
IMG20260608182038.jpg
Spot diagnosis
Reading File
Searching the Web
winged scapula causes diagnosis children serratus anterior palsy
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Diagnosis: Winged Scapula (Scapula Alata)
The image clearly shows prominent winging of the right scapula - the medial border and inferior angle are visibly protruding away from the thoracic wall, a classic sign of serratus anterior weakness.
What is happening anatomically?
The serratus anterior muscle normally anchors the scapula firmly against the posterior chest wall. When it weakens or is paralysed, the scapula loses its medial fixation and the vertebral border "lifts off" - producing the wing-like protrusion seen here.
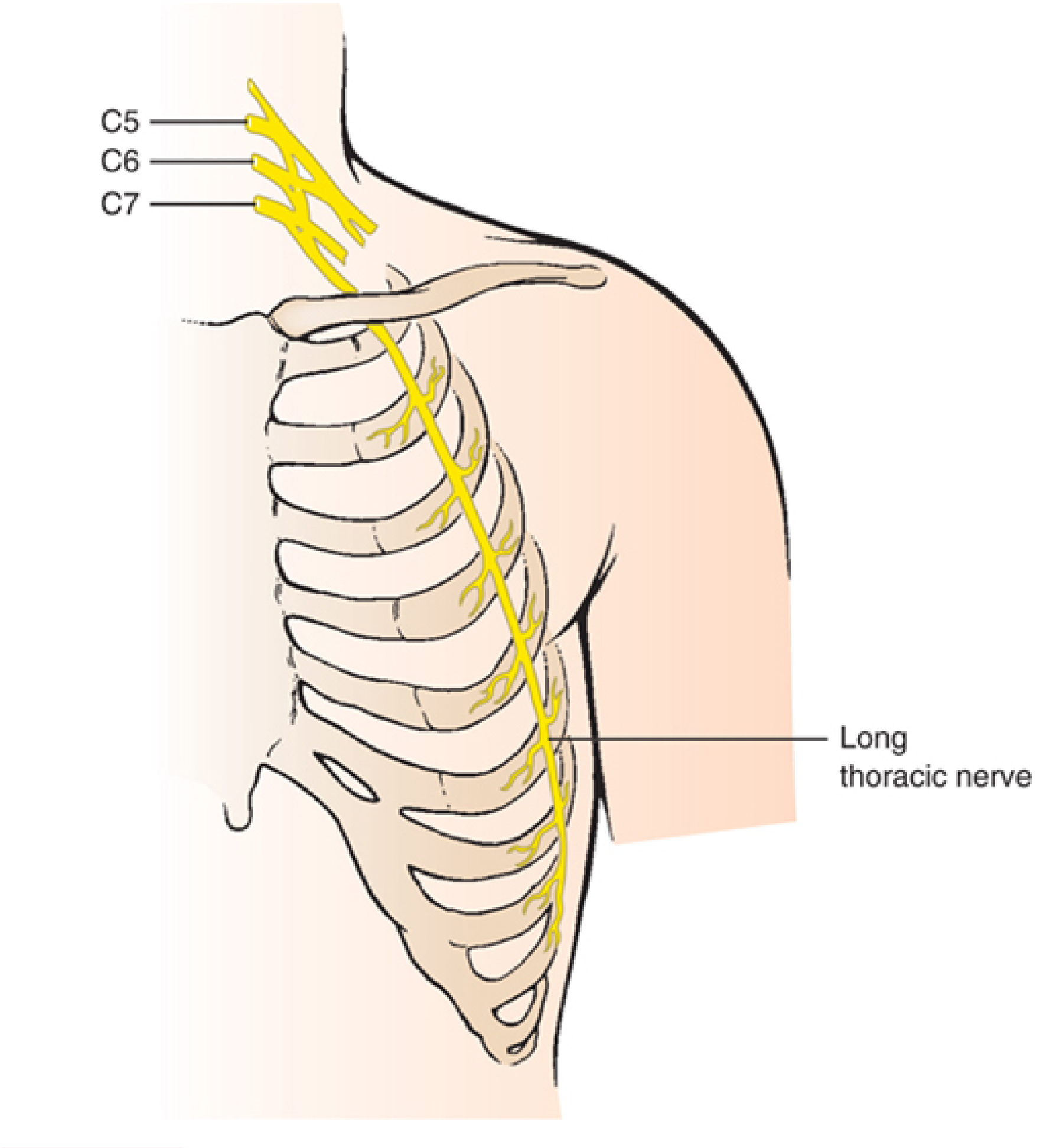
The long thoracic nerve (C5-C6-C7) courses along the lateral thoracic wall to supply the serratus anterior.
Most Common Cause
Long thoracic nerve palsy is by far the most frequent cause. A review of 128 patients with unilateral winged scapula found:
- Long thoracic nerve palsy: 70 cases
- Spinal accessory nerve palsy: 39 cases
- Both nerves: 5 cases
- Facioscapulohumeral dystrophy (FSHD): 5 cases
(Localization in Clinical Neurology, 8e)
Differential Diagnosis in a Child
| Cause | Key feature |
|---|---|
| Long thoracic nerve palsy (C5-7) | Most common; trauma, carrying heavy bags ("rucksack palsy"), viral illness, neuralgic amyotrophy |
| Spinal accessory nerve palsy (CN XI) | Trapezius weakness; scapula drops and rotates differently |
| Facioscapulohumeral muscular dystrophy (FSHD) | Bilateral, family history, facial weakness |
| Congenital absence/hypoplasia of serratus anterior | Present from birth, no preceding illness |
| Parsonage-Turner syndrome | Acute onset severe pain followed by weakness |
Clinical Clues - How to Confirm
- Wall push-up test: Ask the patient to push outstretched arms against a wall - winging becomes dramatically more pronounced with serratus anterior palsy (especially in the lower two-thirds of the scapula).
- Check arm elevation - difficulty raising arm above 90° is common.
- EMG/NCS - to confirm long thoracic neuropathy.
- In a child: also consider FSHD - check for facial weakness, bilateral involvement, and family history.
Management
- Most cases (especially long thoracic nerve palsy) are self-limiting and resolve within 18 months with conservative care.
- Physiotherapy - scapular stabilisation exercises.
- Surgical options (pectoralis major transfer, scapulothoracic fusion) only for refractory cases beyond 2 years.
(Localization in Clinical Neurology 8e; Fischer's Mastery of Surgery 8e)
This is a shared conversation. Sign in to Orris to start your own chat.