Ards defination and pathology
Reading File
Finding Sources
Searching PubMed
"acute respiratory distress syndrome"[MeSH Terms] AND "definition"
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have all the content needed to write a comprehensive answer. Let me compile the full response.
Acute Respiratory Distress Syndrome (ARDS)
Definition
ARDS is a clinical syndrome of acute, diffuse, inflammatory lung injury that leads to increased pulmonary vascular permeability, increased lung weight, and loss of aerated lung tissue. It is characterized by non-cardiogenic pulmonary edema with severe hypoxemia refractory to oxygen therapy.
- Robbins & Kumar Basic Pathology defines it as: "A clinical syndrome of respiratory insufficiency caused by diffuse alveolar damage."
- Sabiston Textbook of Surgery states: "ARDS is an inflammatory response of the lung to multiple inciting factors... characterized by decreasing ability to oxygenate and decreased compliance of the lung."
Berlin Definition (2012) - The Current Standard
The ARDS Definition Task Force (Berlin, 2012) replaced older criteria (including the American-European Consensus Conference definition) with the following:
| Criterion | Details |
|---|---|
| Timing | Onset within 1 week of a known clinical insult or new/worsening respiratory symptoms |
| Chest Imaging | Bilateral opacities not fully explained by effusions, lobar/lung collapse, or nodules |
| Origin of Edema | Respiratory failure not fully explained by cardiac failure or fluid overload; if no ARDS risk factor present, echocardiography required to exclude hydrostatic edema |
| Oxygenation | PaO2/FiO2 ratio ≤300 mmHg with PEEP ≥5 cmH2O |
Severity Classification (by PaO2/FiO2):
| Severity | PaO2/FiO2 Ratio | Mortality |
|---|---|---|
| Mild | 200 - 300 mmHg | ~35% |
| Moderate | 100 - 200 mmHg | ~40% |
| Severe | < 100 mmHg | ~46% |
Source: Tintinalli's Emergency Medicine; Harrison's Principles of Internal Medicine 22E
2023 Update (proposed): The Berlin criteria have been updated to include non-intubated patients (using SpO2/FiO2 ≤315 if SpO2 ≤97% on high-flow nasal oxygen ≥30 L/min or CPAP/NIV), ultrasound as an alternative imaging modality, and criteria for resource-limited settings without PEEP requirements. - Harrison's 22E, 2025
Common Causes / Precipitating Factors
Direct (pulmonary) causes:
- Pneumonia (most common)
- Aspiration of gastric contents
- Pulmonary contusion
- Inhalation injury
Indirect (extrapulmonary) causes:
- Sepsis (most common overall trigger)
- Major trauma
- Severe acute pancreatitis
- Blood product transfusions (TRALI)
- Burns, shock
Pathology
Gross Pathology
In the acute exudative stage, the lungs are heavy, firm, red, and boggy. They show congestion, interstitial and intra-alveolar edema, inflammation, fibrin deposition, and diffuse alveolar damage. This manifests radiologically as patchy ground-glass opacities with or without consolidation.
- Robbins, Cotran & Kumar Pathologic Basis of Disease
The Three Overlapping Pathologic Phases

ARDS phases over time (Harrison's, 22E)
Phase 1 - Exudative Phase (Days 0-7)
This is the hallmark phase of ARDS. It is defined by the pathologic term Diffuse Alveolar Damage (DAD).
