CRRT
Reading File
Finding Sources
Searching PubMed
"continuous renal replacement therapy" AND "acute kidney injury"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have everything needed for a comprehensive CRRT overview. Here is the full response:
Continuous Renal Replacement Therapy (CRRT)
Definition and Core Concept
CRRT is a form of renal replacement therapy (RRT) that removes fluid and solutes continuously over 24 hours, using slow, pump-driven extracorporeal circuits. Unlike intermittent hemodialysis (IHD), which operates at high blood flow rates (200-350 mL/min) over 3-4 hours, CRRT uses blood flow rates of 100-200 mL/min and runs around the clock. This slower pace translates to fewer abrupt hemodynamic changes and more precise fluid management. Its efficacy depends on minimal interruption - clotting, procedures, or transport all degrade effective delivered dose.
- Brenner and Rector's The Kidney, p. 2817
- Fischer's Mastery of Surgery, p. 228
Modalities
All contemporary CRRT is venovenous (pump-driven). The original arteriovenous circuits have been largely abandoned due to complications from prolonged arterial cannulation and dependence on MAP-CVP gradient for flow.
| Modality | Mechanism | Solute Removal |
|---|---|---|
| SCUF (Slow Continuous Ultrafiltration) | Convection only | Fluid removal; minimal solute |
| CVVH (Continuous Venovenous Hemofiltration) | Convection | Small + medium MW solutes |
| CVVHD (Continuous Venovenous Hemodialysis) | Diffusion | Small solutes (urea, creatinine) |
| CVVHDF (Continuous Venovenous Hemodiafiltration) | Convection + Diffusion | Broadest spectrum |
Although convective therapies (CVVH, CVVHDF) provide enhanced clearance of higher molecular weight solutes compared with diffusive therapies at equal urea clearance, no clear clinical benefit has been demonstrated for CVVH or CVVHDF versus CVVHD.
Indications
CRRT is preferred over IHD in the following settings:
- Hemodynamic instability - the primary clinical driver; patients on vasopressors tolerate CRRT better than IHD
- Severe fluid overload requiring continuous, titrated removal
- Cerebral edema - avoids rapid osmotic shifts seen with IHD
- Continuous metabolic control - hyperammonemia, lactic acidosis, severe hyperkalemia requiring sustained management
- Need for large-volume IV medications (nutrition, antibiotics, blood products) in a fluid-restricted patient
KDIGO guidelines recommend using CRRT and IHD in a complementary fashion: CRRT for hemodynamically unstable patients, IHD for stable patients, with modality switching as the clinical picture evolves.
Dosing and Intensity
Dose is expressed as effluent volume per kg body weight per hour (mL/kg/hr) - the sum of ultrafiltrate + dialysate flow rates.
Two landmark RCTs established the current standard:
- ATN Trial (n=1124): Intensive (35 mL/kg/hr CVVHF) vs. less intensive (20 mL/kg/hr). 60-day mortality: 53.6% vs. 51.5% (P=.47) - no benefit from higher intensity.
