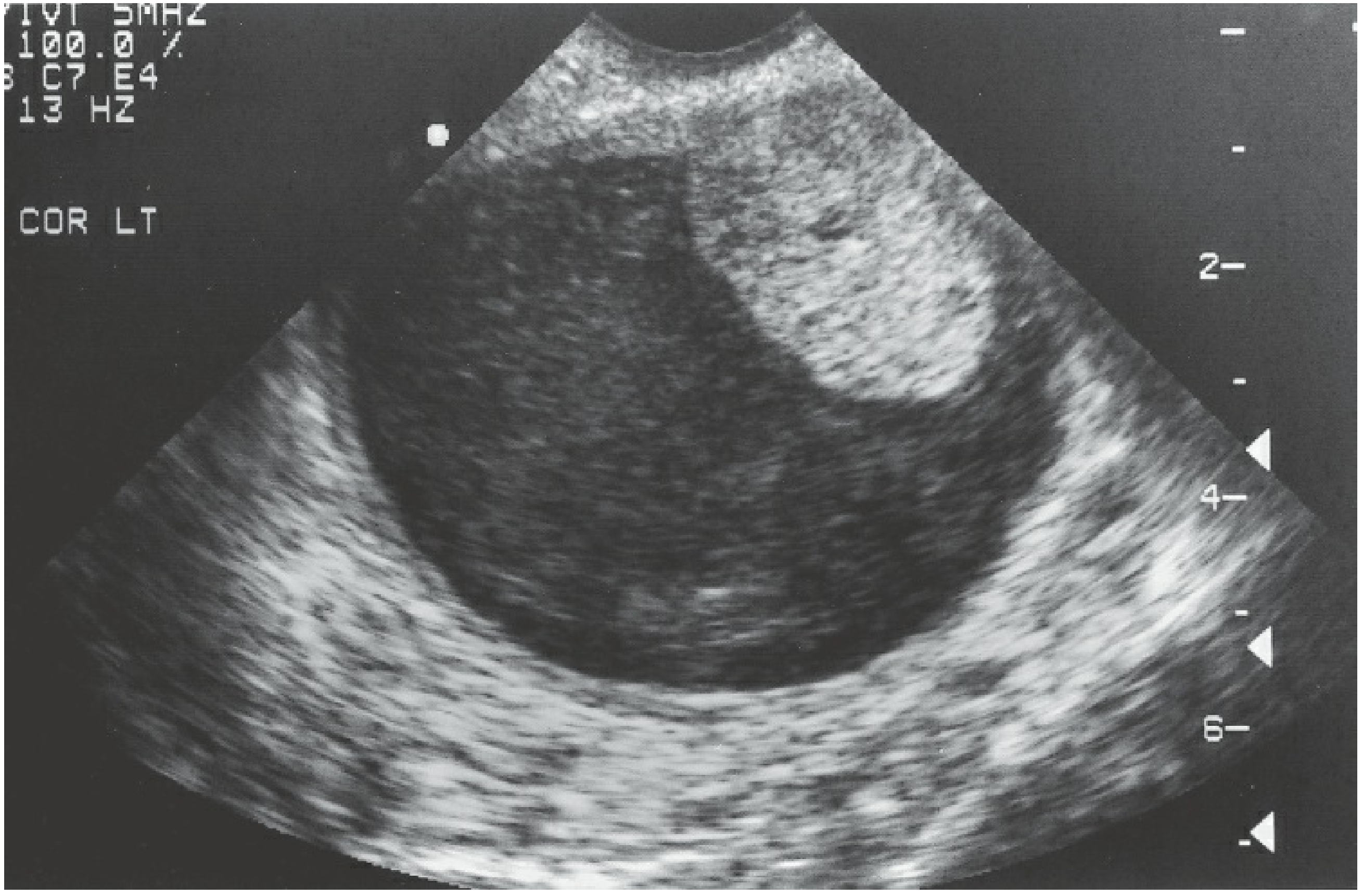
- Endometrioma ("chocolate cyst"): associated with peritoneal endometriosis; classic sonographic finding is unilocular cyst with low-level "ground-glass" echogenicity
- Dermoid (benign cystic teratoma): most common neoplasm to undergo torsion
- Cystadenomas (serous/mucinous): can replace the entire ovary
- Polycystic ovaries: not truly "cysts"; part of PCOS diagnostic spectrum
Initial Evaluation
History & Examination
- Menstrual and reproductive history, contraceptive use, family history of ovarian/breast cancer
- Abdominal and pelvic exam — note: smooth, mobile mass = more likely benign; fixed, nodular = raises malignancy concern
Laboratory
- β-hCG (all reproductive-age women — must exclude ectopic/pregnancy)
- CBC (if rupture/hemorrhage suspected)
- CA-125: not reliable in premenopausal women (elevated with endometriosis, fibroids, PID, pregnancy); CA-125 >200 in premenopausal women warrants gynecologic-oncology co-management
- Additional tumor markers by clinical context: AFP, LDH (germ cell); inhibin A/B (stromal); CEA, CA19-9 (epithelial in older patients)
Imaging — Cornerstone: Transvaginal Ultrasound (TVUS)
TVUS characterizes:
- Size and consistency (unilocular, mixed echogenicity, multiloculated, solid)
- Features raising suspicion for malignancy: size >10 cm, solid components, papillary excrescences, irregularity, ascites
- Specific patterns: endometrioma (ground-glass), dermoid (echogenic with posterior shadowing), corpus luteum (ring of fire on Doppler)
Transvaginal + transabdominal ultrasound are complementary for masses with an abdominal component. MRI is useful for characterization when ultrasound is equivocal.
Management by Clinical Scenario
1. Premenopausal — Functional Cyst (Uncomplicated)
- Expectant management is first-line; follicular cysts resolve in 4–8 weeks
- Oral contraceptives (OCPs): do not hasten resolution of existing cysts, but monophasic OCPs reduce risk of developing new functional cysts by suppressing folliculogenesis and ovulation
- Repeat ultrasound in 6–8 weeks to confirm resolution
- Surgery indicated if: persistent beyond 2–3 cycles, enlarging, symptomatic, or features concerning for neoplasm
2. Premenopausal — Suspected Benign Neoplasm
- Adnexal masses ≥8 cm in premenopausal women generally require surgical exploration
- Laparoscopic ovarian cystectomy: preferred approach for dermoid cysts, fibromas, and most benign neoplasms
- Oophorectomy: often required for larger dermoids and cystadenomas that replace the entire ovary
- Laparotomy: reserved for very large masses, equivocal diagnosis, or suspected malignancy
