Ebstein anomaly explain from nelson textbook of pediatrics
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive information. Let me compile the full, detailed answer.
Note: Nelson's Textbook of Pediatrics is not available in the medical library database. The response below draws from Schwartz's Principles of Surgery (11th Ed.), Braunwald's Heart Disease (a standard reference for congenital heart disease), and Fuster and Hurst's The Heart (15th Ed.) - all authoritative, peer-reviewed sources covering Ebstein anomaly in full detail consistent with Nelson's coverage.
Ebstein Anomaly
Definition
Ebstein anomaly is a congenital cardiac malformation characterized by apical (inferior) displacement of the tricuspid valve - specifically the septal and posterior leaflets - into the right ventricle (RV), due to failure of delamination of the tricuspid valve leaflets from the underlying RV endocardium during embryogenesis.
- Incidence: 1 per 200,000 live births; accounts for less than 1% of all congenital heart disease
- Named after Wilhelm Ebstein, who described it in 1866
Anatomy
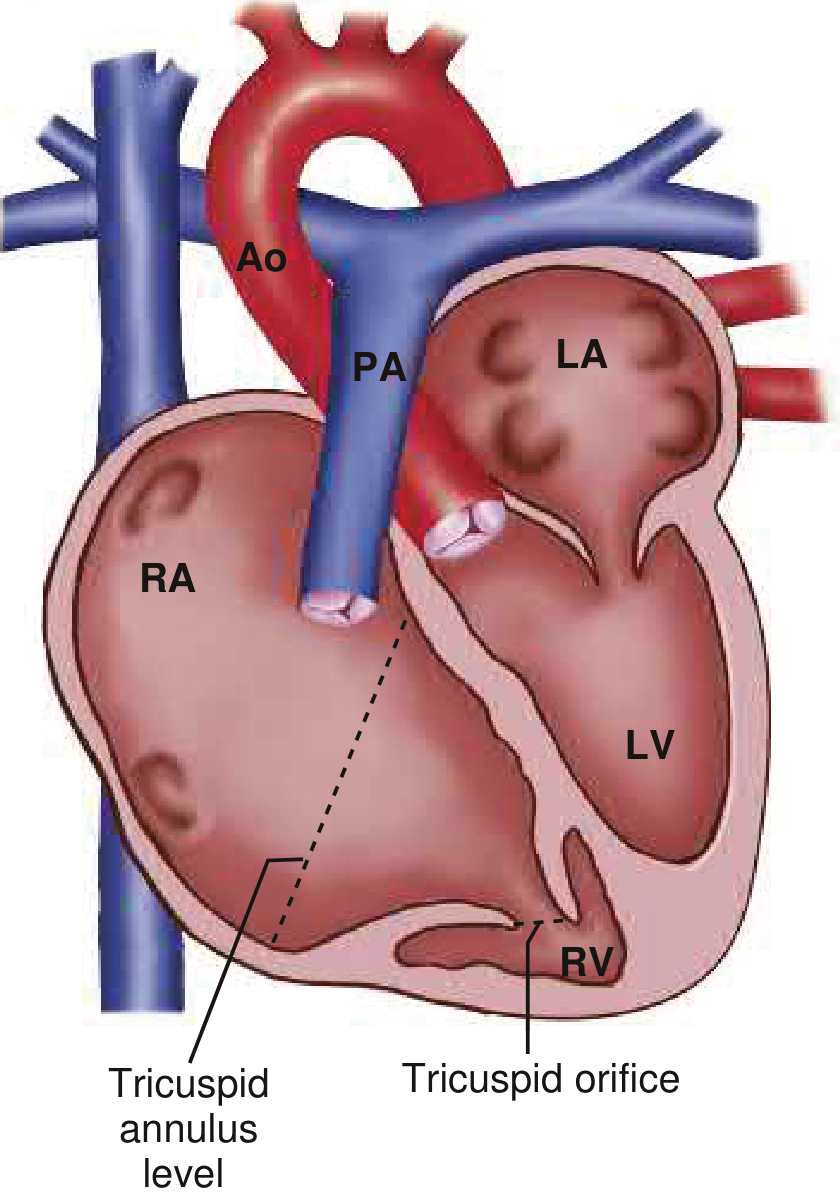
Key anatomical features:
| Structure | Finding |
|---|---|
| Anterior leaflet | Attached at normal annular position; elongated, "sail-like," may be fenestrated |
| Septal + posterior leaflets | Inferiorly displaced into RV |
| Diagnostic criterion | Displacement > 8 mm/m² between AV valve insertion sites, or >20 mm in adults |
| Right ventricle | Divided into two parts: atrialized RV (inlet, thin/dilated) + functional/trabeculated RV (outlet) |
| Right atrium | Massively dilated, includes the atrialized RV |
| Tricuspid valve | Regurgitant, "sail-like" anterior leaflet |
The atrialized RV is the portion between the true AV groove and the displaced valve. It is thin-walled, dilated, and contracts paradoxically (discordantly) with the rest of the RV - a key contributor to dysfunction.
