Ca rectum management
Reading File
Finding Sources
Finding Sources
Searching PubMed
rectal cancer management treatment
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have everything needed for a thorough, well-illustrated answer. Let me compile it.
Carcinoma of the Rectum - Management
Background
The rectum spans 12-15 cm from the anorectal ring to the rectosigmoid junction. Rectal cancer refers to tumors at or below the peritoneal reflection. It accounts for approximately 45,000 new diagnoses per year in the US and is uniquely challenging due to the bony pelvis confines and proximity to sphincters, bladder, prostate/vagina, and autonomic nerves. Management requires a multidisciplinary team approach.
Clinical Presentation & Diagnosis
- Most common symptom: Change in bowel habits
- Other features: rectal bleeding, iron deficiency anemia, change in stool caliber, tenesmus (late, suggests invasion), palpable rectal mass
- Diagnosis: Biopsy at endoscopy; complete colonoscopy preferred (3-5% synchronous tumor risk)
- Tumour marker: CEA - not diagnostic but used for prognosis and post-treatment surveillance
- DRE: Assess distance from anal verge, fixity, and sphincter involvement
- Rigid proctoscopy is preferred over flexible endoscopy for measuring distance from anal verge
Staging Workup
Locoregional staging:
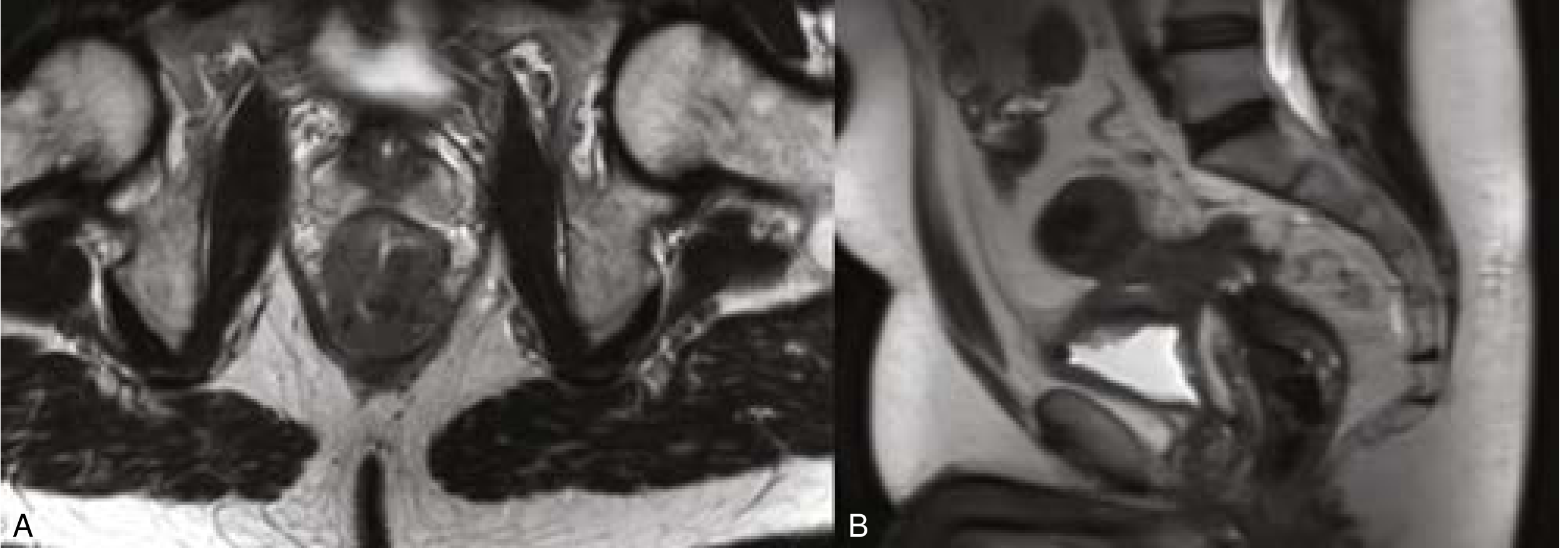
- MRI pelvis (preferred): high-resolution T2-weighted thin-cut sequences for depth of invasion, nodal status, and circumferential resection margin (CRM)
- Endorectal ultrasound (EUS): historically used, now limited due to operator-dependency and poor accuracy with bulky/posterior tumors
- Threatened CRM = tumor within 1 mm on MRI - highly predictive of positive radial margin, poor disease-free and overall survival
Nodal staging on MRI: Nodes suspicious if >9 mm short axis, round shape, irregular borders, heterogeneous signal.
