How to interpret penile Doppler reports
Reading File
Finding Sources
Finding Sources
Searching PubMed
penile duplex Doppler ultrasound erectile dysfunction interpretation
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching the Web
penile Doppler interpretation PSV EDV resistive index normal values criteria 2024
Reading File
Loading Image
I now have comprehensive information to provide a thorough answer. Let me compile it all.
Interpreting Penile Doppler Reports
Penile Doppler (penile duplex ultrasonography) is the most reliable and least-invasive method for assessing erectile dysfunction (ED) hemodynamics. It combines high-resolution ultrasound (7.5–12 MHz) with pulsed color Doppler, always performed after intracavernosal pharmacostimulation (ICI).
1. How the Study Is Performed
Pharmacostimulation: A vasoactive agent is injected into the corpus cavernosum — typically alprostadil 10–20 µg, papaverine+phentolamine (Bimix 0.3 mL), or Trimix 0.3 mL. Flow velocities are measured at baseline then every 5 minutes up to 20 minutes.
Color coding: Blood flowing toward the probe = red; blood flowing away = blue. The entire penis from the crural base to the glans can be imaged.
What is measured:
- PSV — Peak Systolic Velocity (cm/s)
- EDV — End-Diastolic Velocity (cm/s)
- RI — Resistive Index = (PSV − EDV) / PSV
- Cavernous artery diameter (baseline vs. post-injection)
- Acceleration time — the systolic rise time
2. Key Parameters & Normal Values
| Parameter | Normal | Borderline | Abnormal |
|---|---|---|---|
| PSV | ≥ 35 cm/s | 25–35 cm/s | < 25 cm/s |
| EDV (at full erection) | < 5 cm/s (ideally 0 or negative) | — | > 5 cm/s |
| Resistive Index (RI) | ≥ 0.80 | 0.75–0.80 | < 0.75 |
| Acceleration time | — | — | > 122 ms |
| Artery diameter change | > 75% increase post-ICI | — | < 75% increase |
A normal erection in a healthy young man: PSV ~89 cm/s, EDV = 0 cm/s, RI = 1.0 (as shown in the image below)
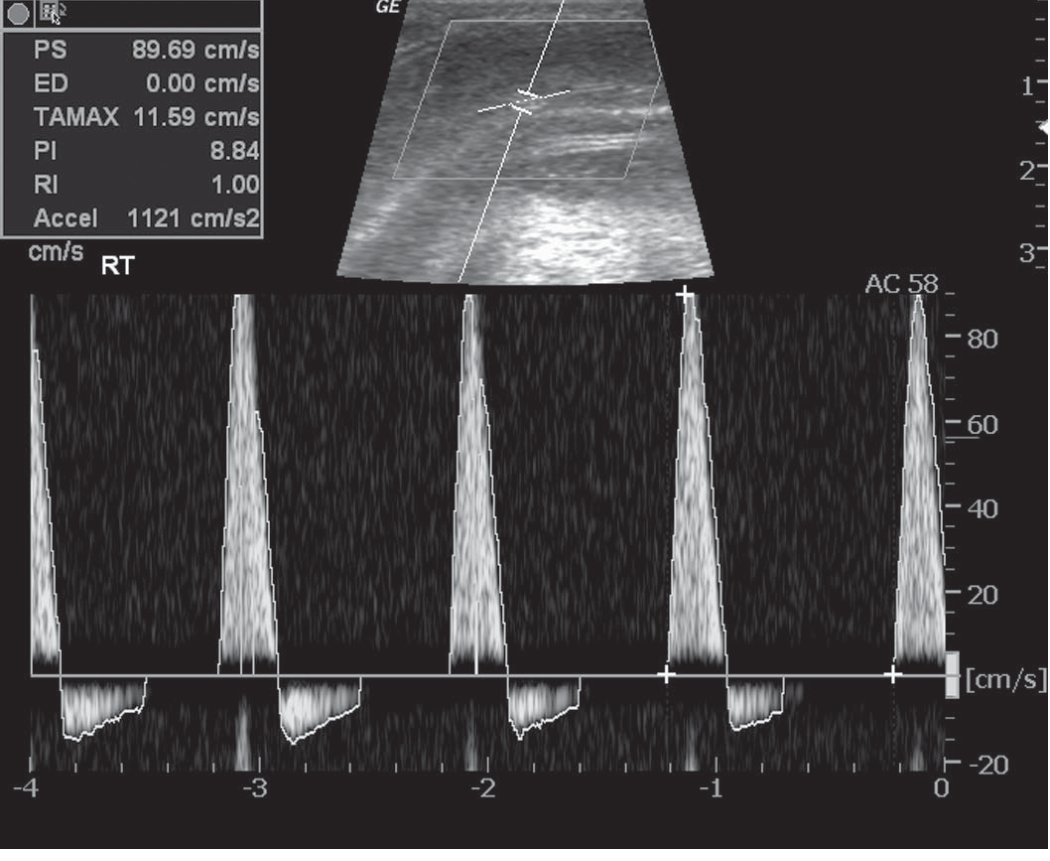
Smith & Tanagho's General Urology, Fig. 39-4A — Excellent arterial response: PS = 89.69 cm/s, ED = 0 cm/s, RI = 1. Note the negative (below-baseline) diastolic flow wave, indicating intracavernosal pressure exceeding systemic diastolic BP.