- Gynecologic oncology consultation when cancer is suspected or complex surgery is anticipated
- — Sabiston Textbook of Surgery
3. Endometrioma
- Many patients managed medically depending on symptoms and fertility desires
- Endometriomas >4 cm are generally refractory to medical management → laparoscopic excision is treatment of choice
- Excision is preferred over drainage (reduces recurrence; preserves fertility better)
- Recent data: women with asymptomatic endometriomas do not need removal prior to ART if the diagnosis is not in question
- — Berek & Novak's Gynecology
4. Postmenopausal
- Any new ovarian cyst in a postmenopausal woman warrants careful evaluation
- Predominantly cystic lesions ≤8 cm may be observed or managed with OCPs for 2 cycles
- Surgical evaluation is appropriate for larger lesions, solid components, or associated symptoms/elevated markers
- — Berek & Novak's Gynecology
5. Pediatric/Premenarcheal
- Adnexal masses ≥2 cm in premenarcheal girls usually require surgical exploration
- Tumor markers: hCG, AFP, LDH; consider CT chest (germ cell tumors can metastasize to lungs/mediastinum)
- Karyotype preoperatively for all premenarcheal girls, especially with dysgerminoma (may arise in dysgenetic gonads)
Complications & Emergency Management
Ruptured Ovarian Cyst
- Corpus luteum cyst is the most common cyst to rupture and cause hemoperitoneum
- Symptoms mimic ectopic pregnancy — always exclude with β-hCG
- Diagnosis: TVUS (quantify free fluid), CBC (falling hematocrit), orthostatic vitals
- Hemodynamically stable, small free fluid → observation ± hospitalization, repeat imaging
- Orthostasis, significant anemia, or large hemoperitoneum → surgical management (laparoscopy preferred, laparotomy if needed)
- Rupture of endometrioma/dermoid → chemical peritonitis; surgical exploration required even without major blood loss
Adnexal Torsion
- Most common neoplasm to torque: dermoid cyst; 83% of torsion occurs in ovaries ≥5 cm
- Presents with acute-onset unilateral pelvic pain + nausea; Doppler flow does NOT rule out torsion
- Urgent surgical management (laparoscopy) — diagnosis often confirmed intraoperatively
- The Ovarian Torsion Composite Index (OT-CI) ≥3 has 100% sensitivity for torsion
Red Flags for Malignancy
| Feature | Comment |
|---|---|
| Size >10 cm | Higher risk |
| Solid or mixed solid-cystic | Requires further workup |
| Papillary excrescences | High concern |
| Bilateral masses | Increases concern |
| Ascites | Strong indicator |
| Postmenopausal status | All new cysts need evaluation |
| CA-125 >200 (premenopausal) | Refer to gynecologic oncology |
