Paget disease
Reading File
Finding Sources
Searching PubMed
"Paget disease"[MeSH Terms] AND bone
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent. I have comprehensive information. Let me now compile the full, structured answer using all the gathered content.
Paget's Disease of Bone
Definition
Paget's disease is a localized bone-remodeling disorder affecting widespread, non-contiguous skeletal areas. The pathologic process begins with overactive osteoclastic bone resorption followed by compensatory, disorganized osteoblastic new bone formation, producing a structurally abnormal mosaic of woven and lamellar bone. Pagetic bone is expanded, less compact, and more vascular - making it susceptible to deformities and fractures. - Harrison's Principles of Internal Medicine, 22nd Ed.
Epidemiology
- Prevalence ~0.5% in the UK and USA; common in Western Europe (Britain, France, Germany) but rare in Scandinavia, Africa, Asia, and the Middle East
- Greater prevalence in males; increases markedly with age
- Autopsy series reveal disease in ~3% of individuals over age 40
- Radiographic prevalence in patients >55 years: 2.5% men, 1.6% women
- For unclear reasons, prevalence and severity have been declining, and age at diagnosis is increasing
- Harrison's, p. 3312; Goldman-Cecil Medicine
Etiology
Both genetic and viral factors are implicated.
Genetic Factors
- Positive family history in 15-25% of patients (raises prevalence 7-10x among first-degree relatives)
- Key gene mutations:
| Gene | Protein | Disease |
|---|---|---|
| SQSTM1 (most common) | Sequestosome-1/p62 | Familial and sporadic Paget's |
| TNFRSF11B | Osteoprotegerin (OPG) | Juvenile Paget's (familial idiopathic hyperphosphatasia) |
| TNFRSF11A | RANK | Familial expansile osteolysis; early-onset Paget's |
| VCP (valosin-containing protein) | - | Inclusion body myopathy + Paget's + frontotemporal dementia (IBMPFD) |
| CSF1 | M-CSF | Increased osteoclast differentiation |