3. Waveform Pattern During Normal Erection Progression
Understanding the phase-dependent waveform is essential:
| Phase | PSV | EDV | Color |
|---|---|---|---|
| Flaccid | Low | Low forward | — |
| Filling phase (0–5 min post-ICI) | ↑↑ High (both systole & diastole increase) | High forward | Red |
| Tumescence | High, sharp peak | Decreasing | — |
| Full erection / rigidity | Sharp, tall spikes | Zero or negative (reversal) | Shift red → blue at diastole |
The reversal of diastolic flow (flow below baseline) is a hallmark of normal corporal veno-occlusion — it means intracavernosal pressure has risen above systemic diastolic BP.
4. Diagnostic Interpretation
Arteriogenic ED (Arterial Insufficiency)
- PSV < 25 cm/s — diagnostic of cavernous arterial insufficiency
- PSV 25–35 cm/s — borderline; ~20% of these patients may still have normal CIS test (false-positive zone)
- Acceleration time > 122 ms — additional marker of poor arterial inflow
- Artery diameter increase < 75% after ICI — supportive finding
- Asymmetry: A difference of > 10 cm/s between the two cavernous arteries suggests a unilateral atherosclerotic lesion; flow reversal across a collateral vessel may indicate the same
Venogenic ED (Cavernous Veno-Occlusive Dysfunction)
- EDV > 5 cm/s at 15–20 min post-ICI (when PSV is adequate, i.e., ≥ 25–30 cm/s)
- RI < 0.75 — indicates failure of veno-occlusive mechanism
- Rapid detumescence despite high PSV
- The key point: EDV should only be interpreted as abnormal when arterial inflow is confirmed adequate (PSV ≥ 35 cm/s); if PSV is low, high EDV may simply reflect poor arterial drive rather than true venous leak
Normal Vascular Function
- PSV ≥ 35 cm/s, EDV = 0 cm/s (or negative), RI ≥ 0.80 → suggests psychogenic or neurogenic ED
Mixed Vasculogenic ED
- Low PSV and elevated EDV → combined arterial and venous pathology
5. Special Findings
| Finding | Interpretation |
|---|---|
| Sustained high PSV + rapid detumescence + EDV > 5 cm/s | Venogenic (venous leak) impotence |
| High-flow turbulent signal without ICI | High-flow priapism (post-traumatic arteriocavernous fistula) |
| Asymmetric PSV > 10 cm/s difference | Unilateral cavernous artery stenosis / atherosclerosis |
| Echogenic plaques in tunica albuginea | Peyronie's disease (Doppler can localize plaque) |
| Intracavernosal heterogeneous echo | Fibrosis / prior trauma |
6. Technical Pitfalls
- Anatomic variants: Early branching or multiple cavernous arteries can falsely lower measured PSV. Perforators from dorsal or spongiosal arteries can alter velocity measurements.
- Measurement location matters: PSV varies between crus, proximal, and mid-cavernosal positions.
- Patient anxiety: Can suppress the erectile response, giving falsely low PSV — always re-dose before concluding arteriogenic ED.
- Inadequate pharmacostimulation: A subtherapeutic ICI dose is the most common cause of false arteriogenic diagnosis. Re-dose if erection quality is poor.
- EDV interpretation only valid when PSV is adequate: Don't label venous leak if PSV is low.
7. Summary Decision Tree
Post-ICI Penile Doppler
│
▼
PSV < 25 cm/s ──────────────► Arteriogenic ED
│
PSV 25–35 cm/s ─────────────► Borderline / repeat or re-dose
│
PSV ≥ 35 cm/s
│
├── EDV < 5 cm/s, RI ≥ 0.80 ──► Normal vascular; consider psychogenic/neurogenic
│
└── EDV ≥ 5 cm/s, RI < 0.75 ──► Venogenic ED (cavernous veno-occlusive dysfunction)
Sources:
- Campbell-Walsh-Wein Urology, Chapter 69: Duplex Ultrasonography (Gray Scale or Color-Coded), pp. 2019–2020
- Smith & Tanagho's General Urology, 19th ed., p. 627 (Color Duplex Ultrasonography section)
Management of peyronies disease
Finding Sources
Searching PubMed
Peyronie disease management treatment
Finding Sources
Reading Article
PMID: 41359447
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.