MRI showing T3 tumor (left) and T4 tumor invading bladder (right):
Distant staging:
- CT chest and abdomen (standard)
- MRI abdomen if liver metastasis concern
- PET: not standard; considered for non-diagnostic CT or to confirm solitary metastasis
Staging system: AJCC/UICC TNM 8th edition
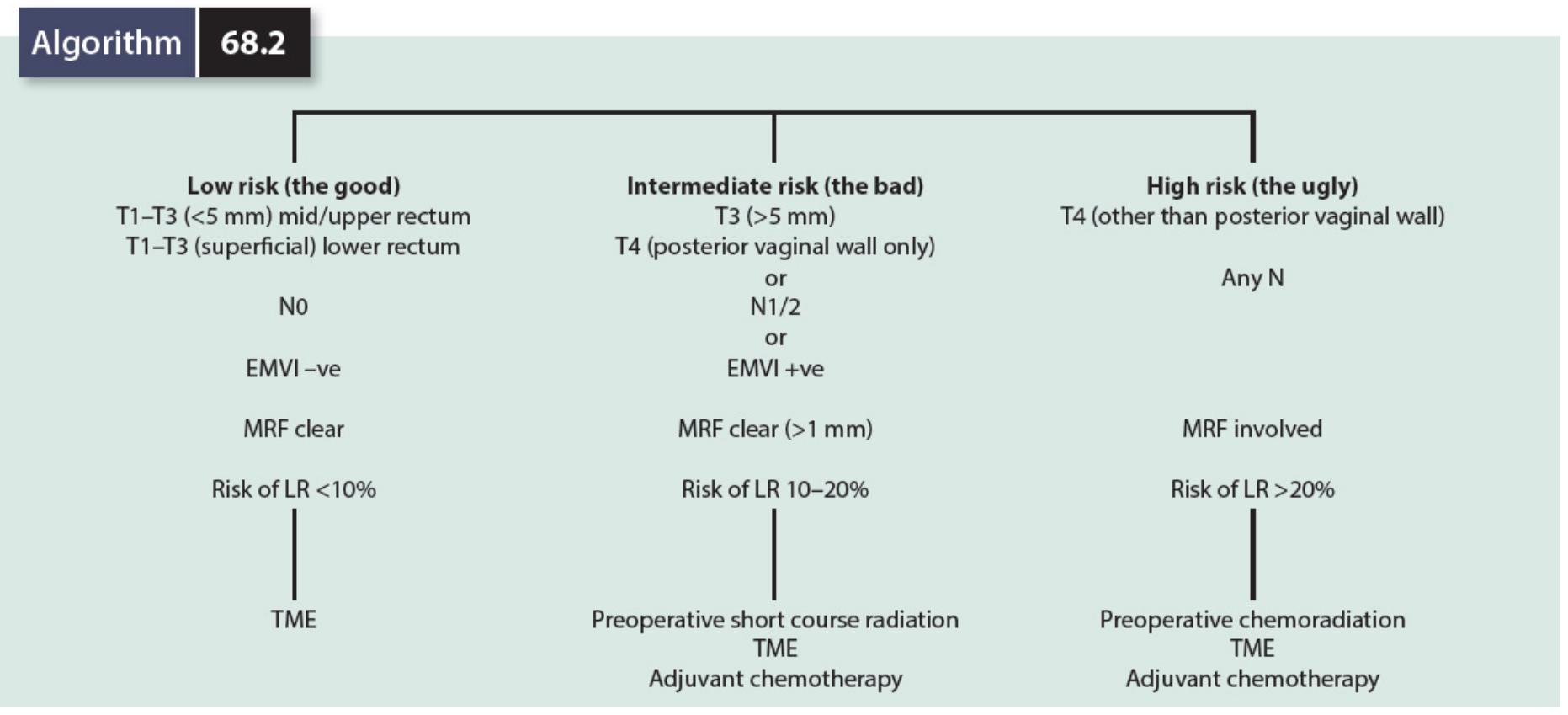
Risk Stratification - "The Good, the Bad, and the Ugly"
| Risk | Criteria | Risk of LR | Treatment |
|---|---|---|---|
| Low ("the good") | T1-T3 (<5 mm) mid/upper rectum; T1-T3 superficial lower rectum; N0; EMVI -ve; MRF clear | <10% | TME alone |
| Intermediate ("the bad") | T3 >5 mm; T4 (posterior vaginal wall only); N1/2; EMVI +ve; MRF clear >1mm | 10-20% | Short-course RT + TME + adjuvant chemo |
| High ("the ugly") | T4 (other than posterior vaginal wall); MRF involved; any N | >20% | Long-course CRT + TME + adjuvant chemo |
(Mulholland & Greenfield's Surgery, 7e)
Neoadjuvant Therapy
Indications: Clinical T3, T4, or node-positive disease (clinical T1-T2 N0 disease does not require neoadjuvant therapy).
Long-Course Chemoradiotherapy (LCRT)
- 45-50 Gy in 25 fractions (1.8-2 Gy/day) + concurrent fluoropyrimidine (5-FU or capecitabine)
- Surgery after 6-10 weeks (8 weeks preferred) - longer delay increases pathologic complete response (pCR) rate
- Standard for high-risk/bulky locally advanced rectal cancer (LARC)
Short-Course Radiotherapy (SCRT)
- 5 Gy x 5 fractions over 5 days
- Surgery within 7-10 days OR delayed 5-12 weeks (delayed preferred - lower complication rate)
- Non-inferior to LCRT for local recurrence, DFS, and OS with less toxicity and lower cost (Polish trial, Trans-Tasman trial)
- Increasingly used in the US; widely used in Europe
Total Neoadjuvant Therapy (TNT) - Current Practice Shift
- Goal: Deliver ALL preoperative systemic therapy + RT before surgery to address micrometastatic disease early
- Radiation given in short or long-course format
- Chemotherapy (FOLFOX) given as induction (before RT) or consolidation (after RT)
- Results in higher pCR rates vs CRT alone; better treatment completion
- NCCN indications for TNT: T4 lesions, T3 with threatened margins, medically inoperable patients; can also consider for T3 without threatened margins and T1-T2 N+ disease
- Early data suggest improved survival vs conventional CRT + surgery + adjuvant chemo
2024 ASCO Guideline (PMID: 39116386) is the most recent evidence-based guideline on management of locally advanced rectal cancer, published in J Clin Oncol Oct 2024 - may update some older textbook recommendations above.
