How to do cervical circlage
Reading File
Finding Sources
Searching PubMed
"cervical cerclage"[MeSH Terms] AND technique
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
I now have all the information needed. Here is a comprehensive answer on cervical cerclage.
Cervical Cerclage
Cervical cerclage is a surgical procedure in which a suture is placed around the cervix to reinforce it and prevent premature dilation, primarily used for cervical insufficiency and prevention of preterm birth.
Indications
There are three recognized indications, each with its own timing and evidence base:
| Indication | Trigger | Timing |
|---|---|---|
| History-Indicated (HIC) | Prior painless cervical dilation leading to 2nd-trimester loss; or prior ultrasound-indicated cerclage with delivery ≤32 weeks | 11-15 weeks gestation |
| Ultrasound-Indicated | Singleton with prior preterm birth (16-36 wks) AND current transvaginal cervical length <25 mm | Before 24 weeks |
| Physical Exam-Indicated | Painless cervical dilation found on exam, <24 weeks, no labor/rupture/infection | Before 24 weeks |
A transabdominal cerclage is reserved for patients with: prior failed history-indicated transvaginal cerclage with early preterm birth <33 weeks, or those with little to no accessible vaginal cervix due to mullerian anomaly or prior cervical surgery.
- Creasy & Resnik's Maternal-Fetal Medicine, p. 890
Absolute Contraindications
- Non-viable pregnancy
- Unexplained vaginal bleeding
- Ruptured membranes
- Active preterm labor
- Acute cervical or intrauterine infection
Relative Contraindications
-
Known or suspected fetal abnormality
-
Prolapsed fetal membranes through the external os (higher risk of iatrogenic membrane rupture)
-
Placenta previa with cervical dilation
-
Pfenninger and Fowler's Procedures for Primary Care, p. 932
Pre-Procedure Work-Up
- Confirm viable intrauterine pregnancy by ultrasound
- Screen for cervical infection (gonorrhea, chlamydia) - treat before proceeding
- Consider amniocentesis for exam-indicated and ultrasound-indicated cases to rule out subclinical infection
- Perioperative indomethacin is used for exam-indicated cerclage; consider for ultrasound-indicated
- Fetal heart rate monitoring before and after the procedure
Equipment
- Bladder catheter
- Weighted vaginal speculum
- Deaver or right-angle retractor
- Ring forceps
- No. 5 Mersilene band (non-absorbable) with curved needle - the standard suture material. Do not confuse with 5-0 suture
- Pickups (e.g., Russian forceps)
- Metzenbaum scissors
- Needle driver
Anesthesia
General endotracheal or spinal anesthesia is standard. Local or paracervical block is avoided due to concern for alteration in uterine blood flow. The procedure is done in an operating room as an outpatient same-day procedure.
Procedure - McDonald Cerclage (Transvaginal, Most Common)
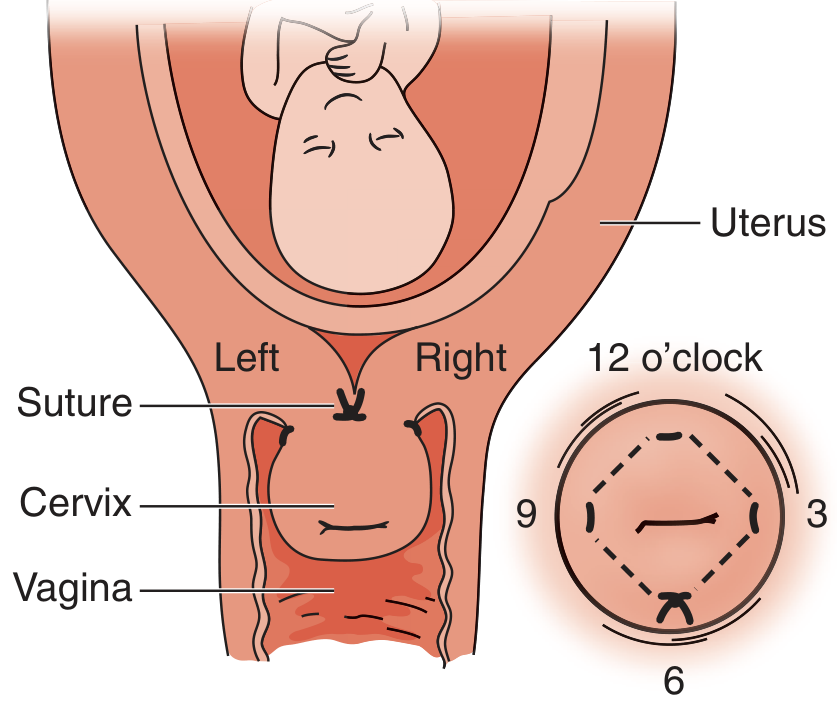
Figure: Cervical cerclage and relevant anatomy. The suture is placed as a pursestring with the knot resting at the 6 o'clock position in the posterior vagina.
