Malaria medicine
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Searching the Web
antimalarial drugs 2025 WHO guidelines treatment
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from Harrison's 22e, Goodman & Gilman, and Katzung's pharmacology. Here is a thorough overview of malaria medicines:
Antimalarial Drugs — A Comprehensive Overview
The Malarial Parasite Life Cycle & Drug Targets
No single antimalarial drug kills sporozoites (the infecting form injected by mosquitoes), so chemoprophylaxis only prevents symptomatic disease — it does not prevent infection. Because no drug hits all parasite stages simultaneously, combinations are often required for complete parasite elimination.
Drugs fall into three functional groups (Goodman & Gilman's):
- Blood-stage schizonticidals only — artemisinins, chloroquine, mefloquine, quinine/quinidine, pyrimethamine, sulfadoxine, tetracyclines. These treat/prevent symptomatic malaria but cannot clear liver hypnozoites.
- Liver + blood-stage actives — atovaquone + proguanil (Malarone). Because they kill primary liver stages of P. falciparum, post-exposure prophylaxis can stop sooner (only a few days after leaving the endemic area).
- Hypnozoite-active (radical cure) — primaquine and tafenoquine (8-aminoquinolines). These are the only agents that eradicate dormant liver stages (hypnozoites) of P. vivax and P. ovale responsible for relapses.
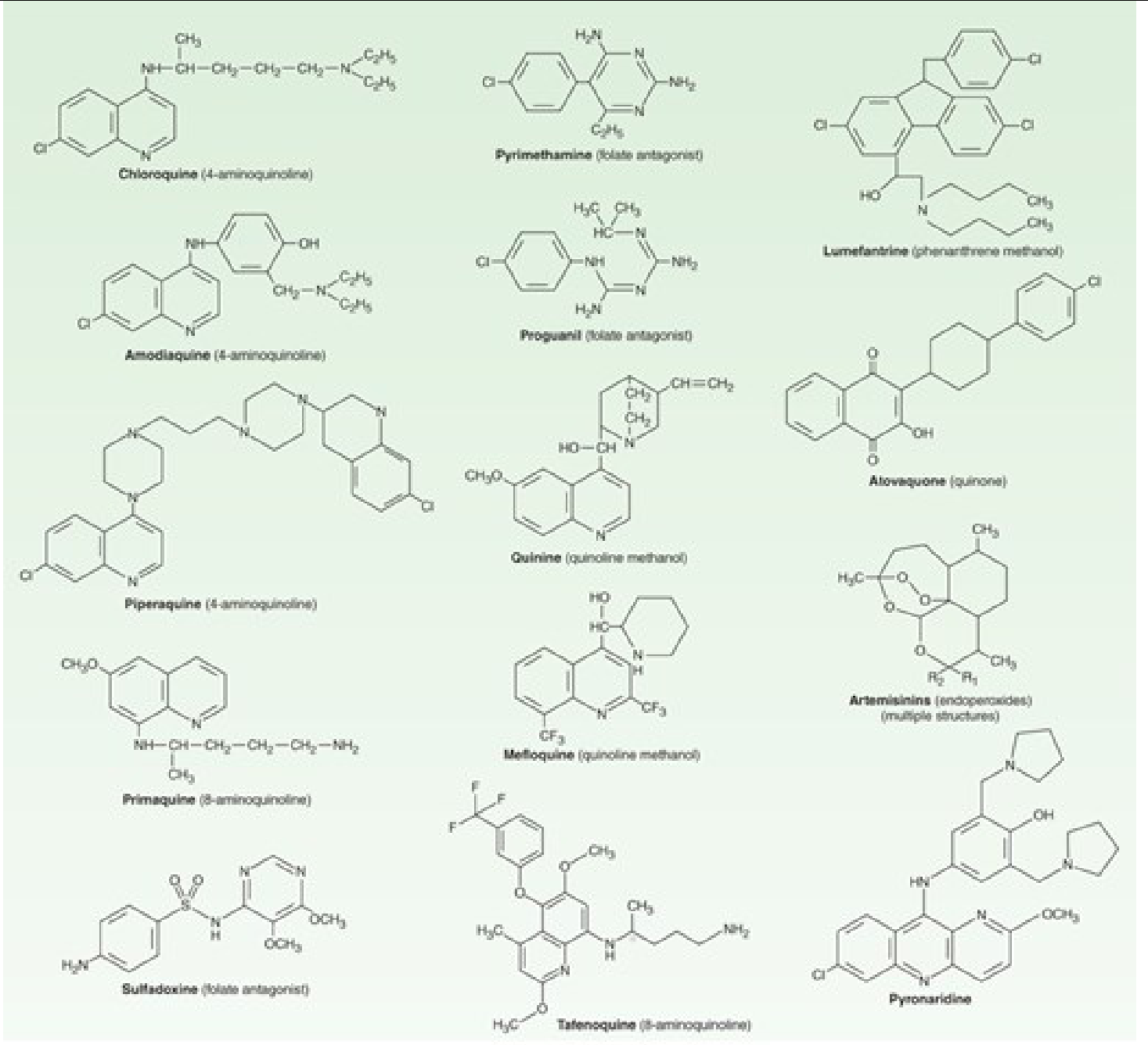
Drug Classification Table
(from Katzung's Basic & Clinical Pharmacology, 16th Ed.)
