glomerular filtration barrier and its clinical aspect with UTI
Reading File
Finding Sources
Finding Sources
Searching PubMed
"glomerular filtration barrier" AND proteinuria
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full answer.
Glomerular Filtration Barrier - Structure, Function, and Clinical Aspects with UTI
1. Overview of the Glomerular Filtration Barrier (GFB)
The glomerular filtration barrier (GFB) is a highly specialized, trilaminar structure that separates the capillary lumen from Bowman's space. It determines what enters the urinary filtrate - allowing water and small solutes through freely while excluding plasma proteins and blood cells. The GFB consists of four functional elements:
- Glycocalyx overlying the endothelial cells
- Fenestrated endothelium
- Glomerular basement membrane (GBM)
- Podocyte epithelial layer with slit diaphragms
(Medical Physiology - Boron & Boulpaep; Costanzo Physiology 7th Ed.)
2. Layers in Detail
Layer 1 - Fenestrated Endothelium
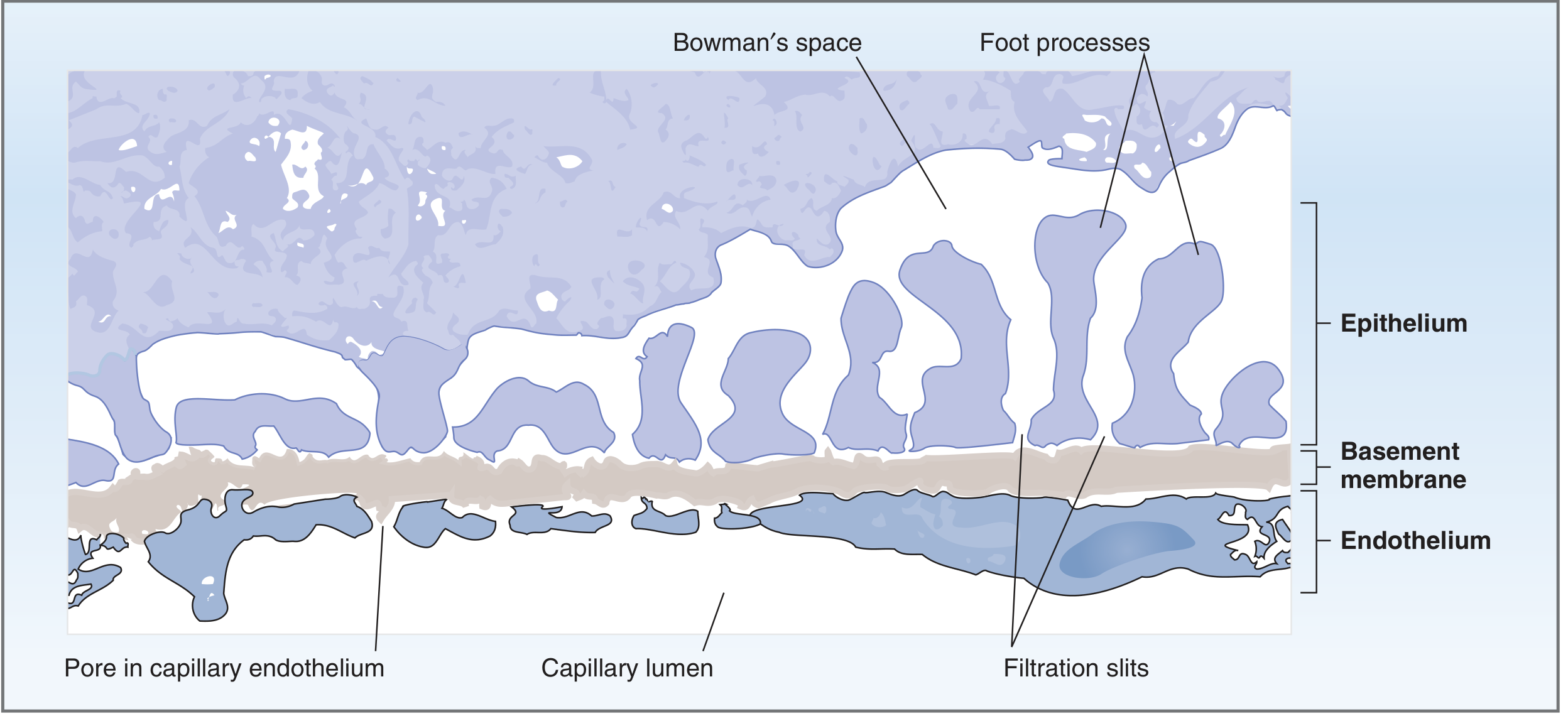
- Endothelial cells have fenestrations (pores) 70-100 nm in diameter