Step-by-step:
- Obtain informed consent; document intrauterine fetal viability.
- Administer general or regional anesthesia.
- Position the patient in dorsal lithotomy; prep and drape in sterile fashion.
- Drain the bladder (a Foley catheter is not mandatory).
- Place a weighted speculum in the posterior vagina.
- Insert a Deaver or right-angle retractor anteriorly for exposure; have an assistant hold it carefully to avoid bladder injury.
- Grasp the anterior lip of the cervix with ring forceps and displace it superiorly.
- Start at the 6 o'clock position - place the first bite at the mid-portion of the cervix at the cervicovaginal junction (equidistant between the ectocervix and the vaginal reflection). Pass the needle through mid-cervical stroma - do not enter the cervical canal. Direct needle toward 3 o'clock.
- Proceed counterclockwise (clockwise if left-handed): pass suture from 6 o'clock → exit at 3 o'clock → reinsert → exit at 12 o'clock → reinsert → exit at 9 o'clock → reinsert → exit back at 6 o'clock.
- Cinch down the suture as a pursestring, without drawing too tightly. Tie with three knots at 6 o'clock, leaving tails long enough to be grasped for later removal.
- Inspect for bleeding. Remove weighted speculum and ring forceps.
- Transfer to recovery with fetal monitoring to confirm viability.
Common error: Placing the suture too shallowly - it will tear out when tightened. Ensure each bite passes through mid-cervical stroma.
- Pfenninger and Fowler's Procedures for Primary Care, p. 932-933
Operative Note Key Points
Document: procedure type (McDonald), suture type and size, anesthesia used, suture location, number of knots, and estimated blood loss. A diagram is helpful. File a copy in the pregnancy record.
Postoperative Care
- Observe on fetal monitor post-procedure before discharge
- Acetaminophen is usually adequate for pain control
- Antibiotics are not routinely recommended; tocolytics have no proven benefit
- Pelvic rest: no vaginal intercourse for at least 1 week (often for the entire pregnancy)
- Limit physical activity for at least 1 week
- Expect possible significant vaginal discharge for weeks after the procedure
- Increased frequency of prenatal visits for the remainder of pregnancy
- Bed rest is NOT recommended (as per the perioperative considerations table)
Cerclage Removal
- Routine removal at 37 weeks in the office setting
- Technique: place speculum, grasp the knot with pickups (e.g., Russian forceps), elevate the knot, cut with Metzenbaum scissors, and remove
- If removal is difficult, proceed to the operating room - do not force it in the office
- If preterm labor occurs and tocolysis fails, remove the cerclage promptly to avoid cervical laceration
Complications
| Complication | Notes |
|---|---|
| Rupture of membranes | Up to 65% within 2 weeks (emergent cerclage) |
| Chorioamnionitis | Up to 30% (emergent/urgent cases) |
| Suture displacement | - |
| Uterine rupture | Rare |
| Maternal septicemia | - |
| Preterm labor and delivery | - |
| Fetal loss | - |
Urgent or emergent cerclage carries significantly higher complication rates. Scheduled, elective cerclage with clear indications is preferred.
Evidence Summary
-
Cochrane review: overall cerclage use reduced risk of early and late preterm birth (average RR = 0.77; 95% CI 0.66-0.89)
-
HIC benefit is primarily seen in women with 3 or more second-trimester losses or early preterm births
-
For patients with a prior failed transvaginal HIC: transabdominal cerclage is superior to repeat transvaginal for prevention of preterm birth <32 weeks (one RCT)
-
Cerclage is not beneficial in multiple gestations regardless of history or cervical length
-
Creasy & Resnik's Maternal-Fetal Medicine, p. 890-891
Create a patient education handout on cerclage preoperative instructions and postoperative expectations
Asking for Preferences
Reading File
Running Command
Running Command
Writing File
Running Command
Running Command
Your patient education handout is ready:
Cerclage Patient Education
PDF Document · PDF
Here's what the handout covers, organized in patient-friendly language:
Pre-Operative Section
- What cerclage is and why it's done (plain language explanation)
- Tests needed beforehand: ultrasound, infection screening, possible amniocentesis
- Night-before instructions: fasting, hygiene, no jewelry, arrange a driver
- Day-of instructions: medications, clothing, what to bring
- What to expect in the operating room (anesthesia type, positioning, how the stitch is placed)
Post-Operative Section
- Side-by-side table: first 24-48 hours vs. first week expectations
- Ongoing pregnancy expectations (no routine bed rest, increased discharge, follow-up visits)
- Cerclage removal at 37 weeks - how it's done in the office
- Risks reminder table (membranes, infection, preterm labor, bleeding)
- Prominent red/orange warning box listing emergency signs requiring immediate care
- FAQ section (work, travel, whether cerclage is guaranteed to work, C-section)
- Fillable contact block for the care team's details
The layout uses a teal color scheme with clear section headers, designed to be readable and printable on standard letter paper. Let me know if you'd like any content changes, a different language level, or additional sections.