Associated anomalies:
- ASD or patent foramen ovale (PFO) - most common associated defect, causes right-to-left shunt and cyanosis
- WPW syndrome / accessory pathway - present in 15% of patients (multiple right-sided accessory pathways are common)
- Pulmonary stenosis or atresia (functional or anatomical)
- VSD, PDA, mitral valve disease, bicuspid aortic valve
- L-loop TGA (Ebstein-like anomaly of tricuspid valve)
- Left ventricular non-compaction
Pathophysiology
RV dysfunction results from two main mechanisms:
- Inflow obstruction at the level of the atrialized ventricle - produces ineffective RV filling
- Tricuspid regurgitation - worsened by progressive annular dilatation, further reduces effective forward flow
The discordant contraction of the large atrialized portion and the reduced number of myocardial fibers in the functional RV cause contractile dysfunction.
In severe neonatal cases:
- Lack of forward RV output produces functional/physiologic pulmonary atresia - the infant becomes ductus-dependent
- All systemic venous return is shunted right-to-left across the ASD
- The enormously enlarged RV compresses the LV ("pancaked" LV on short-axis echo), impairing LV filling and output
- To-and-fro flow within the atrialized RV prevents adequate intracardiac mixing
Clinical Features
The clinical spectrum directly mirrors the anatomical severity:
Neonate/Infant (severe form)
- Cyanosis and acidosis at birth
- Respiratory distress
- Heart failure
- May be lethal in utero (hydrops fetalis) in the most severe cases
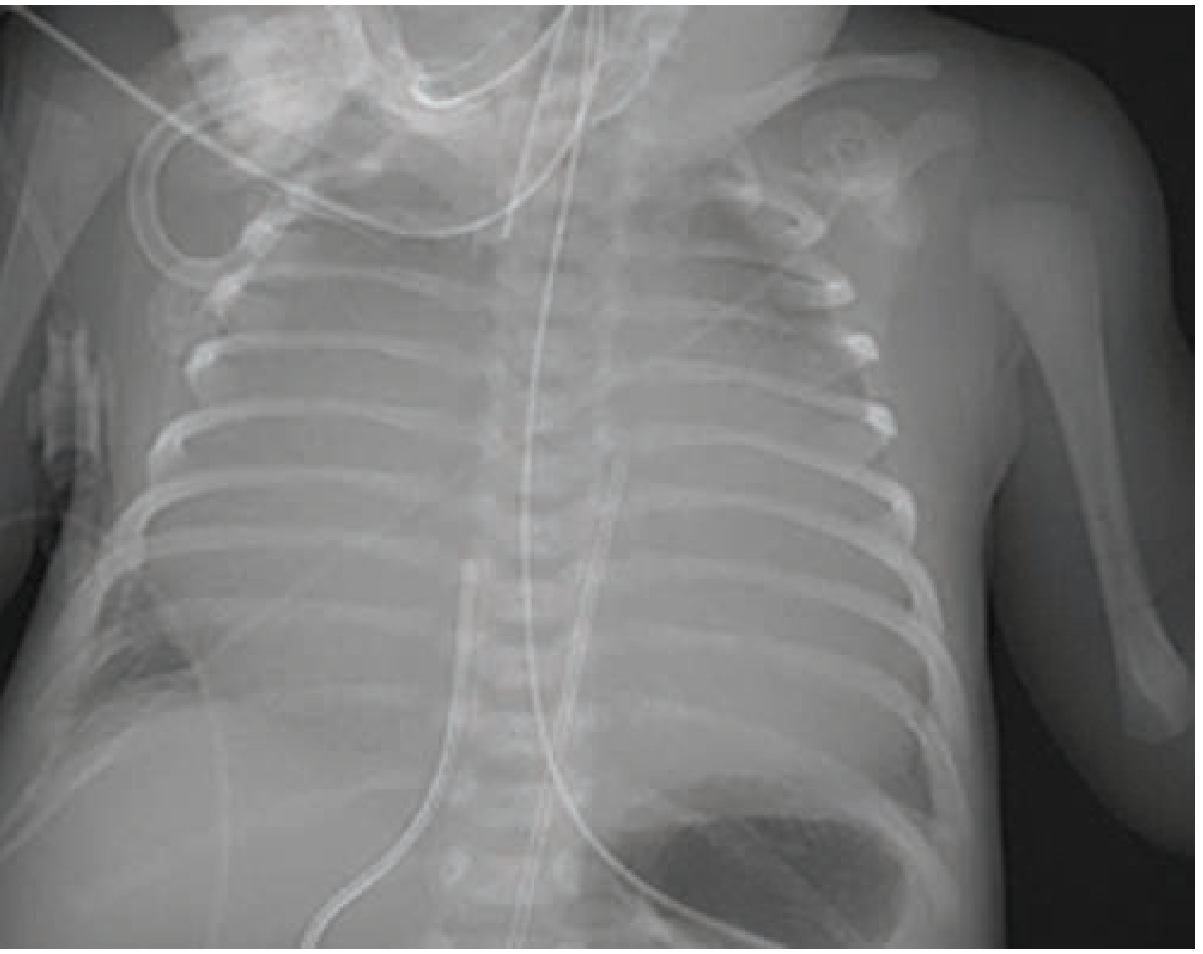
- Cardiomegaly ("wall-to-wall" heart on CXR)
Older child / adolescent / adult (milder form)
- Gradual onset of symptoms; average age of diagnosis in mid-teens
- Exercise intolerance, fatigue
- Cyanosis (from right-to-left shunt across ASD)
