Hii
Explain macrolides and Aminoglycoside
Macrolides and Aminoglycosides
MACROLIDES
Structure
Mechanism of Action
- Bind reversibly to the 23S rRNA of the 50S ribosomal subunit
- This blocks polypeptide chain elongation
- Result: bacteriostatic activity
Spectrum of Activity
| Organism Type | Susceptibility |
|---|---|
| Gram-positive bacteria | Active |
| Mycoplasma, Legionella, Chlamydia | Active (pulmonary infections) |
| Campylobacter spp. | Active |
| Most gram-negative bacteria | Resistant |
| Mycobacterium avium complex | Active (azithromycin, clarithromycin) |
Clinical Uses
- Respiratory tract infections (pneumonia, especially atypical)
- Alternative to penicillin in penicillin-allergic patients (gram-positive infections)
- Mycoplasma, Legionella, Chlamydia pneumonia
- M. avium complex in HIV patients
Resistance Mechanisms
- Methylation of 23S rRNA - most common; prevents antibiotic binding
- Enzymatic inactivation - by esterases, phosphorylases, glycosidases
- Mutations in 23S rRNA or ribosomal proteins
Note: Erythromycin and clindamycin both induce rRNA methylation, so cross-resistance between macrolides and clindamycin is observed.
Key Drugs
- Erythromycin - original, narrow use now due to GI side effects
- Azithromycin - long half-life, once-daily dosing, excellent tissue penetration
- Clarithromycin - better bioavailability, used in H. pylori triple therapy
AMINOGLYCOSIDES
Structure
- Natural sources: Streptomycin, neomycin, kanamycin, tobramycin from Streptomyces; gentamicin and sisomicin from Micromonospora
- Synthetic: Amikacin (from kanamycin), netilmicin (from sisomicin)
Mechanism of Action
- Drug crosses the outer membrane, cell wall, and cytoplasmic membrane via an aerobic, energy-dependent transport process
- Binds irreversibly to 30S ribosomal proteins
- Two consequences:
- Misreading of mRNA → aberrant/nonfunctional proteins
- Premature ribosome release from mRNA → interruption of protein synthesis
- Result: bactericidal (due to irreversible binding)
Spectrum of Activity
| Organism Type | Susceptibility |
|---|---|
| Gram-negative rods (Enterobacteriaceae, Pseudomonas, Acinetobacter) | Primary targets |
| Gram-positive (with cell-wall agent combo) | Active synergistically |
| Anaerobes | Resistant (transport requires oxygen) |
| Streptococci/Enterococci alone | Resistant (poor cell wall penetration) |
Clinical Uses
- Serious gram-negative infections (sepsis, pneumonia, UTI)
- Synergistic therapy: aminoglycoside + penicillin/ampicillin/vancomycin for enterococcal or streptococcal endocarditis
- Streptomycin: tuberculosis, tularemia
- Amikacin: reserved for gentamicin/tobramycin-resistant organisms
- Tobramycin: slightly more active than gentamicin against Pseudomonas
Resistance Mechanisms
- Enzymatic modification - most common:
- Phosphotransferases (APHs)
- Adenyl-transferases (ANTs)
- Acetyltransferases (AACs) These act on the amino and hydroxyl groups of the drug.
- Mutation of ribosomal binding site (uncommon - requires mutation of multiple rRNA gene copies)
- Decreased uptake into the cell (occasionally seen in Pseudomonas)
- Active efflux (rare, only in gram-negatives)
Toxicity (clinically important)
- Nephrotoxicity - dose-dependent, reversible; monitor renal function
- Ototoxicity - vestibular and/or cochlear damage; can be irreversible
- Neuromuscular blockade - rare, seen with high doses
Side-by-Side Comparison