| Fixed, nodular pelvic mass | Suspicious for advanced disease |
Summary Algorithm
Ovarian cyst identified on imaging
↓
Is patient pregnant? → Exclude ectopic
↓
Premenopausal Postmenopausal
↓ ↓
Functional cyst? Any new cyst → evaluate
→ Observe 6–8 wks ≤8 cm unilocular → observe
→ Resolves → discharge >8 cm or complex → surgery
→ Persists/enlarges ↓
Features of neoplasm?
↓ Yes
Laparoscopic cystectomy
(oncology consult if suspicious)
Sources:
- Berek & Novak's Gynecology, Chapters 10 & 39 (pp. 452–460, 2378)
- Sabiston Textbook of Surgery, Chapter 29 (pp. 2803–2804)
Treatment for peripheral neuropathy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"peripheral neuropathy" AND treatment
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive, authoritative content from multiple major textbooks. I have enough to construct a thorough, well-organized answer.
Treatment of Peripheral Neuropathy
Guiding Principle: Treat the Underlying Cause First
The primary goal is to identify and treat the treatable cause. In developed countries, diabetes and alcoholism are the most common causes; worldwide, leprosy is the leading treatable cause. Up to 20% of cases remain idiopathic despite thorough evaluation. Removing or correcting the cause (glycemic control, cessation of offending drug, vitamin replacement, treating infection) is the foundation on which symptomatic treatment is built.
— Textbook of Family Medicine 9e
Disease-Specific (Etiologic) Treatment
| Cause | Targeted Intervention |
|---|---|
| Diabetic neuropathy | Tight glycemic control; duloxetine or pregabalin for pain |
| Nutritional deficiency (B12, thiamine, B6) | Vitamin supplementation |
| Alcoholic neuropathy | Alcohol cessation; thiamine/B-vitamin repletion |
| Uremic neuropathy | Dialysis or renal transplantation improves neuropathy |
| HIV neuropathy | Antiretroviral therapy, immunomodulation, symptom relief |
| Hypothyroid neuropathy | Thyroid hormone replacement |
| Multiple myeloma/MGUS | Treating the underlying myeloma can improve neuropathy in >50% |
| Leprosy | Antimicrobial therapy (dapsone + rifampicin ± clofazimine) |
| Toxic/drug-induced | Discontinue offending agent; recovery typically follows |
| Carpal tunnel syndrome | Splinting, corticosteroid injection, surgical decompression |
| Immune-mediated (GBS, CIDP) | IVIG, plasmapheresis, corticosteroids |
Symptomatic Pharmacologic Treatment of Neuropathic Pain
Symptomatic treatment is effective but seldom provides complete relief — best therapies achieve a 30–50% reduction in pain. Simple analgesics (aspirin, acetaminophen, NSAIDs) are rarely beneficial for neuropathic pain alone.