Create a patient education handout on cerclage preoperative instructions and postoperative expectations
Asking for Preferences
Running Command
The file from your previous request is still available - no need to regenerate it:
Cerclage Patient Education
PDF Document · PDF
The handout covers:
- Pre-op: What cerclage is, required tests (ultrasound, infection screening, possible amniocentesis), fasting/hygiene/night-before instructions, day-of checklist, and what to expect in the OR
- Post-op: First 24-48 hours vs. first week expectations (side-by-side table), ongoing pregnancy guidance, cerclage removal at 37 weeks
- Safety: Emergency warning box (bleeding, fever, ruptured membranes, contractions), risks table, FAQ section
- Contact block: Fillable fields for provider name, phone, after-hours line, and next appointment
Let me know if you'd like any changes - different reading level, additional sections, a different language, or a logo/clinic name added.
Write a consent for cervical cerclage procedure
Asking for Preferences
Running Command
Writing File
Running Command
Running Command
Your consent form is ready:
Cerclage Informed Consent
PDF Document · PDF
The form is structured as a complete medicolegal consent document with 12 numbered sections:
| Section | Contents |
|---|---|
| 1. Patient Information | Fillable fields for name, DOB, MRN, gestational age, surgeon, date, facility |
| 2. Nature of the Procedure | Plain-language description of McDonald, Shirodkar, and transabdominal techniques |
| 3. Indication | Checkbox list covering all four recognized indications (history, ultrasound, exam, prior failed cerclage) |
| 4. Expected Benefits | Evidence summary including Cochrane RR ~0.77; specifies who benefits most; notes no benefit in twins |
| 5. Material Risks | Table of 11 risks with approximate frequencies (e.g., membrane rupture up to 65% in emergent cases, chorioamnionitis up to 30%) |
| 6. Alternatives | Progesterone, pessary, transabdominal cerclage, expectant management, bed rest |
| 7. Consequences of non-treatment | Risk of preterm birth and neonatal morbidity if cerclage is declined |
| 8. Anesthesia | Notes spinal/general anesthesia; separate anesthesia consent required |
| 9. Additional procedures | Blanket authorization for unforeseen intraoperative interventions |
| 10. Patient Declaration | Six checkbox acknowledgements covering understanding, Q&A, right to withdraw, and photo consent |
| 11. Interpreter box | Language assistance declaration with checkboxes |
| 12. Signatures | Patient/LAR block, witness block, physician attestation, and a separate consent revocation section |
Note: This is a clinical template. Have your institution's legal or risk management team review it for local regulatory compliance before use.
Show some real videos of Mcdonald stitch for cervical circlage
Searching the Web
McDonald cervical cerclage procedure video site:youtube.com
Here are real surgical videos of the McDonald cervical cerclage technique, all on YouTube:
1. "Art of Cerclage - McDonald Cerclage" - Dr. Sara Rahman
294K+ views - One of the most-watched and highly regarded cerclage videos available. Detailed step-by-step technique.
Watch on YouTube
2. "Cervical Cerclage: McDonald Procedure"
A clean surgical video demonstrating the purse-string suture placement at the cervicovaginal junction with clear visualization of the steps.
Watch on YouTube
3. "Cervical Cerclage (McDonald's Procedure)" - Prophylactic + Therapeutic
A real case - prophylactic and therapeutic cerclage in a patient with short cervical length (2.3 cm) at 18 weeks gestation. Good clinical context.
Watch on YouTube
4. "McDonald Stitch Application - Cervical Cerclage Insertion Technique"
Covers the purpose of cerclage, types, technique, and risks - useful for understanding the full context alongside watching the procedure.
Watch on YouTube
5. "Cervical Encirclage - McDonald Procedure"
Another real surgical recording of the McDonald technique.
Watch on YouTube
6. "Cervical Cerclage - McDonald's Technique" - Dr. Shilpa GB
A real case in a twin pregnancy at 16 weeks - useful to see how the technique is applied in a higher-risk scenario.
Watch on YouTube
Note: I cannot embed or play videos directly here - clicking each link will open YouTube. For learning purposes, the Dr. Sara Rahman "Art of Cerclage" video is particularly recommended given its high view count and detailed narration.
This is a shared conversation. Sign in to Orris to start your own chat.