Pathogenesis:
- Alveolar capillary endothelial cells and type I pneumocytes are injured
- Loss of the normally tight alveolar-capillary barrier to fluid and macromolecules
- Protein-rich exudate leaks into interstitial and alveolar spaces
- Pro-inflammatory cytokines (IL-1, IL-6, IL-8, TNF-α) and lipid mediators (leukotriene B4) are elevated
- Neutrophil recruitment into pulmonary interstitium and alveoli - neutrophils release proteases, ROS, and cytokines causing further injury
Histologic findings:
- Widespread alveolar and interstitial edema, inflammation, and hemorrhage
- Hyaline membranes - composed of precipitated plasma proteins, fibrin, necrotic epithelial cell debris, and dysfunctional surfactant components - these are the pathological footprint of DAD
- Type I alveolar epithelial cells more severely damaged than Type II cells
- Swollen, disorganized epithelium detached from basement membranes
- Widened interstitium with leukocytes, platelets, RBCs, fibrin
- Pulmonary vascular injury: microthrombi and fibrocellular proliferation
- Inactivated/lost surfactant -> alveolar collapse
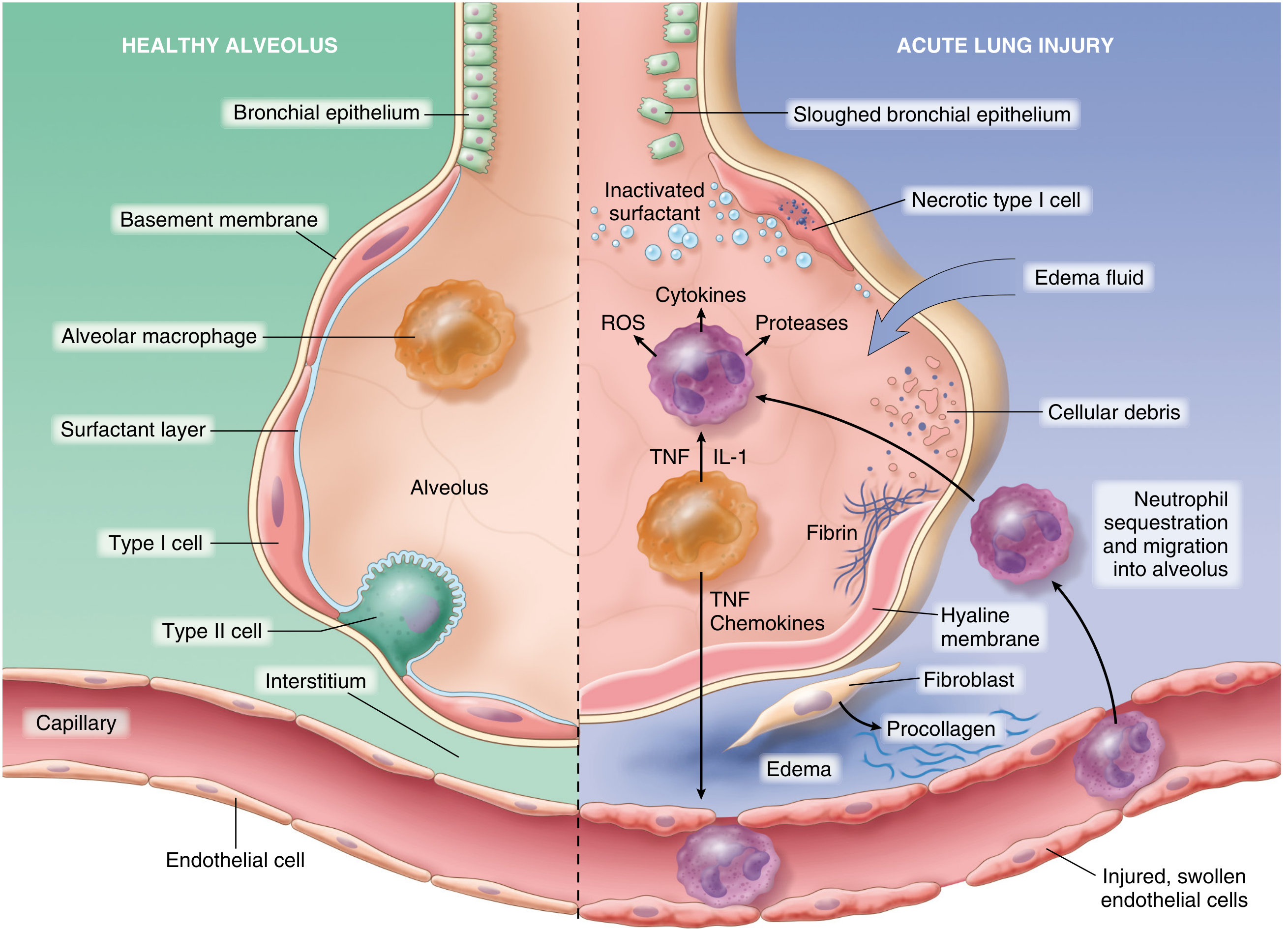
The normal alveolus compared with the injured alveolus in acute lung injury/ARDS. Note: neutrophil infiltration, TNF/IL-1 cytokine release, hyaline membrane formation, fibrin, edema, and injured endothelium. (Robbins, Cotran & Kumar)
Functional consequences:
- Decreased respiratory system compliance (stiff lungs)
- Right-to-left intrapulmonary shunting (ventilation-perfusion mismatch)
- Profound, refractory hypoxemia
- Increased pulmonary dead space (minute ventilation ~twice normal, ~12 L/min)
- Pulmonary hypertension (from hypoxic vasoconstriction, fibrin deposition, vascular compression)
Phase 2 - Proliferative Phase (Days 7-21)
- Follows the exudative phase in a subset of patients
- Type II pneumocytes proliferate (attempt at epithelial repair)
- Hyaline membranes are reorganized
- Granulation tissue forms in alveolar walls and spaces
- Fibrin prominent in alveoli and interstitium
- Infiltration with fibroblasts (activated early in injury)
- Air-blood barrier thickened by interstitial and epithelial enlargement
- Decrease in neutrophil numbers
- Some reabsorption of edema fluid
Many patients begin to recover clinically during this phase, but some develop progressive lung injury and early pulmonary fibrosis.
