
IMG-20260620-WA0058.jpg
Diagnosis, loose stools for more than 3 week along with blood
Reading File
Finding Sources
Finding Sources
Searching PubMed
"Entamoeba histolytica" AND "amoebic dysentery" AND treatment
Reading File
Reading File
Searching PubMed
"Entamoeba histolytica" AND colitis AND treatment
Reading File
Loading Image
Reading File
I now have comprehensive information to provide a thorough clinical analysis. Here is the full report:
Clinical Analysis - Lab Report for Shefeeq, 38M
Lab Findings Summary (from report)
| Test | Result | Significance |
|---|---|---|
| Stool Colour | Reddish | Fresh blood present |
| Consistency | Semi-solid (loose) | Abnormal |
| Mucus | Present/HPF | Mucosal irritation |
| Ova | Nil | No helminth infection |
| Cyst | EH Cyst Present | Entamoeba histolytica confirmed |
| RBC (stool) | 60-65/HPF | Significant - indicates invasive disease |
| Pus Cells (stool) | 25-30/HPF | Active inflammation |
Diagnosis: Amebic Dysentery (Invasive Intestinal Amebiasis)
The combination of:
- EH Cyst (Entamoeba histolytica cyst) in stool microscopy
- Bloody, semi-solid stools for >3 weeks
- 60-65 RBCs/HPF (very elevated)
- 25-30 Pus cells/HPF
- Mucus present
...is a classic presentation of amebic colitis/dysentery caused by Entamoeba histolytica.
Life Cycle and Pathophysiology
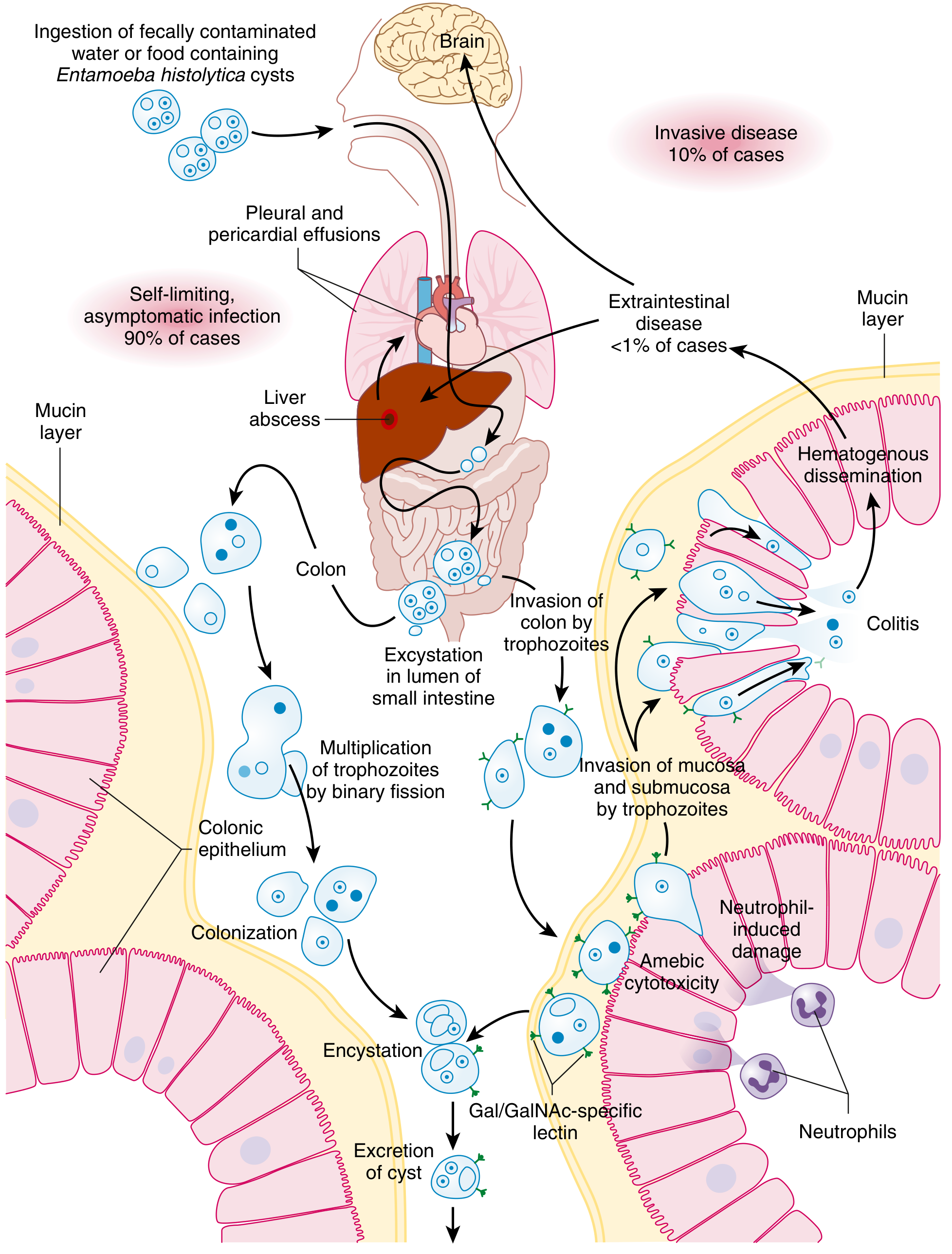
As shown above, E. histolytica cysts are ingested through fecal-oral contamination (contaminated water/food). In the colon, trophozoites invade the mucosa using the Gal/GalNAc lectin, causing direct cytotoxicity and neutrophil-induced mucosal damage, producing the characteristic flask-shaped ulcers.