- Palpitations / arrhythmias (SVT, pre-excitation, atrial flutter/fibrillation)
- Symptoms of right heart failure (edema, ascites)
- Paradoxical embolism (stroke) from right-to-left shunt
Investigations
Chest X-Ray
- Classic: globular "wall-to-wall" heart or "box-shaped" heart
- Decreased pulmonary vascular markings
- Small aortic and pulmonary trunk shadow
ECG
- "Himalayan" P waves (>5 mm) - giant peaked P waves due to massive right atrial enlargement
- Prolonged PR interval
- Right bundle branch block (complete or incomplete) - RSR' pattern in V1
- Short PR interval + delta wave (WPW pattern) - in ~15% with accessory pathway
- Right axis deviation
- Atrial flutter or fibrillation (common in adults)
- Low voltage QRS
Echocardiography (diagnostic standard)
- Confirms inferior displacement of tricuspid valve leaflets
- Assesses: tricuspid valve morphology, degree of TR, size of atrialized RV, functional RV size, pulmonary valve, ASD direction of shunt
- Diagnostic criterion: septal leaflet displacement >8 mm/m²
Cardiac MRI (CMR)
- Quantifies: RV volumes, RV systolic function, LV volumes, degree of TR, cardiac output, Qp:Qs
- RV and LV systolic dysfunction on CMR are associated with mortality and sustained VT
- Useful when echo is suboptimal
Electrophysiology Study (EPS)
- Indicated for: WPW on ECG, history of SVT, wide-complex tachycardia, or syncope
- Radiofrequency ablation performed if accessory pathway identified
Prognostic Scoring: Great Ormond Street Score (GOSE)
Used to stratify neonates with Ebstein anomaly:
$$\text{GOSE} = \frac{\text{Area of RA} + \text{Area of atrialized RV}}{\text{Area of functional RV} + \text{LA} + \text{LV}}$$
| GOSE Score | Ratio | Mortality |
|---|---|---|
| 1 | < 0.5 | 8% |
| 2 | 0.5 - 1.0 | 8% |
| 3 | 1.1 - 1.4 | 100% |
| 4 | > 1.5 | 100% |
A score > 2 predicts uniformly fatal outcome.