Surgical Management
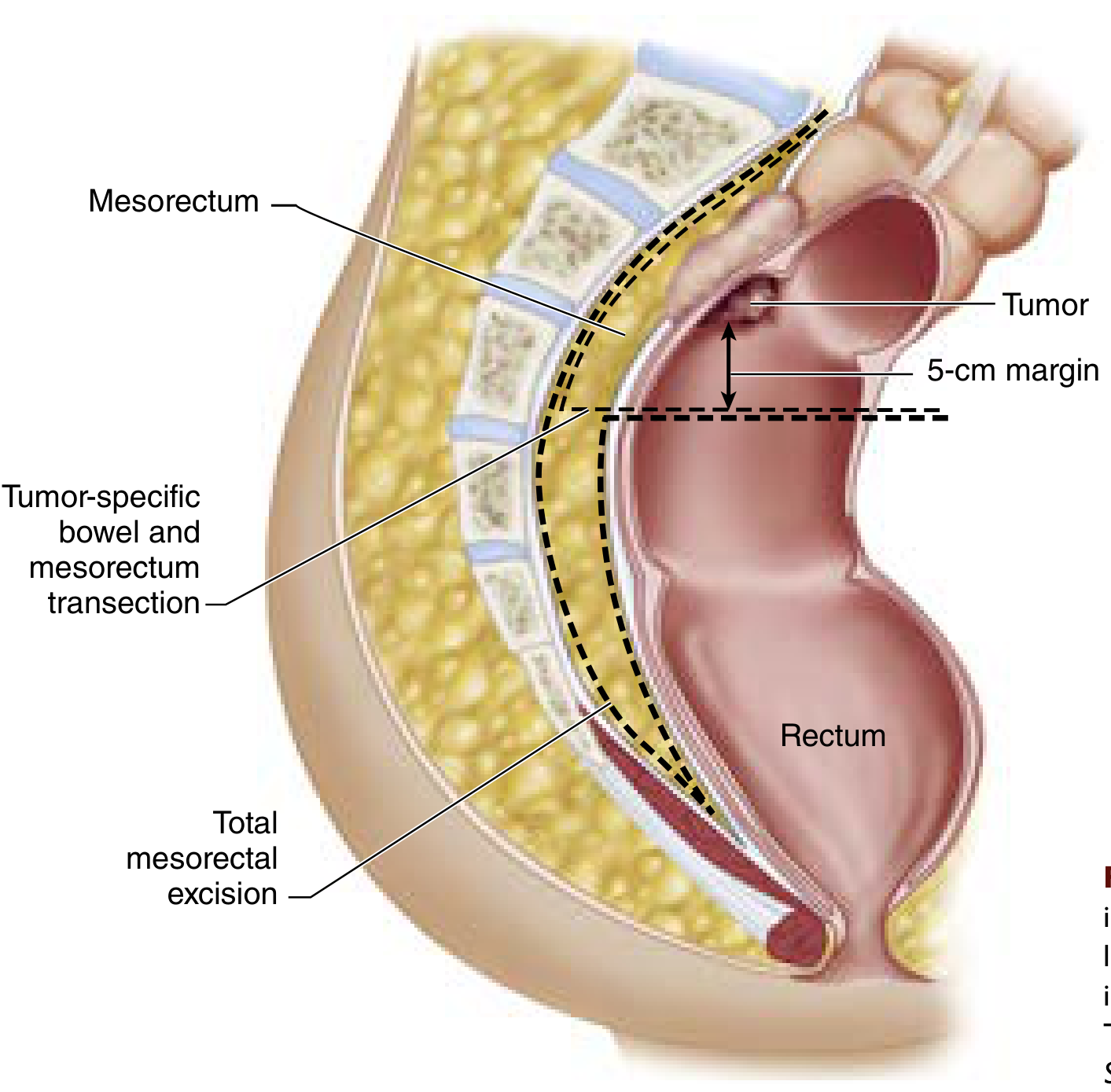
Core Principle: Total Mesorectal Excision (TME)
Defined by Bill Heald in 1982. TME involves sharp dissection within the avascular plane between visceral and parietal layers of endopelvic fascia, ensuring complete excision of the mesorectum with its blood supply, lymphatics, and any tumor deposits.