From Goldman-Cecil Medicine: "Diarrhea with mucus or visible or microscopic blood in a patient with E. histolytica infection is the definition of amebic dysentery or colitis. The onset of symptoms is typically gradual during a period of 3 or 4 weeks after infection, with abdominal tenderness and increasingly severe diarrhea." This matches this patient's presentation precisely.
Why the Duration Matters (>3 Weeks)
Unlike bacterial dysentery (Shigella, Salmonella) where symptoms typically last only 1-2 days to 1 week, amebic colitis has a characteristically gradual onset over 3-4 weeks - this is a distinguishing feature that fits this patient's timeline exactly.
Important: Confirm Pathogenic vs. Non-pathogenic Species
Note that E. histolytica cysts are morphologically identical to the non-pathogenic E. dispar and E. moshkovskii under routine microscopy. However, given the high RBC count (60-65/HPF) and symptoms, this is almost certainly pathogenic E. histolytica (invasive disease). Ideally, confirmation by:
- Stool antigen detection (ELISA) - sensitivity ~80% for colitis
- Real-time PCR - sensitivity >95%
- Serology (indirect hemagglutination) - useful in invasive disease
Differential Diagnoses to Consider
| Condition | Against |
|---|---|
| Bacterial dysentery (Shigella, Campylobacter) | Typically acute, 1-2 day onset; no EH cyst |
| Inflammatory Bowel Disease (IBD) | No cysts; must rule out infection first |
| Colorectal malignancy | 38-year-old, no family history mentioned; need colonoscopy if no treatment response |
| Balantidium coli | Rare; different cyst morphology |
Treatment (per Goldman-Cecil Medicine)
Step 1 - Treat invasive infection with a nitroimidazole:
| Drug | Dose | Duration | Notes |
|---|---|---|---|
| Tinidazole (preferred) | 2g once daily | 3 days | Fewer side effects, better tolerated than metronidazole |
| Metronidazole | 500-750mg 3x/day | 7-10 days | Standard option |
| Secnidazole | 2g single dose | Single dose | Convenient |
| Ornidazole | 500mg 3x/day | 5 days | Alternative |
Step 2 - Follow with a luminal amebicide (to eliminate residual cysts in the gut lumen, as parasites persist in up to 50% of patients treated with nitroimidazole alone):
- Paromomycin 500mg 3x/day for 7 days (drug of choice)
- OR Diloxanide furoate 500mg 3x/day for 10 days
Tinidazole + Paromomycin is the preferred two-drug regimen for confirmed invasive amebic colitis.
Urine Findings (incidental)
The urine findings (RBC 2-3/HPF, Pus 3-4/HPF, Calcium oxalate crystals 5-6/HPF) are mildly abnormal but likely incidental or dietary (calcium oxalate crystals are common after oxalate-rich foods). No urgent urological concern, but worth monitoring.
Red Flags - Refer/Investigate Urgently If:
- Severe abdominal pain or guarding (toxic megacolon - seen in 0.5% of amebic colitis)
- Right upper quadrant pain or fever - rule out amebic liver abscess (extraintestinal spread, 10x more common in men)
- No improvement after 72 hours of treatment
- Symptoms worsen - consider colonoscopy
Summary
Primary Diagnosis: Amebic Dysentery / Invasive Amebic Colitis (Entamoeba histolytica)
Key Evidence: EH cyst on microscopy + bloody mucoid stools for >3 weeks + RBC 60-65/HPF + Pus 25-30/HPF
Treatment: Tinidazole (2g OD x 3 days) followed by Paromomycin (500mg TDS x 7 days)
Follow-up: Repeat stool examination after treatment to confirm eradication; watch for hepatic spread
Disclaimer: This analysis is for informational purposes only. The treating physician (Dr. Harinath, MBBS MS General Surgery) should make all clinical decisions based on complete history, examination, and judgment.
- Goldman-Cecil Medicine, Chapter 323 (Amebiasis)
- Bailey and Love's Short Practice of Surgery, 28th Edition
This is a shared conversation. Sign in to Orris to start your own chat.