Management
Medical (non-operative)
- Prostaglandin E1 (PGE1) infusion in ductus-dependent neonates
- Diuretics for heart failure
- Anti-arrhythmic therapy (though ablation is preferred over medication for accessory pathways)
- Annual follow-up lifelong; more frequent if RV dysfunction, cyanosis, cardiomegaly, or arrhythmia
Indications for Surgery
Surgery is indicated for:
- Symptomatic infants
- Older children/adults with NYHA class III or IV
- Progressive cyanosis
- Arrhythmias (WPW/SVT)
- Worsening exercise tolerance
Preference: Treat arrhythmias with ablation before surgery, as post-surgical access to right-sided pathways is hindered.
Surgical Options
1. Danielson Repair (1992) - standard for children/adults surviving infancy:
- Excision of redundant right atrial tissue
- Patch closure of ASD
- Plication of the atrialized RV (obliteration of aneurysmal cavity)
- Posterior tricuspid annuloplasty (narrows the annulus)
- Reconstruction of tricuspid valve using anterior leaflet ("monocusp" repair)
- Tricuspid valve replacement if reconstruction not feasible
- Intraoperative EPS + ablation for pre-excitation
2. Starnes Procedure - for symptomatic neonates:
- Placement of a fenestrated patch to close the tricuspid valve orifice (converting to single-ventricle physiology)
- Combined with systemic-to-pulmonary artery shunt (BT shunt)
- Fenestration allows RV decompression in pulmonary atresia
- Followed by staged Fontan pathway
3. One-and-a-half ventricle repair:
- Bidirectional cavopulmonary shunt (Glenn) diverts SVC blood to pulmonary arteries
- RV propels IVC blood to pulmonary arteries via RVOT
- Results in separate systemic and pulmonary circulations in series
- For patients with hypoplastic/dysplastic RV
Natural History and Complications
- Younger age at diagnosis, male gender, cardiothoracic ratio ≥0.65, and severe valve displacement predict decreased survival
- Atrial arrhythmia (particularly AVRT) is the most common complication, increasing with age - often precedes adverse events
- Sudden death associated with multiple accessory pathways + atrial fibrillation
- Biventricular failure or sudden death are the main causes of death in unoperated patients
- Women with Ebstein anomaly can become pregnant; outcomes related to degree of TR, RV dysfunction, cyanosis, and arrhythmias
Sources
- Schwartz's Principles of Surgery, 11th Ed., Ch. 20 (Congenital Heart Disease)
- Braunwald's Heart Disease, 2-Vol Set - Cardiovascular Medicine, Ch. 82
- Fuster and Hurst's The Heart, 15th Ed., Ch. 67
Coarctation of aorta explain from nelson textbook of pediatrics
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the material needed for a comprehensive, well-illustrated answer. Let me compose it.