First-Line Agents
1. Anticonvulsants (Gabapentinoids) — Best for lancinating/stabbing pain
| Drug | Starting Dose | Effective Range | Notes |
|---|---|---|---|
| Gabapentin | 300 mg at bedtime (100–300 mg bid/tid in elderly or renal insufficiency) | 900–3,600 mg/day in 2–3 doses | Titrate by 300 mg every 5–7 days; equal efficacy to amitriptyline with fewer side effects |
| Pregabalin | 50–75 mg twice daily | 150–600 mg/day | More linear pharmacokinetics than gabapentin; absorbed more efficiently |
Mechanism: Bind α₂-δ subunits of voltage-dependent calcium channels in the dorsal horn, reducing ectopic neuronal firing. Both act additively with antidepressants and opioids.
Evidence: Controlled trials support use in postherpetic neuralgia (PHN), painful diabetic neuropathy (DPN), HIV polyneuropathy, fibromyalgia, and spinal cord injury pain.
Side effects: Drowsiness, confusion (especially in elderly); both increase overdose risk when co-prescribed with opioids.
2. Antidepressants — Effective for both constant and lancinating pain
Tricyclic Antidepressants (TCAs)
- Amitriptyline, desipramine, nortriptyline: Start at 10–25 mg at bedtime; increase by similar increments no more than once per week; therapeutic doses typically 75–150 mg
- Mechanism: Block reuptake of norepinephrine and serotonin; inhibit sodium channels
- Desipramine and nortriptyline have fewer anticholinergic and sedating effects → preferred in elderly
- Caution: Avoid in ischemic heart disease, narrow-angle glaucoma, prostatism; anticholinergic effects (constipation, dry mouth, urinary retention), orthostatic hypotension
SNRIs
- Duloxetine 60–120 mg/day: Dual 5-HT and norepinephrine reuptake inhibitor; FDA-approved for DPN; moderate effect
- Venlafaxine 150–225 mg/day: Fewer side effects than TCAs but likely less efficacious
- SSRIs are less effective than TCAs for neuropathic pain
Second-Line Agents
Topical Agents (advantage: minimal systemic side effects)
| Agent | Formulation | Use |
|---|---|---|
| Lidocaine 5% patch | Applied to painful area | Proven for PHN; allodynia; burning feet |
| Capsaicin cream 0.075% | Applied 3–4×/day for ≥4 weeks | Depletes substance P in unmyelinated C fibers; initial burning in weeks 1–2 (apply lidocaine cream first to mitigate); long-term benefit remains marginal |
| Capsaicin 8% patch | Specialist-applied | Stronger effect; pretreat with topical lidocaine |
Tramadol
- 200–400 mg/day; centrally acting; μ-opioid + norepinephrine/serotonin reuptake inhibition
- Effective in painful diabetic and other neuropathies; nausea/constipation in ~20%
Third-Line Agents
Other Anticonvulsants
| Drug | Notes |
|---|---|
| Carbamazepine | 1,000–1,600 mg/day; first-line for trigeminal neuralgia; sodium channel blocker; limited by agranulocytosis risk; start low |
| Oxcarbazepine | Better tolerated than carbamazepine; effective >1,200 mg/day; rapid relief in trigeminal neuralgia (24–48 h) |
| Lamotrigine | 200–400 mg/day; effective in HIV neuropathy, SCI pain, trigeminal neuralgia; major risk: Stevens-Johnson syndrome |
| Topiramate | Variable evidence; failed multiple DPN trials |
Opioid Analgesics
- Reserved for failure of adequate trials of first- and second-line agents
- RCTs support oxycodone and levorphanol for PHN and DPN