- These pores freely pass fluid, dissolved solutes, and plasma proteins
- They are not large enough to permit blood cells to cross
- The surface is coated by an endothelial glycocalyx (negatively charged), which acts as the first electrostatic barrier against anionic proteins like albumin
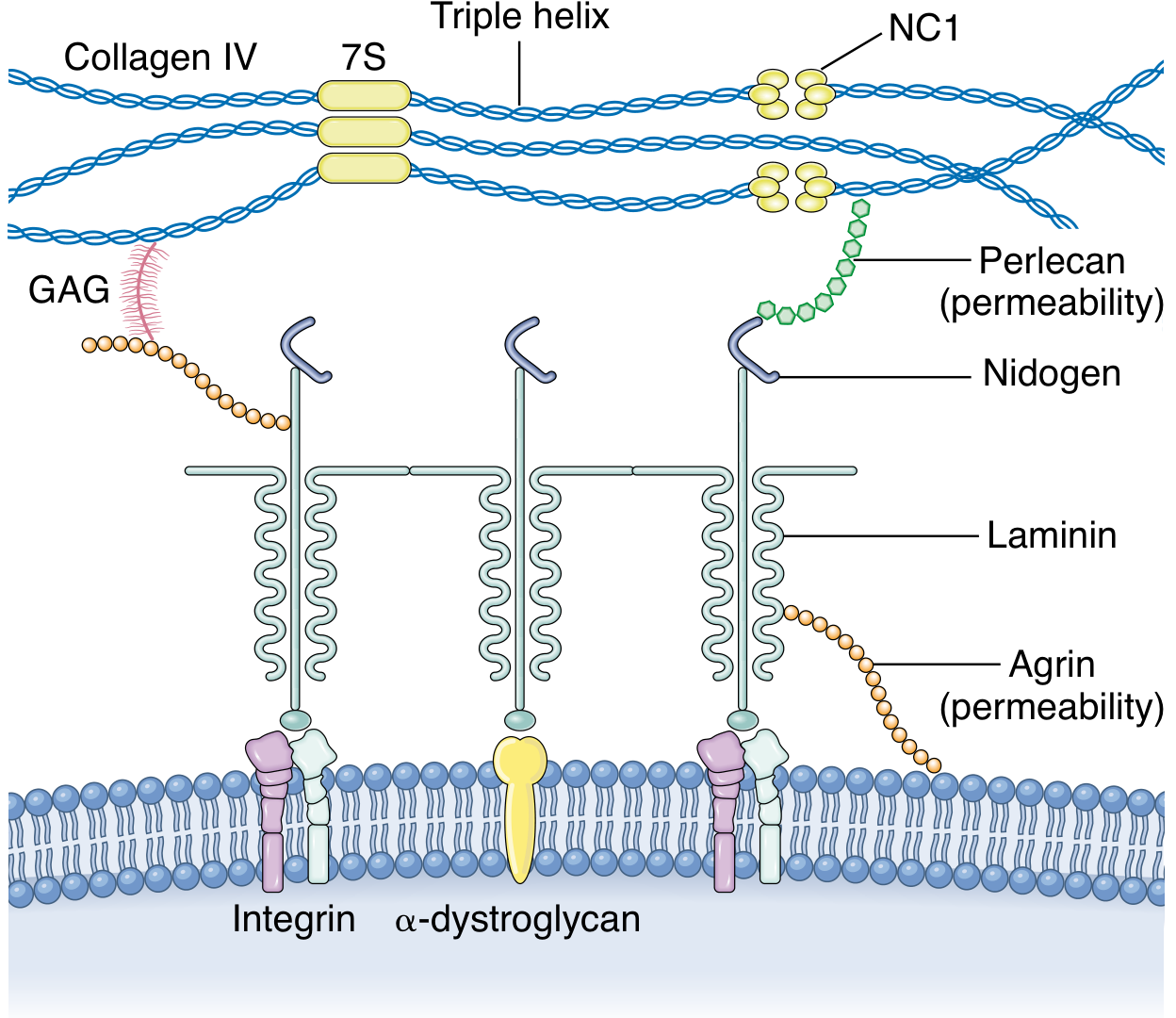
Layer 2 - Glomerular Basement Membrane (GBM)
The GBM has three sublayers (Costanzo Physiology):
- Lamina rara interna - fused to the endothelium
- Lamina densa - central dense layer (primary structural barrier)
- Lamina rara externa - fused to the podocyte layer
Key molecular components (Brenner & Rector's The Kidney):
- Type IV collagen (α3α4α5 chains in the mature GBM) - provides structural scaffold
- Laminin 521 - synthesized jointly by podocytes and endothelial cells
- Agrin and perlecan - heparan sulfate proteoglycans (HSPGs) providing anionic charge barrier
- Nidogen - links collagen IV to laminin networks
The multilayered GBM is considered the most significant barrier to plasma protein filtration.