Note: Nelson's Textbook of Pediatrics is not in the medical library database. The response below draws from multiple peer-reviewed surgical and cardiology textbooks - Schwartz's Principles of Surgery (11th Ed.), Sabiston Textbook of Surgery, Bailey & Love's Short Practice of Surgery (28th Ed.), The Developing Human (Clinically Oriented Embryology), and Braunwald's Heart Disease - all covering coarctation of the aorta with pediatric-specific detail consistent with Nelson's coverage.
Coarctation of the Aorta (CoA)
Definition
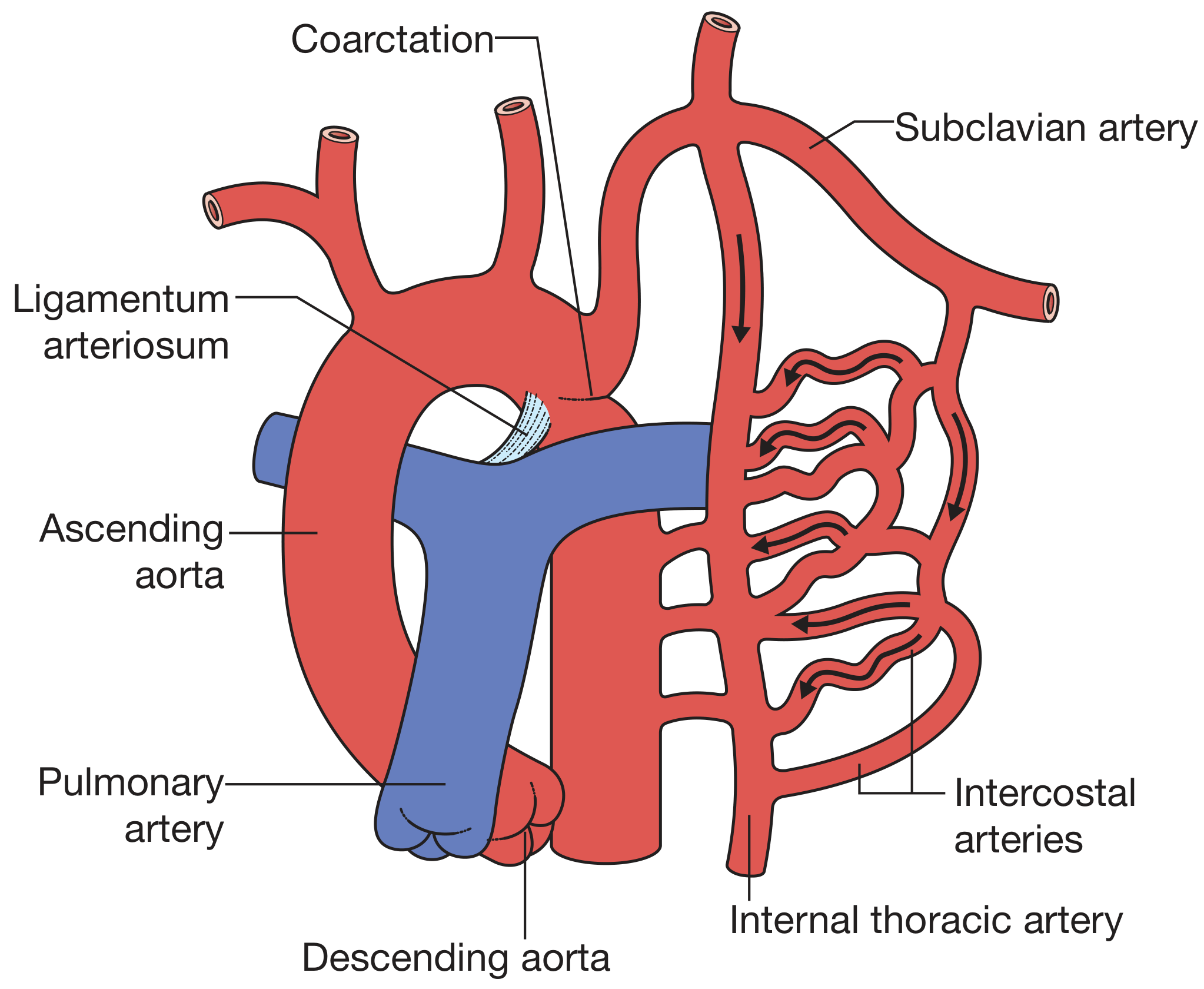
Coarctation of the aorta is a hemodynamically significant luminal narrowing of the aorta, most commonly located in the descending thoracic aorta just distal to the left subclavian artery, at or near the insertion of the ductus arteriosus (ligamentum arteriosum).