| Feature | Macrolides | Aminoglycosides |
|---|---|---|
| Ribosome target | 50S (23S rRNA) | 30S |
| Binding | Reversible | Irreversible |
| Bactericidal/static | Bacteriostatic | Bactericidal |
| Primary spectrum | Gram-positive, atypicals | Gram-negative rods |
| Anaerobe coverage | Some | None |
| Key toxicity | GI upset, QT prolongation | Nephro/ototoxicity |
| Resistance (main) | 23S rRNA methylation | Enzymatic modification |
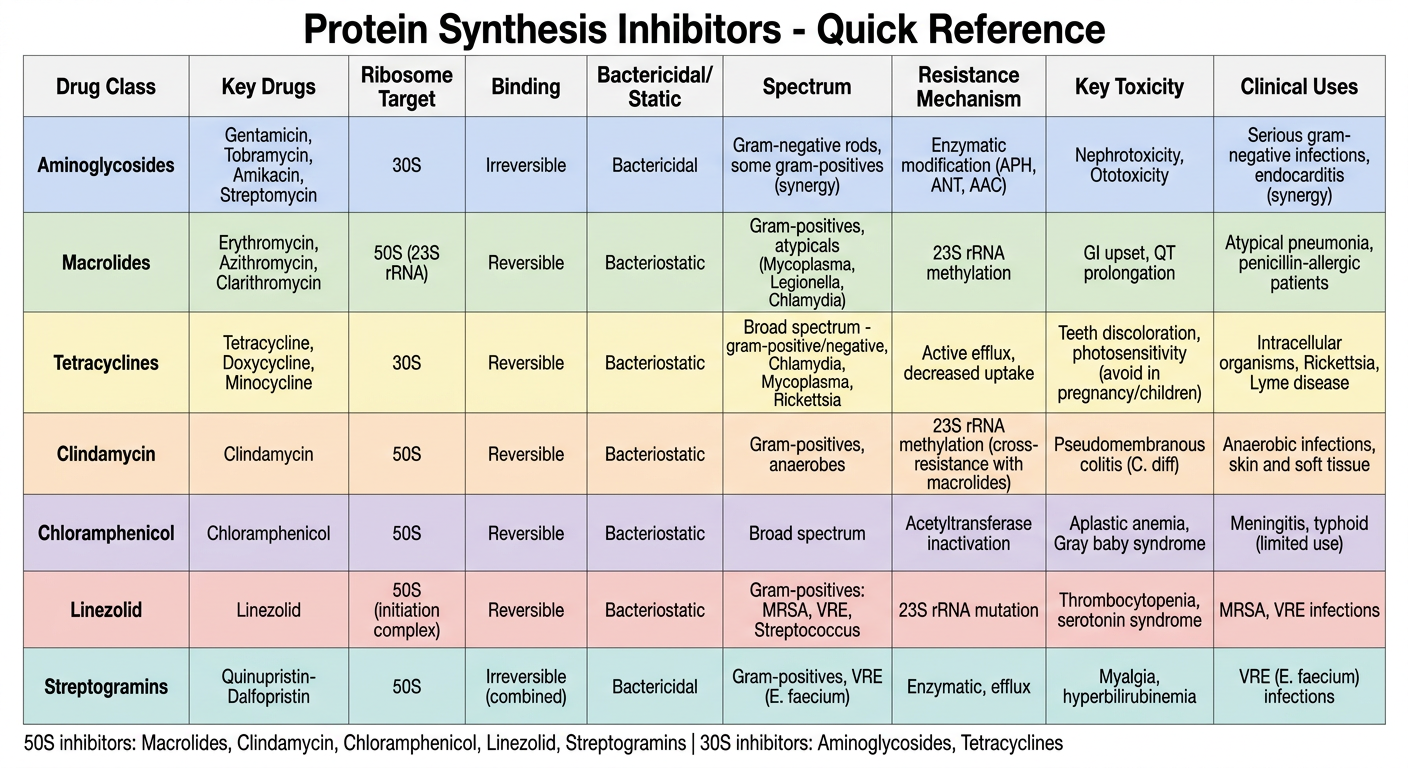
Generate a quick reference chart comparing protein synthesis inhibitors
A clean, professional medical quick reference chart titled "Protein Synthesis Inhibitors - Quick Reference" comparing the following antibiotic classes in a well-organized table format with color-coded rows: Columns: Drug Class | Key Drugs | Ribosome Target | Binding | Bactericidal/Static | Spectrum | Resistance Mechanism | Key Toxicity | Clinical Uses Rows (each row in a distinct soft color): 1. Aminoglycosides (blue row) | Gentamicin, Tobramycin, Amikacin, Streptomycin | 30S | Irreversible | Bactericidal | Gram-negative rods, some gram-positives (synergy) | Enzymatic modification (APH, ANT, AAC) | Nephrotoxicity, Ototoxicity | Serious gram-negative infections, endocarditis (synergy) 2. Macrolides (green row) | Erythromycin, Azithromycin, Clarithromycin | 50S (23S rRNA) | Reversible | Bacteriostatic | Gram-positives, atypicals (Mycoplasma, Legionella, Chlamydia) | 23S rRNA methylation | GI upset, QT prolongation | Atypical pneumonia, penicillin-allergic patients 3. Tetracyclines (yellow row) | Tetracycline, Doxycycline, Minocycline | 30S | Reversible | Bacteriostatic | Broad spectrum - gram-positive/negative, Chlamydia, Mycoplasma, Rickettsia | Active efflux, decreased uptake | Teeth discoloration, photosensitivity (avoid in pregnancy/children) | Intracellular organisms, Rickettsia, Lyme disease 4. Clindamycin (orange row) | Clindamycin | 50S | Reversible | Bacteriostatic | Gram-positives, anaerobes | 23S rRNA methylation (cross-resistance with macrolides) | Pseudomembranous colitis (C. diff) | Anaerobic infections, skin and soft tissue 5. Chloramphenicol (purple row) | Chloramphenicol | 50S | Reversible | Bacteriostatic | Broad spectrum | Acetyltransferase inactivation | Aplastic anemia, Gray baby syndrome | Meningitis, typhoid (limited use) 6. Linezolid (red row) | Linezolid | 50S (initiation complex) | Reversible | Bacteriostatic | Gram-positives: MRSA, VRE, Streptococcus | 23S rRNA mutation | Thrombocytopenia, serotonin syndrome | MRSA, VRE infections 7. Streptogramins (teal row) | Quinupristin-Dalfopristin | 50S | Irreversible (combined) | Bactericidal | Gram-positives, VRE (E. faecium) | Enzymatic, efflux | Myalgia, hyperbilirubinemia | VRE (E. faecium) infections Footer note: "50S inhibitors: Macrolides, Clindamycin, Chloramphenicol, Linezolid, Streptogramins | 30S inhibitors: Aminoglycosides, Tetracyclines" Use a clean white background, bold column headers in dark navy, alternating soft pastel row colors, professional medical font, clear borders on all cells.
- Only aminoglycosides bind irreversibly and are bactericidal among the common 30S/50S inhibitors
- Only aminoglycosides are useless against anaerobes (need O₂ for transport)
- Linezolid is unique - it blocks the initiation complex (not elongation)
- Cross-resistance between macrolides and clindamycin (same 23S methylation mechanism)