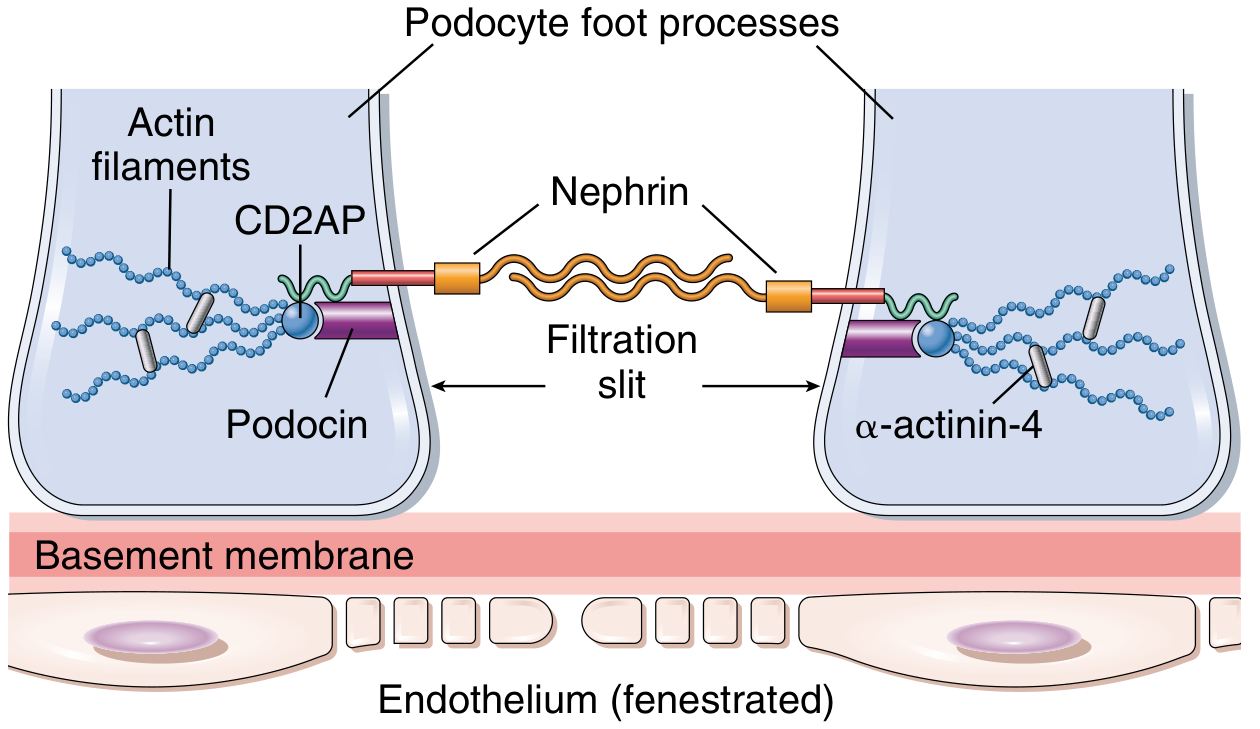
Layer 3 - Podocytes and Filtration Slit Diaphragm
Podocytes are highly differentiated mesenchymal cells that:
- Extend major processes from the cell body
- Major processes give rise to secondary foot processes that interdigitate in a "zipper-like" pattern
- Between adjacent foot processes are filtration slits (25-60 nm) bridged by the slit diaphragm
Slit diaphragm molecular architecture (Brenner & Rector):
- Nephrin (NPHS1) - transmembrane immunoglobulin superfamily protein; forms the core structural scaffold of the slit with neph1; nephrin molecules are positioned on the apical side
- Podocin (NPHS2) - anchors nephrin to the plasma membrane; creates a signaling hub in lipid-rich membrane compartments; linked to TRPC6 channel
- CD2AP (CD2-associated protein) - links nephrin/podocin complex to the actin cytoskeleton
- α-actinin-4 - connects foot process actin filaments
- ZO-1, occludin - tight junction proteins associated with the slit diaphragm
- FAT1, P-cadherin - adherens junction proteins
- Podocalyxin - sialomucin on the apical surface; its highly negative charge keeps adjacent foot processes separated, maintaining the filtration barrier open
3. Filtration Selectivity - Size and Charge Barriers
Two mechanisms restrict what crosses the GFB (Costanzo Physiology 7th Ed.):
Size Selectivity
| Component | Pore/Slit Size | Function |
|---|---|---|
| Endothelial fenestrae | 70-100 nm | Bars blood cells |
| GBM (lamina densa) | ~8 nm effective radius | Bars large proteins |
| Filtration slits | 25-60 nm | Additional barrier |
Charge Selectivity
- Fixed negative charges (from HSPGs agrin/perlecan, podocalyxin, endothelial glycocalyx) line all three layers
- These repel negatively charged macromolecules like albumin (which has net negative charge at physiologic pH)
- They attract positively charged solutes
- Small ions (Na⁺, K⁺, Cl⁻, HCO₃⁻) are freely filtered regardless of charge
- Classic experiment (Costanzo): Dextrans of the same molecular radius but different charges - cationic dextran filtered most, anionic dextran filtered least, neutral in between
4. Clinical Aspects - When the Filtration Barrier Fails