- Opioids are not first-line for any non-cancer chronic pain — limited evidence for improved quality of life; significant risk of tolerance, hyperalgesia, dependence, addiction
- If used: prefer longer-acting formulations; screen with Opioid Risk Tool; monitor for abuse
- Botulinum toxin A: third-line option; evidence in focal neuropathic pain
Other Adjuvants
- Mexiletine (oral lidocaine): inconsistent results; 100 mg bid, increase slowly
- Ketamine (NMDA antagonist): refractory cases
- Clonidine, baclofen: useful in select patients
- Dextromethorphan: NMDA antagonist; partial relief in DPN but significant sedation/ataxia
- Glucocorticoids (dexamethasone): reduces inflammatory pain; also useful for bone pain
Combination Therapy
When a single agent provides inadequate relief at maximum tolerated dose:
- Gabapentin + nortriptyline is more effective than either drug alone in DPN and PHN
- Gabapentin + tramadol or an opioid is a rational combination
- Gabapentinoids and antidepressants act additively
— Bradley and Daroff's Neurology in Clinical Practice
Non-Pharmacologic Treatment
| Modality | Notes |
|---|---|
| TENS (transcutaneous electrical nerve stimulation) | Low-intensity; reduces pain perception |
| Spinal cord stimulation | For refractory neuropathic pain |
| Acupuncture | Adjunct; some evidence in pain reduction |
| Physiotherapy / graded exercise | Maintains function, prevents deconditioning |
| Multidisciplinary pain program | For chronic refractory neuropathic pain |
| Medical hypnosis / meditation | Reduce pain perception and suffering |
Treatment Hierarchy Summary
PERIPHERAL NEUROPATHY — PAIN MANAGEMENT
Step 1: Treat underlying cause
↓
Step 2: First-line pharmacotherapy
Gabapentin OR Pregabalin
+/- TCA (amitriptyline/nortriptyline) or SNRI (duloxetine)
↓ Inadequate response
Step 3: Second-line
Add/switch to: Tramadol | Topical lidocaine | Topical capsaicin
↓ Still inadequate
Step 4: Third-line
Opioids (oxycodone) | Botulinum toxin A
Alternative anticonvulsants (carbamazepine for trigeminal neuralgia)
↓ Refractory
Step 5: Multidisciplinary pain clinic
Spinal cord stimulation | Ketamine | Combination regimens
Drug Dosing Reference
| Drug | Class | Starting Dose | Target Dose |
|---|---|---|---|
| Gabapentin | α₂-δ ligand | 300 mg qHS | 900–3,600 mg/day |
| Pregabalin | α₂-δ ligand | 50–75 mg bid | 150–600 mg/day |
| Amitriptyline | TCA | 10–25 mg qHS | 75–150 mg/day |
| Nortriptyline | TCA | 10–25 mg qHS | 75–150 mg/day |
| Duloxetine | SNRI | 30 mg/day | 60–120 mg/day |
| Venlafaxine | SNRI | 37.5 mg/day | 150–225 mg/day |
| Carbamazepine | Na⁺ channel blocker | Low (titrate) | 1,000–1,600 mg/day |
| Lamotrigine | Na⁺ channel blocker | 25–50 mg/day | 200–400 mg/day |
| Tramadol | Weak opioid + SNRI | 50 mg | 200–400 mg/day |
| Capsaicin cream 0.075% | Topical | 3–4× daily | ≥4 weeks trial |
| Lidocaine 5% patch | Topical Na⁺ blocker | 1–3 patches/day | Applied to painful area |
Sources:
- Bradley and Daroff's Neurology in Clinical Practice, Chapter 106 (pp. 2711–2718)
- Barash, Cullen, and Stoelting's Clinical Anesthesia 9e, Chapter 56 (p. 4776)
- Goldman-Cecil Medicine, Chapter 26 (pp. 271–272)
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 2 (p. 125)
- Textbook of Family Medicine 9e, Chapter 14 (p. 1241)
This is a shared conversation. Sign in to Orris to start your own chat.