| TM7SF4 | DC-STAMP | Osteoclast fusion |
Viral Factors
-
Paramyxovirus inclusions (measles, RSV, canine distemper virus) found in pagetic osteoclasts
-
Viral mRNA detected in osteoclast precursors
-
Decline in Paget's disease coincides with widespread measles vaccination
-
However, no live virus has been cultured from pagetic bone, and antibody levels against paramyxoviruses are not elevated in affected patients
-
Harrison's Principles of Internal Medicine, 22nd Ed.
Pathophysiology
The RANK/RANKL/OPG axis is central to the pathology:
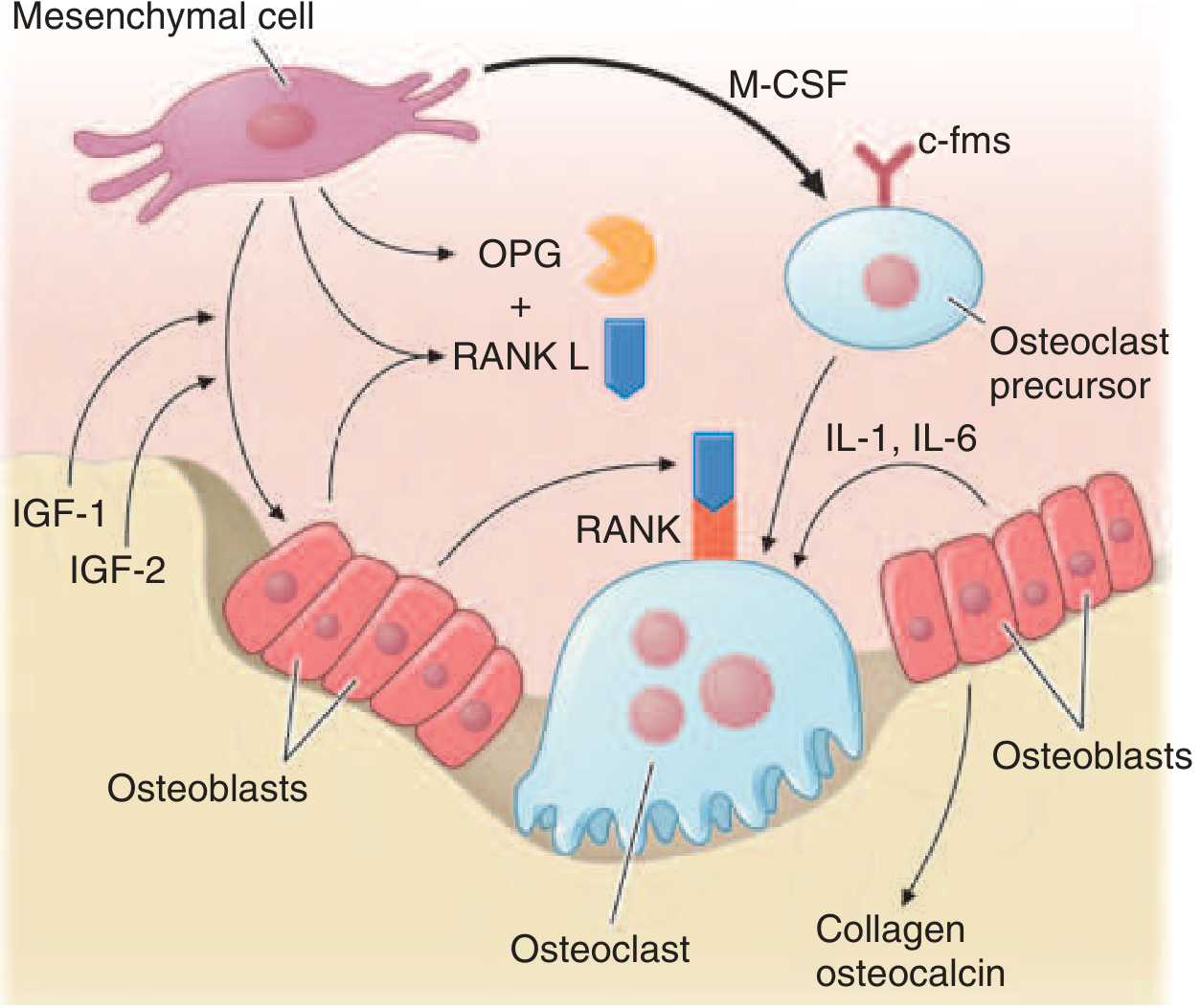
Figure: Factors promoting osteoclast and osteoblast differentiation and function (from Harrison's, 22nd Ed.)
Key cellular abnormalities:
- Pagetic osteoclasts are 10-100x more numerous than normal; may have up to 100 nuclei (vs. 3-5 normally)
- Resorptive surfaces increase sevenfold; erosion rate: 9 μg/day (normal = 1 μg/day)
- Osteoclast precursors are hypersensitive to 1,25(OH)2D3 and hyperresponsive to RANKL
- Marrow stromal cells show increased RANKL expression
- IL-6 is elevated in blood and overexpressed in pagetic osteoclasts
- c-fos (proto-oncogene) and Bcl-2 (antiapoptotic) are overexpressed
Three Phases of Paget's Disease
- Osteolytic phase - prominent bone resorption, hypervascularization; radiographic "blade of grass" or advancing lytic wedge
- Mixed phase - simultaneous resorption and formation; woven bone replaces lamellar bone; fibrous connective tissue replaces marrow
- Sclerotic (osteoblastic) phase - bone formation predominates; "cotton wool" appearance on X-ray; mosaic pattern histologically
Bone mass is normal or increased (not reduced), unless there is vitamin D/calcium deficiency.
Sites Affected
Most common sites (in order):
- Pelvis (most common, ~70%)
- Femur
- Skull
- Tibia
- Lumbar spine
- Cervical spine and clavicle (less common)
Clinical Features
Most patients (~70-80%) are asymptomatic at diagnosis.