TME quality grading (pathologic assessment):
- Complete - intact mesorectal fascia
- Near-complete - small defects <5 mm
- Incomplete - defects >1 cm or muscularis propria exposed
Preoperative Preparation
- Mechanical bowel preparation + oral antibiotics (reduces SSI compared with MBP alone)
- Stoma site marking if planned
- DVT prophylaxis and IV antibiotics on day of surgery
Surgical Procedures by Location
| Location | Operation | Notes |
|---|---|---|
| Upper rectum | Low Anterior Resection (LAR) | 5 cm distal margin preferred; tumor-specific mesorectal excision |
| Mid rectum | LAR with complete TME | Colorectal or coloanal anastomosis |
| Low rectum | LAR with coloanal anastomosis (CAA) | 1 cm distal margin acceptable if complete TME achieved |
| Very low / sphincter involvement | Abdominoperineal Resection (APR) | Permanent colostomy; when sphincter preservation impossible |
Sphincter Preservation
- Attempted whenever adequate distal margin is achievable with functional sphincter
- 1 cm distal margin acceptable for low tumors if complete TME is done
- Neoadjuvant therapy may downsize tumor to allow LAR instead of APR (though not strongly guideline-supported for T2 N0 disease)
Surgical Approach
- Open vs. laparoscopic vs. robotic - no definitive difference in oncologic outcomes
- Laparoscopic: less pain, lower ileus, shorter stay, less blood loss
- Robotic: lower conversion rate, better 3D visualization, instrument articulation; but longer operative times and higher cost
- Transanal TME (taTME): emerging technique for low rectal cancers, particularly in obese patients or narrow pelvis
Stage-Specific Management Summary
| Stage | T/N | Treatment |
|---|---|---|
| Stage I | T1-T2 N0 | Surgery alone (LAR or APR with TME) |
| Stage II | T3-T4 N0 | Neoadjuvant therapy + TME + consider adjuvant chemo |
| Stage III | Any T, N+ | Neoadjuvant therapy (LCRT or SCRT or TNT) + TME + adjuvant chemo |
| Stage IV | M1 | Individualized: if resectable, systemic chemo → resection of primary + metastases; if unresectable, systemic therapy ± palliative procedures |
Stage IV / Synchronous Metastatic Disease
Approximately 20% present with synchronous metastases. Liver is most common site (~50% of stage IV have liver-only disease).
Management principles:
- Assess resectability in multidisciplinary setting (including hepatic/thoracic surgeons)
- Resectable = margin-negative removal of all known tumor possible with adequate organ reserve
- No benefit from incomplete R1/R2 resection in asymptomatic patients - systemic chemotherapy preferred
- For resectable liver disease: 3-4 months systemic therapy first (assess biology, facilitate resectability), then surgical options:
- Combined (simultaneous primary + liver resection): healthy patients, upper rectal tumors, minor hepatic resections
- Rectum-first approach
- Liver-first approach: if large liver burden, threatened CRM, short-course RT before liver surgery
Surgical algorithms for resectable stage IV: Individualised based on rectal tumor location, liver burden complexity, symptoms, and patient fitness.
Watch-and-Wait (Nonoperative Management)
For patients with clinical complete response (cCR) after neoadjuvant chemoradiation (assessed by DRE + endoscopy + MRI):
- Surveillance protocol without surgery
- Local tumor regrowth may occur - requires TME surgery
- Particularly appealing for distal rectal cancer where APR with permanent stoma would otherwise be required
- Currently supported by retrospective data; considered experimental pending prospective trial maturation
- Evidence basis: International Watch & Wait Database (IWWD)
Immunotherapy (dMMR/MSI-H tumors)
- Checkpoint inhibitors are first-line for stage IV dMMR/MSI-H colorectal cancer
- dMMR is rare in rectal cancer (~3-7%; most dMMR tumors arise in right colon)
- Neoadjuvant PD-1 blockade in dMMR LARC: early data show 100% cCR rate (12-patient prospective study), avoiding CRT or surgery entirely
- Long-term durability data pending; likely to change paradigms for dMMR LARC
Adjuvant Therapy
- Adjuvant chemotherapy (typically FOLFOX or CAPOX) after surgery for Stage III and high-risk Stage II
- If TNT approach was used preoperatively, adjuvant chemotherapy schedule is incorporated into the TNT protocol itself
- Adjuvant radiation is rarely given if adequate neoadjuvant radiation was delivered
Surveillance After Curative Resection
- Colonoscopy 3-6 months post-resection (if not completed before surgery)
- CEA monitoring
- CT chest/abdomen/pelvis - at regular intervals per NCCN guidelines
- MRI pelvis for local recurrence assessment
Sources:
- Current Surgical Therapy 14e - "Management of Rectal Cancer" (Low & Mutch)
- Sabiston Textbook of Surgery - "Management of Rectal Cancer with Synchronous Metastases"
- Mulholland & Greenfield's Surgery 7e - Watch and Wait; Risk Stratification Algorithm
- 2024 ASCO Guideline on Locally Advanced Rectal Cancer: Scott AJ et al., J Clin Oncol Oct 2024 - PMID 39116386
This is a shared conversation. Sign in to Orris to start your own chat.