| Drug | Chemical Class | Primary Use |
|---|---|---|
| Chloroquine | 4-Aminoquinoline | Treatment & prophylaxis where parasites remain sensitive |
| Amodiaquine | 4-Aminoquinoline | Some chloroquine-resistant P. falciparum; fixed combo with artesunate |
| Piperaquine | Bisquinoline | P. falciparum in fixed combo with dihydroartemisinin (DHA-PPQ) |
| Quinine | Quinoline methanol | Oral/IV treatment of P. falciparum (severe disease; often + doxycycline) |
| Mefloquine | Quinoline methanol | Prophylaxis & treatment of P. falciparum |
| Primaquine | 8-Aminoquinoline | Radical cure of P. vivax/P. ovale; terminal prophylaxis |
| Tafenoquine | 8-Aminoquinoline | Radical cure of P. vivax; once-dose alternative to 14-day primaquine |
| Sulfadoxine-pyrimethamine (SP/Fansidar) | Folate antagonist combo | Some chloroquine-resistant P. falciparum; intermittent preventive therapy (IPT) in pregnancy |
| Atovaquone-proguanil (Malarone) | Quinone + folate antagonist | Treatment & prophylaxis of P. falciparum |
| Doxycycline | Tetracycline | Treatment (with quinine) of P. falciparum; prophylaxis |
| Lumefantrine | Amyl alcohol | Fixed combo with artemether (Coartem/AL) — most widely used ACT |
| Artemisinins (artesunate, artemether, dihydroartemisinin) | Sesquiterpene lactone endoperoxides | First-line treatment of P. falciparum; IV artesunate for severe disease |
| Pyronaridine | Mannich base acridine | Fixed combo with artesunate (Pyramax) |
Drug Mechanisms
Artemisinins
Free-radical generation after endoperoxide bond cleavage → damage to parasite proteins and membranes. Artemisinin and derivatives are the fastest-acting antimalarials, with a half-life of ~1 hour (artesunate). They are 10-fold more potent in vivo than other drugs and show no cross-resistance with older agents, making them the cornerstone of modern malaria therapy — Harrison's Principles of Internal Medicine 22e.
Chloroquine / Aminoquinolines
Accumulate in the parasite's digestive vacuole → inhibit heme polymerization → toxic free heme accumulates → parasite death. Resistance in P. falciparum is mediated by the Pfcrt transporter mutation, which pumps chloroquine out of the vacuole.
Artemisinins + Partner Drugs (ACTs)
Artemisinin rapidly reduces parasite biomass; the slower-eliminated partner drug (lumefantrine, piperaquine, amodiaquine, etc.) eliminates residual parasites and provides prolonged protection. This two-drug strategy also provides mutual protection against the emergence of resistance.
Atovaquone-Proguanil (Malarone)
Atovaquone blocks the mitochondrial electron transport chain (cytochrome bc1 complex); proguanil (activated to cycloguanil) inhibits dihydrofolate reductase (DHFR). The combination acts synergistically.