Symptoms - Direct Bony Involvement
- Bone pain - deep, aching, worse at rest; most common symptom
- Deformities - bowing of the tibia ("saber shin"), frontal bossing, enlarged skull
- Pathologic fractures - especially transverse "chalk-stick" fractures of the femur or tibia
- Warmth over affected bone due to increased vascularity
Symptoms - Neural Compression
- Hearing loss (most common neurologic complication) - from encroachment on the auditory foramina or cochlear involvement
- Headache and tinnitus (skull involvement)
- Spinal cord/nerve root compression - from vertebral enlargement
- Platybasia (basilar invagination) - can compress the brainstem
- Cranial nerve palsies
Systemic Complications
- High-output cardiac failure - from arteriovenous shunting through hypervascular pagetic bone (rare, requires >35% skeletal involvement)
- Immobilization hypercalcemia - when patients with active disease are immobilized
- Gout and pseudogout - due to hyperuricemia from rapid bone turnover
- Secondary osteoarthritis - from joint deformity (especially hip)
Malignant Transformation
- Osteosarcoma develops in <1% of patients - but in this setting carries a very poor prognosis
- Suspect if: sudden increase in pain, soft tissue mass, rapid rise in ALP
- Less commonly: fibrosarcoma or chondrosarcoma
Diagnosis
Laboratory
| Test | Finding in Active Paget's |
|---|---|
| Serum Alkaline Phosphatase (ALP) | Markedly elevated (best single marker of bone formation activity) |
| Urine hydroxyproline or N-telopeptide | Elevated (bone resorption markers) |
| Serum Ca²⁺, PO₄ | Usually normal |
| Serum PTH | Usually normal |
Radiology
- Plain X-ray - first-line: cortical thickening, bone expansion, coarsened trabecular pattern, "cotton wool" in skull, "blade of grass" lytic front in long bones, "picture frame" vertebra
- Bone scan (technetium-99m) - best for defining extent of skeletal disease; shows intense uptake in pagetic areas
- CT/MRI - useful for suspected complications (nerve compression, sarcomatous change)
Treatment
When to Treat
- Symptomatic disease (pain, neurologic compromise, deformity)
- Pre-operatively for surgery on pagetic bone (to reduce vascularity and bleeding)
- Hypercalcemia of immobilization
- Prophylactic treatment when disease is adjacent to joints, skull base, or weight-bearing bones - but this remains debated
Bisphosphonates (First-Line)
| Drug | Dose | Notes |
|---|---|---|
| Zoledronate (preferred) | 5 mg IV single infusion | Longest remission (months to years); may repeat if ALP remains elevated |
| Risedronate | 30 mg/day × 2 months | Oral; effective; no osteomalacia |
| Alendronate | 40 mg/day × 6 months | Oral; effective; GI side effects at high doses |
| Pamidronate | IV infusion | Used in many countries |
| Etidronate | 5 mg/kg/day | Rarely used now; risk of osteomalacia at higher doses |
Treatment should not exceed 6 months per course but may be repeated after a 6-month break. ALP normalization is the treatment goal. - Katzung's Basic and Clinical Pharmacology, 16th Ed.
Calcitonin (Second-line / Adjunct)
- Subcutaneous or IM: 50-100 MRC units every day or every other day
- Nasal spray: 200-400 units/day
- Effect requires weeks to months; tachyphylaxis (loss of response) develops over time - not due to antibody formation
- Used when bisphosphonates are contraindicated or poorly tolerated
Other Management
- Analgesia (NSAIDs) for bone pain
- Surgery - joint replacement for severe secondary arthritis, osteotomy for deformity, spinal decompression for cord/nerve compression
- Hearing aids for hearing loss (not reversible with treatment)
Summary Table
| Feature | Detail |
|---|---|
| Pathology | Increased osteoclast activity → disorganized bone remodeling |
| Key gene | SQSTM1 (most common) |
| Most affected bone | Pelvis |
| Lab hallmark | Elevated ALP |
| Best extent imaging | Bone scan |
| Most common complication | Hearing loss |
| Most feared complication | Osteosarcoma (<1%) |
| Treatment of choice | Zoledronate 5 mg IV |
Sources: Harrison's Principles of Internal Medicine 22nd Ed., Goldman-Cecil Medicine, Katzung's Basic and Clinical Pharmacology 16th Ed., Firestein & Kelley's Textbook of Rheumatology.
This is a shared conversation. Sign in to Orris to start your own chat.