- Murray & Nadel's Textbook of Respiratory Medicine; Harrison's 22E
Phase 3 - Fibrotic Phase (Day 21+)
- Occurs only in a subset of patients with persistent ARDS (>2 weeks)
- Pulmonary fibrosis with obliteration of pulmonary capillaries
- Deposition of interstitial and alveolar collagen
- Bullae formation
- Greatly reduced lung volumes and compliance
- Elevated N-terminal procollagen peptide III in BAL fluid (marker of active collagen synthesis) can be detected as early as 24 hours after onset - suggesting fibroproliferation may begin simultaneously with inflammation
- Murray & Nadel's Textbook of Respiratory Medicine
DAD - The Pathological Correlate of ARDS
Diffuse alveolar damage (DAD) is the histopathological term used to describe the combination of edema, hemorrhage, and hyaline membranes seen on lung biopsy or autopsy in ARDS.
Important caveat: Studies confirm that only ~50% of ARDS patients show evidence of DAD on autopsy or lung biopsy. Patients with confirmed DAD tend to be:
- Younger
- More severely ill
- Have poorer lung compliance and lower P/F ratios
- Have 5x higher mortality from hypoxemic respiratory failure
Non-DAD pathology in ARDS includes: infectious pneumonia, diffuse alveolar hemorrhage, acute eosinophilic pneumonia, drug-associated pneumonitis.
- Murray & Nadel's Textbook of Respiratory Medicine
Key Pathological Summary Table
| Feature | Exudative Phase | Proliferative Phase | Fibrotic Phase |
|---|---|---|---|
| Timing | Days 0-7 | Days 7-21 | >Day 21 |
| Key lesion | Hyaline membranes, DAD | Type II cell proliferation, granulation | Collagen deposition, fibrosis |
| Cells | Neutrophils dominant | Fibroblasts, Type II pneumocytes | Fibroblasts |
| Edema | Protein-rich, heavy | Resolving | Minimal |
| Compliance | Very low | Improving | Very low (fibrosis) |
| Outcome | May recover or progress | Most recover here | Chronic lung disease |
Key References:
- Berlin ARDS Definition (JAMA 2012) - the current diagnostic standard
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 632-633
- Murray & Nadel's Textbook of Respiratory Medicine, Ch. 134 (Pathology section)
- Harrison's Principles of Internal Medicine 22E (2025), Ch. 312
- Fishman's Pulmonary Diseases and Disorders, Ch. 140
Explain in simple tutor like language
ARDS - Explained Simply 🫁
What is ARDS? (The Simple Version)
Imagine your lungs are like a sponge - normally soft, airy, and good at soaking up oxygen. In ARDS, that sponge gets flooded with fluid and filled with gunk, so it can't do its job anymore.
The full name is Acute Respiratory Distress Syndrome - let's break that down:
- Acute = happens suddenly, within hours to days
- Respiratory = it's a lung problem
- Distress = the lungs are in serious trouble
- Syndrome = a collection of signs and symptoms together
One-liner definition: ARDS is when the lungs get so severely inflamed and flooded that even giving the patient pure oxygen doesn't fix their low blood oxygen levels.
What Causes It?
Think of ARDS as the lungs overreacting to an insult. The insult can hit the lungs directly, or it can start somewhere else in the body and still damage the lungs.
Direct hits to the lung:
- Severe pneumonia
- Breathing in vomit (aspiration)
- Smoke or toxic gas inhalation
Indirect hits (from elsewhere in the body):
- Sepsis - the #1 cause overall (a body-wide infection gone haywire)
- Severe pancreatitis
- Major trauma
- Blood transfusions gone wrong (TRALI)
Think of it this way: Sepsis is like a fire alarm going off in the whole building (your body), and the lungs are the room that gets the most smoke damage.