Primaquine / Tafenoquine
Mechanism not fully elucidated; likely involves oxidative stress in the parasite. Critical warning: Both cause dose-dependent hemolysis in patients with G6PD deficiency — G6PD testing is mandatory before use.
WHO-Recommended Treatment (Harrison's 22e, 2025)
Uncomplicated P. falciparum (and P. knowlesi)
Artemisinin-based combination therapy (ACT) is WHO first-line:
- Artemether-lumefantrine (AL / Coartem) — most widely used globally
- Artesunate-amodiaquine (ASAQ)
- Dihydroartemisinin-piperaquine (DHA-PPQ)
- Artesunate-mefloquine (ASMQ)
- Artesunate-pyronaridine (Pyramax)
Uncomplicated P. vivax, P. ovale, P. malariae
- Chloroquine remains effective in most areas
- Add primaquine (14 days) or tafenoquine (single dose) for radical cure of P. vivax/P. ovale to prevent relapses
Severe / Complicated Malaria
- IV artesunate is the treatment of choice worldwide (superior to IV quinine in trials)
- If artesunate unavailable: IV artemether preferred over quinine
- After 24 h of parenteral treatment and clinical improvement, switch to full-course oral ACT
Chemoprophylaxis
| Regimen | Coverage | Notes |
|---|---|---|
| Atovaquone-proguanil | All areas including chloroquine-resistant zones | Start 1–2 days before, stop 7 days after; short post-exposure window |
| Doxycycline | All areas including multidrug-resistant zones | Start 1–2 days before, stop 4 weeks after |
| Mefloquine | Chloroquine-resistant areas | Start 2–3 weeks before, stop 4 weeks after; neuropsychiatric side effects |
| Chloroquine | Only in chloroquine-sensitive areas (now very limited) | Start 1–2 weeks before, stop 4 weeks after |
| Primaquine | All species including hypnozoites | Requires G6PD testing |
Non-drug measures (insecticide-treated bed nets, repellents, protective clothing) are essential alongside any drug prophylaxis — no chemoprophylactic regimen is fully protective.
Resistance: A Growing Crisis
Harrison's 22e highlights a critical emerging problem:
- Artemisinin resistance in P. falciparum (driven by Pfkelch13 mutations) emerged in Southeast Asia (Greater Mekong Subregion) in the late 2000s and has now spread to East Africa.
- This is accompanied by resistance to partner drugs (piperaquine, mefloquine) in some areas.
- Proposed solution: Triple ACTs combining two slowly eliminated partner drugs for mutual protection.
- Falsified/substandard antimalarials on shelves in Asia and Africa are also a significant cause of treatment failures.
Key Drug Toxicities at a Glance
| Drug | Major Adverse Effects |
|---|---|
| Chloroquine | Retinopathy (long-term), QTc prolongation, pruritus (in Africans) |
| Quinine/Quinidine | Cinchonism (tinnitus, headache), hypoglycemia, QTc prolongation |
| Mefloquine | Neuropsychiatric effects (nightmares, psychosis), QTc prolongation |
| Primaquine/Tafenoquine | Hemolytic anemia in G6PD deficiency |
| Atovaquone-proguanil | GI disturbance; teratogenic potential of proguanil — avoid in first trimester |
| Artemisinins | Generally well tolerated; rare neurotoxicity at very high doses |
| Doxycycline | Photosensitivity, GI upset, esophagitis; contraindicated in pregnancy/children <8 yr |
Special Populations
- Pregnancy: Falciparum malaria is especially dangerous (hypoglycemia, pulmonary edema, fetal loss). ACTs are the recommended treatment; SP is used for intermittent preventive therapy in pregnancy (IPTp). Primaquine/tafenoquine are contraindicated in pregnancy.
- Children: Most malaria deaths (~600,000/yr) occur in African children. ACTs are first-line; IV artesunate for severe disease; dosing is weight-based.
- G6PD-deficient patients: Must avoid primaquine and tafenoquine without careful testing and risk assessment.
Sources: Harrison's Principles of Internal Medicine 22e (2025) | Goodman & Gilman's Pharmacological Basis of Therapeutics | Katzung's Basic & Clinical Pharmacology, 16th Ed. | WHO Guidelines for Malaria, August 2025
This is a shared conversation. Sign in to Orris to start your own chat.