- RENAL Trial (n=1508): CVVHF at 40 vs. 25 mL/kg/hr. 90-day mortality: 44.7% in both arms (P=.99).
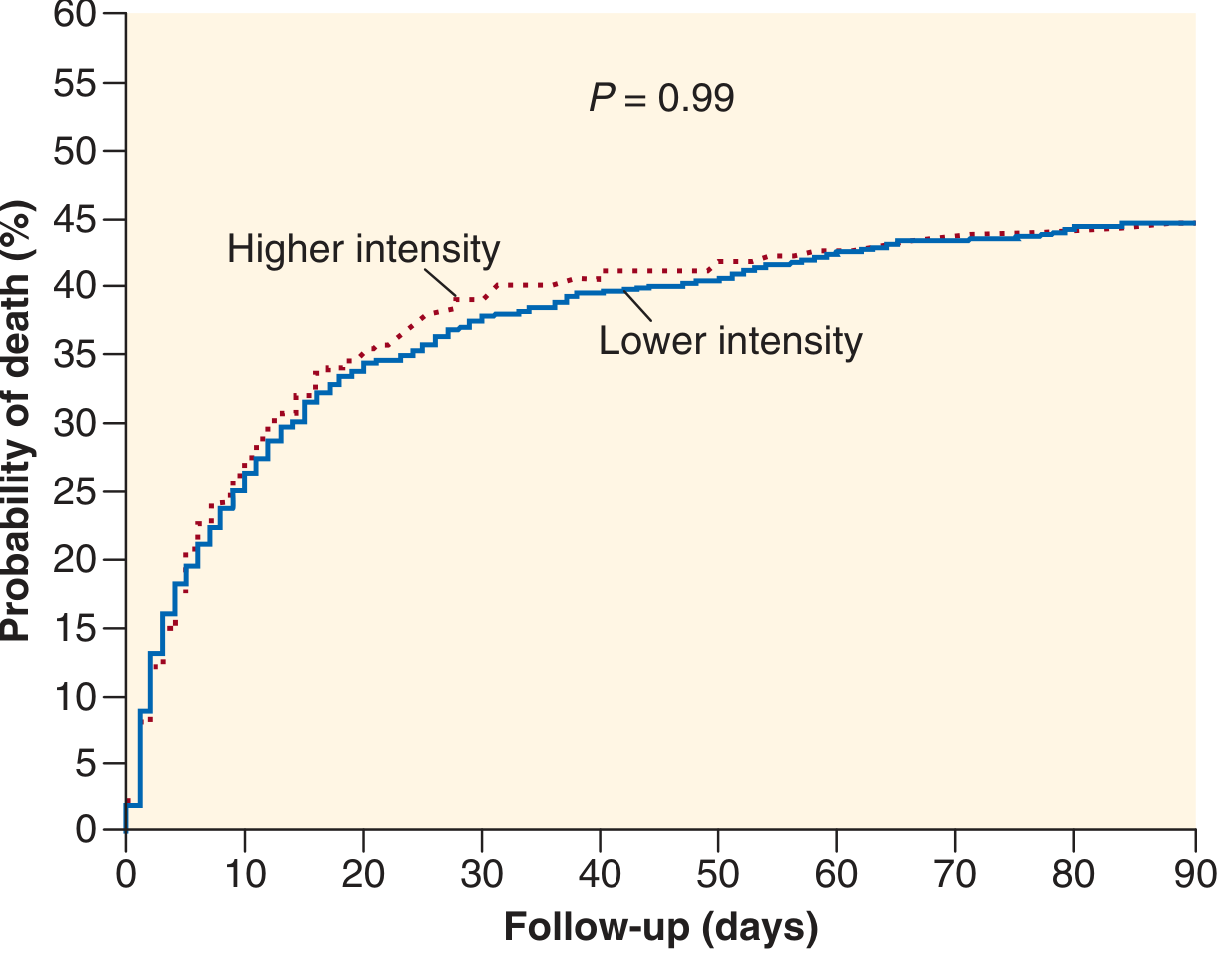
RENAL Trial Kaplan-Meier curve: 90-day mortality was identical (44.7%) regardless of CRRT intensity. From Bellomo et al., N Engl J Med 2009.
KDIGO recommendation: Deliver 20-25 mL/kg/hr effluent volume. Prescribe slightly higher (e.g., 25-30 mL/kg/hr) to account for treatment interruptions, since the delivered dose is invariably less than the prescribed dose.
A 2026 meta-analysis (PMID 41896891) confirmed that lower-dose CRRT does not worsen outcomes compared with standard dosing.
Anticoagulation
Anticoagulation prevents clotting of the extracorporeal circuit, which degrades filter life and reduces delivered dose.
Regional Citrate Anticoagulation (RCA) - Preferred at most centers
- Citrate is infused pre-filter, chelating ionized calcium (target circuit iCa: 0.25-0.45 mmol/L), which blocks the clotting cascade
- A concurrent systemic calcium infusion maintains normal serum calcium
- Advantages: Lower bleeding risk than heparin; longer filter life
- Complications:
- Metabolic alkalosis (citrate converted to bicarbonate in liver) - correct by reducing dialysate/replacement solution bicarbonate
- Citrate accumulation in liver failure: manifests as wide anion gap + hypocalcemia (total Ca high, ionized Ca low - the "citrate lock" sign)
- Can be used cautiously in liver failure with careful monitoring
Unfractionated Heparin (UFH)
- Used when RCA is contraindicated or for patients who need systemic anticoagulation anyway (e.g., mechanical valve, DVT)
- Monitor aPTT; bleeding risk is the main concern
Argatroban
- Drug of choice in heparin-induced thrombocytopenia (HIT)
- Systemic infusion
No Anticoagulation
- Feasible, especially if coagulopathic (cirrhosis, DIC, post-surgery)
- Expect more frequent filter clotting and circuit changes
- Strategies to prolong filter life without anticoagulation: increase blood flow (≥250 mL/min), use pre-filter replacement fluid position in CVVH
CRRT vs. IHD vs. SLED - Comparison
| Feature | IHD | SLED/PIRRT | CRRT |
|---|---|---|---|
| Duration | 3-4 hours | 8-15 hours | 24 hours continuous |
| Blood flow rate | 200-350 mL/min | 100-200 mL/min | 100-200 mL/min |
| Hemodynamic stability | Poorest | Intermediate | Best |
| Fluid removal | Rapid (limited) | Moderate | Precise hourly titration |
| Anticoagulation | Often avoidable | Often avoidable | Usually needed |
| Cost | Lowest | Low | Highest |
| Staff requirements | Lower | Moderate | High (ICU nursing) |
| Rapid solute removal (hyperK, toxins) | Best | Adequate | Not ideal |
| Nursing familiarity | Widest | Moderate | Specialized |
Survival: No RCT has shown a mortality advantage of CRRT over IHD. A large multicenter trial (Hemodiafe study, n=359) showed 60-day survival of 31.5% (IHD) vs. 32.6% (CRRT), P=.98.