- Accounts for 6-8% of all congenital heart disease
- Incidence: approximately 3 per 10,000 live births
- Males affected twice as often as females
- Associated with Turner syndrome in females (45,X)
Embryology
Three competing embryological theories explain CoA:
-
Ductal tissue theory - Smooth muscle of the ductus arteriosus is incorporated into the aortic wall during development. When the ductus constricts after birth, the ductal muscle within the aorta also constricts, forming a coarctation shelf.
-
Abnormal involution theory - Abnormal involution of a small segment of the left dorsal aorta during arch development leads to a stenotic segment that later migrates cranially with the left subclavian artery.
-
Isthmus theory - During fetal life, the aortic isthmus (between the left subclavian artery and the ductus) normally carries very little blood and remains narrow. After ductal closure at birth, this segment normally widens. Failure of this widening results in a persistent coarctation.
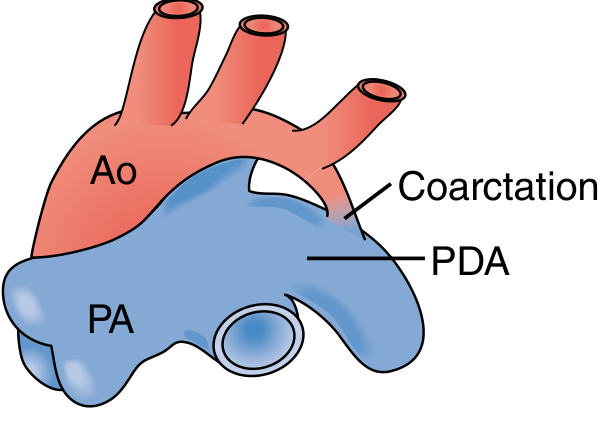
In 90% of cases, the coarctation is directly opposite the ductus arteriosus (juxtaductal position).
Classification
| Type | Position | Features |
|---|---|---|
| Preductal (Infantile) | Proximal to ductus/ligamentum | Long segment, severe, symptomatic in neonates; ductus-dependent; associated with hypoplastic arch |
| Juxtaductal (Periductal) | At the level of the ductus | Most common; discrete shelf of intimal tissue; may have associated PDA |
| Postductal (Adult type) | Distal to ductus | Collateral circulation well developed prenatally; presents in late childhood/adolescence |
Associated Anomalies
- Bicuspid aortic valve - most common association, present in 25-70% of cases
- Patent ductus arteriosus - often critical in preductal type
- Ventricular septal defect (VSD)
- Atrial septal defect (ASD)
- Shone syndrome - a complex of multiple left heart obstructive lesions: mitral stenosis, subaortic stenosis, CoA, and aortic stenosis
- Subaortic stenosis, LV hypoplasia, endocardial fibroelastosis
- Circle of Willis aneurysms (berry aneurysms) - increased risk of rupture
Pathophysiology
CoA causes obstruction to left ventricular outflow, producing two distinct hemodynamic consequences:
1. Proximal (upper body) hypertension
- Results from both mechanical obstruction to LV ejection AND activation of the renin-angiotensin-aldosterone system (RAAS) due to renal hypoperfusion
- Leads to LV pressure overload → LV hypertrophy → eventual LV failure
- Importantly, hypertension often persists even after surgical repair (particularly with late repair)
2. Distal (lower body) hypoperfusion
- The descending aorta, abdominal viscera, kidneys, and lower limbs receive reduced blood flow
- Leads to: fluid overload, excess renin secretion, metabolic acidosis, intestinal ischemia
- Lower extremity claudication and fatigue on exertion
Ductal dependency (neonates)
- In preductal CoA, the ductus arteriosus is the sole source of blood to the lower body prenatally
- As the ductus closes in the first days of life, the neonate rapidly deteriorates - cardiogenic shock, acidosis, oliguria
- PGE1 infusion is emergency treatment to keep or reopen the ductus
Collateral circulation
- In postductal CoA, extensive collateral circulation develops - primarily via intercostal arteries and internal thoracic (mammary) arteries
- This bypasses the obstruction and perfuses the descending aorta