The Berlin Definition - How Doctors Diagnose ARDS
Doctors use 4 criteria - all 4 must be present:
✅ 1. TIMING → Symptoms appear within 1 week of a trigger
✅ 2. CHEST X-RAY → White patches (opacities) on BOTH sides of the lungs
✅ 3. NOT THE HEART → The fluid isn't there because of heart failure
✅ 4. LOW OXYGEN → PaO2/FiO2 ratio ≤ 300 mmHg (even with breathing support)
The Severity Scale - Think of it like a Traffic Light
| Severity | P/F Ratio | Simple meaning |
|---|---|---|
| 🟡 Mild | 200 - 300 | Lungs struggling |
| 🟠 Moderate | 100 - 200 | Lungs in serious trouble |
| 🔴 Severe | < 100 | Lungs barely working |
What is P/F ratio? It compares how much oxygen is in the blood (PaO2) versus how much oxygen you're breathing in (FiO2). A healthy person has a P/F ratio of ~400-500. In ARDS it crashes below 300.
The Pathology - What's Actually Happening Inside the Lung?
ARDS goes through 3 phases - think of it like a fire, then rebuilding, then scars.
🔥 Phase 1 - Exudative Phase (Days 0 to 7)
"The Flooding"
What's the trigger?
Something (sepsis, pneumonia, etc.) activates the immune system, which calls in neutrophils (the army of white blood cells).
Here's what happens step by step:
INJURY
↓
Neutrophils rush into the lungs
↓
They release toxic chemicals (ROS, proteases, cytokines like TNF-α, IL-1, IL-8)
↓
These chemicals damage the walls between the air sacs and the blood vessels
↓
The "barrier" breaks down → protein-rich fluid LEAKS into the air sacs (alveoli)
↓
Air sacs fill with fluid instead of air → lungs can't oxygenate blood
Under the microscope you see:
- Hyaline membranes - a waxy pink lining inside the air sacs, made of fibrin, dead cell debris, and proteins. This is the hallmark finding - called Diffuse Alveolar Damage (DAD)
- Lots of neutrophils
- Flooded, collapsed air sacs
- Swollen, damaged Type I cells lining the alveoli
- Inactivated surfactant (the soap-like substance that keeps alveoli open)
Analogy: The hyaline membrane is like plastic wrap stuck to the inside of a balloon - air can't get in properly.
Clinically: Patient is severely short of breath, very low oxygen levels, needs a ventilator.
🔨 Phase 2 - Proliferative Phase (Days 7 to 21)
"The Repair Crew Arrives"
The acute flooding is calming down. The body starts trying to clean up and rebuild.
- Type II pneumocytes (the repair cells of the lung) start multiplying to replace the dead Type I cells
- Hyaline membranes start getting cleared away
- Fibroblasts (connective tissue cells) move in to patch up damage
- Fluid starts being reabsorbed
- Neutrophils decrease
Good news: Most patients who survive start getting better here.
Bad news: Some patients start laying down scar tissue instead of normal lung.
🪨 Phase 3 - Fibrotic Phase (Day 21+)
"The Scar"
This only happens in a minority of patients who don't recover.
- The lung starts scarring over (fibrosis)
- Air sacs get replaced by scar tissue
- Lungs become permanently stiff
- Can cause chronic lung disease and even cor pulmonale (right heart failure)
Analogy: Think of a cut on your skin. Most of the time it heals cleanly. Sometimes it heals with a thick, hard scar. ARDS fibrosis is the lung doing that - scarring instead of proper healing.
The Full Timeline at a Glance
Why Can't You Just Give More Oxygen?
Great question. Normally if someone is low on oxygen, you give them oxygen and it works. In ARDS it doesn't - because:
- The air sacs are flooded - oxygen can't reach the blood even if you blow it in
- There's severe V/Q mismatch - blood is flowing to parts of the lung that can't ventilate
- This is called an intrapulmonary shunt - blood bypasses the functional lung entirely
Analogy: Imagine trying to dry a soaking wet sponge by blowing air at it. If the sponge is completely saturated, blowing more air doesn't help much.
Quick Summary Box
| What | ARDS |
|---|---|
| What is it? | Severe non-cardiogenic lung flooding and inflammation |
| Pathological term | Diffuse Alveolar Damage (DAD) |
| Hallmark histology | Hyaline membranes |
| Key cells | Neutrophils (exudative), Type II pneumocytes + fibroblasts (proliferative) |
| Key problem | Alveolar-capillary barrier breakdown → protein-rich fluid floods alveoli |
| Phases | Exudative (0-7d) → Proliferative (7-21d) → Fibrotic (>21d) |
| Mortality | 35-46% depending on severity |
| Treatment | Lung-protective ventilation (6 mL/kg tidal volume), prone positioning |
This is a shared conversation. Sign in to Orris to start your own chat.