Kidney recovery: Some observational data and a meta-analysis suggest CRRT recipients who survive the acute phase may have a lower risk of long-term dialysis dependence (~25% lower at 2 years in one Ontario cohort study). This potential nephroprotective benefit likely explains why CRRT remains preferred in hemodynamically unstable patients despite equal mortality data.
Fluid Balance Management
Volume overload is nearly universal in critically ill AKI patients. CRRT allows hourly ultrafiltration adjustments - a key advantage over IHD.
Practical example:
- Goal: net fluid removal of 50 mL/hr in an anuric patient
- Inputs in the preceding hour: 30 mL PN + 40 mL infusions = 70 mL in; 30 mL drain out = net +40 mL
- Prescribed ultrafiltration volume = 40 (net balance) + 50 (target removal) = 90 mL/hr
Persistent fluid overload during CRRT is independently associated with higher mortality. Effective volume assessment tools include bedside ultrasound (IVC diameter, lung B-lines) and bioimpedance analysis.
Drug Dosing During CRRT
CRRT significantly alters pharmacokinetics. Key principles:
- Protein binding: Only unbound drug is removed. Protein binding >80% markedly reduces CRRT clearance (e.g., vancomycin ~50% bound - moderate removal; ceftriaxone ~95% bound - minimal removal)
- Volume of distribution (Vd): High Vd (>1 L/kg) = low CRRT removal (drug is tissue-distributed, not in plasma)
- Molecular weight: High-flux filters remove drugs up to 250 kDa
- Effluent rate dependence: CVVH drug clearance ≈ ultrafiltration rate; CVVHDF adds diffusive clearance on top
Clinical rule of thumb:
- CRRT clearance <25% of total body clearance → no dosage adjustment needed
- CRRT clearance 25-50% of total body clearance → supplement with loading dose; use CrCl 30-50 mL/min equivalent for maintenance dosing
- Filter age matters: protein accumulation on the membrane reduces clearance over time
Antibiotics of particular concern: Aminoglycosides, vancomycin, beta-lactams, carbapenems - all require therapeutic drug monitoring during CRRT because standard dosing tables were derived from old, less efficient filters and may be dangerously underdosing in modern practice.
Complications and Monitoring
| Complication | Cause | Monitoring |
|---|---|---|
| Hypothermia | Blood cooling in circuit | Inline blood warmer; temperature monitoring |
| Electrolyte losses | Phosphate poorly removed by IHD but well-removed by CRRT | Daily phosphate, magnesium, potassium |
| Hypocalcemia | Citrate anticoagulation | Ionized calcium q4-6h during citrate |
| Metabolic alkalosis | Citrate metabolism | Bicarbonate level; adjust replacement fluid |
| Citrate toxicity | Impaired liver metabolism | Total Ca/ionized Ca ratio >2.5 is the warning sign |
| Filter clotting | Circuit activation of coagulation | Monitor filter pressure drop, flow resistance |
| Bleeding | Over-anticoagulation | aPTT, anti-Xa (if LMWH) |
Key Takeaways
- CRRT is the preferred modality in hemodynamically unstable ICU patients with AKI.
- Target effluent dose: 20-25 mL/kg/hr (KDIGO). Prescribe slightly more to account for downtime.
- Higher doses (35-45 mL/kg/hr) do NOT improve survival - definitively shown by ATN and RENAL trials.
- Regional citrate anticoagulation is the preferred strategy at most centers; watch for citrate accumulation in liver failure.
- CRRT vs. IHD: equal mortality, but CRRT may be nephroprotective in survivors.
- Drug dosing must be reassessed; many antibiotic dosing guidelines are outdated for modern high-efficiency CRRT circuits.
Sources: Brenner and Rector's The Kidney (9th ed.), Fischer's Mastery of Surgery (8th ed.), Brenner and Rector's The Kidney block 34 (pharmacokinetics), Washington Manual of Medical Therapeutics. RENAL Trial: Bellomo et al., N Engl J Med 2009. ATN Trial: Palevsky et al., N Engl J Med 2008. Recent meta-analysis (PMID 41896891, Crit Care 2026).
This is a shared conversation. Sign in to Orris to start your own chat.