- Causes rib notching on CXR (dilated posterior intercostal vessels erode the inferior rib margins)
Clinical Features
Neonates / Young Infants (Severe / Preductal CoA)
- Appears well in first 2-4 days of life (ductus still patent, bypassing the coarctation)
- As ductus closes: acute deterioration - pallor, poor perfusion, tachypnea, tachycardia
- Signs of cardiogenic shock: poor feeding, lethargy, weak pulses, cool extremities
- Absent or markedly diminished femoral pulses
- Differential cyanosis (lower body blue, upper body pink - if PDA is present with right-to-left shunting through it)
- Hepatomegaly, pulmonary edema
Older Children / Adolescents (Postductal / Juxtaductal CoA)
- Often asymptomatic for years
- Discovered incidentally during screening for upper body hypertension
- Headaches, epistaxis (from hypertension)
- Tired legs, cramping, intermittent claudication on exercise
- Prominent pulsation in the neck (due to hypertension and collaterals)
- Pulsation felt under the ribs (intercostal collaterals)
Physical Examination
| Finding | Significance |
|---|---|
| Radio-femoral delay | Delayed femoral pulse vs. radial pulse; cardinal sign |
| Upper extremity > lower extremity BP | >20 mmHg gradient is significant |
| Absent/weak femoral pulses | Hallmark finding |
| Hyperdynamic precordium | LV pressure overload |
| Murmur | Harsh systolic murmur, best heard over the left chest and posterior thorax/back |
| Continuous murmur over scapula | From large collateral vessels |
| Prominent suprasternal notch pulsations | Dilated carotid/subclavian arteries |
Investigations
Chest X-Ray
- Rib notching (inferior surface of ribs 3-8 bilaterally) - due to dilated tortuous posterior intercostal arteries; NOT seen in infants (collaterals not yet developed)
- "Figure-of-3" sign (also called "3 sign") on plain film - the upper bulge is the dilated left subclavian artery, the middle indentation is the coarctation, and the lower bulge is the post-stenotic dilatation of the descending aorta
- "E sign" on barium swallow - mirror image of figure-of-3
- Heart size: usually normal in older children; cardiomegaly may be present in neonates
- Pulmonary venous congestion in acute presentation
ECG
- Left ventricular hypertrophy (in older patients)
- Right ventricular hypertrophy may predominate in neonates
Echocardiography (primary diagnostic modality)
- Demonstrates the narrowed aortic segment and the pressure gradient across it
- Assesses: aortic arch anatomy, transverse arch hypoplasia, bicuspid aortic valve, associated intracardiac defects, LV function
- Doppler shows elevated peak velocity and diastolic run-off pattern (typical of significant obstruction)
CT Angiography / MRI
- Provides precise 3D anatomy of arch, coarctation length, and collaterals
- Useful pre-operatively, especially for transverse arch assessment and re-coarctation
Cardiac Catheterization
- Reserved for equivocal cases
- Increasingly used as a therapeutic rather than purely diagnostic modality (balloon dilation ± stenting)
Management
Emergency Management (Neonate in Shock)
- PGE1 infusion - reopens the ductus arteriosus to restore lower body perfusion (standard of care)
- Resuscitation: correct acidosis, inotropic support, mechanical ventilation if needed
- Stabilize before definitive surgical repair
Surgical Treatment (Gold Standard)
Surgery via left thoracotomy (third or fourth intercostal space) is the standard approach for most pediatric cases, especially neonates and infants.
Surgical techniques:
| Technique | Description | Indication |
|---|---|---|
| Resection + end-to-end anastomosis | Most common; excise coarctation, primary anastomosis | Discrete CoA in all ages |
| Extended end-to-end anastomosis | Anastomosis extends along the lesser curve of the arch | Distal arch hypoplasia; promotes arch growth |
| Aortic arch advancement | All-native tissue repair; allows somatic growth | Transverse arch hypoplasia |
| Subclavian flap aortoplasty (Waldhausen) | Left subclavian artery transected and used as a vascularized patch over coarctation | Avoids prosthetic material; less used now (risk: left arm ischemia) |
| Prosthetic patch aortoplasty | Prosthetic patch used to enlarge stenotic segment | Long-segment CoA, re-coarctation; high risk of late aneurysm (especially Dacron) |
| Interposition tube graft | Prosthetic graft replaces coarctation segment | Long-segment CoA, previous surgery |
- Balloon dilation in neonates is avoided as primary therapy due to high re-coarctation rate and risk of aortic wall disruption
- Concomitant intracardiac defects (e.g., large VSD + arch hypoplasia) may be repaired simultaneously via median sternotomy on CPB
Catheter-Based Intervention
- Balloon angioplasty ± stenting: increasingly used for older children and adults; standard for adults with isolated CoA; off-label stenting reduces recurrence but raises concerns about somatic growth and lifetime metal implant risk
- Primary treatment for re-coarctation after surgical repair
- Mean gradient reduction ~74% in native CoA, higher for recurrent
Complications Without Treatment
The majority of patients die before age 40 years without correction. Causes of death:
- Left ventricular failure (most common)
- Infective endocarditis
- Aortic rupture or dissection
- Haemorrhagic stroke (from associated berry aneurysms + hypertension)
- Myocardial infarction (from coronary artery disease driven by chronic hypertension)
Post-Repair Complications and Follow-up
| Complication | Notes |
|---|---|
| Persistent/recurrent hypertension | Common even after anatomically successful repair; more likely with late repair |
| Re-coarctation | Most common long-term surgical complication; treatable with balloon ± stent |
| Aneurysm at repair site | Particularly after Dacron patch aortoplasty (up to 89% of aneurysms in this group) |
| Spinal cord ischemia / paraplegia | 0.5% incidence; prevented by left heart bypass / distal perfusion during repair |
| Complete heart block | Risk during surgery near conduction tissue |
| Circle of Willis aneurysm rupture | Ongoing risk, especially with residual/recurrent hypertension |
- Lifelong follow-up is mandatory
- Blood pressure monitoring in all four limbs
- Regular imaging (echo, MRI/CT) to assess repair site and aortic arch
- Anti-hypertensive therapy (ACE inhibitors, beta-blockers) as needed
Prognosis
- Early surgical repair gives excellent outcomes and is associated with prevention of long-term hypertension
- Pre-repair hypertension may not fully resolve despite successful repair, especially if repair is delayed
- Long-term survival after repair is near-normal when performed early and without major residual defects
Sources
- Schwartz's Principles of Surgery, 11th Ed., Ch. 20
- Sabiston Textbook of Surgery (Biological Basis of Modern Surgical Practice), Ch. 113
- Bailey and Love's Short Practice of Surgery, 28th Ed., Ch. 59
- The Developing Human - Clinically Oriented Embryology, Ch. 13
This is a shared conversation. Sign in to Orris to start your own chat.