A. Nephrotic Syndrome - Loss of Charge/Structural Barrier
| Disease | Mechanism of GFB Disruption | Key Feature |
|---|---|---|
| Minimal Change Disease (MCD) | Loss of anionic charges (HSP loss), podocyte foot process effacement via CD80, c-mip, and angiopoietin-like 4 activation | Nephrotic range proteinuria; foot processes effaced on EM |
| Focal Segmental Glomerulosclerosis (FSGS) | Mutations in NPHS1 (nephrin), NPHS2 (podocin), ACTN4 (α-actinin-4), TRPC6 | Segmental scarring, massive proteinuria |
| Membranous Nephropathy | Anti-PLA2R antibodies attacking podocyte antigens; immune complex deposition in subepithelial space | "Spike and dome" on EM; complement activation |
| Diabetic Nephropathy | GBM thickening (increased synthesis), loss of HSPGs, mesangial expansion | Microalbuminuria → proteinuria |
| Alport Syndrome | Mutations in COL4A3/A4/A5 (type IV collagen α-chains) → "basket-weave" GBM appearance | Hematuria, sensorineural deafness, renal failure |
(Comprehensive Clinical Nephrology 7th Ed.; Robbins Pathologic Basis of Disease; Brenner & Rector)
B. Nephritic Syndrome - Breach of Barrier by Inflammation
- Post-infectious GN (e.g., post-streptococcal): immune complex deposition activates complement and neutrophil infiltration
- IgA Nephropathy: galactose-deficient IgA1 forms mesangial deposits; characterized by synpharyngitic hematuria
- Crescent GN (RPGN): rupture of GBM; fibrin and plasma proteins leak into urinary space → crescent formation
5. UTI - Clinical Aspects and Renal Connection
Definitions (Comprehensive Clinical Nephrology 7th Ed.)
- Asymptomatic bacteriuria (ASB): >10⁵ organisms/mL without symptoms
- Cystitis: lower tract infection (frequency, dysuria, strangury); as few as 10² organisms/mL with pyuria and symptoms
- Acute pyelonephritis: >10⁵ organisms/mL + parenchymal infiltration + upper tract symptoms (fever, loin pain); may progress to systemic sepsis
Common Organisms
- E. coli (>70% of UTIs) - virulence factors include type 1 fimbriae (P-pili) for uroepithelial adhesion
- Klebsiella spp.
- Proteus spp. (especially in diabetics or urinary obstruction)
- Enterococci
- Staphylococcus saprophyticus
- Pseudomonas (especially in catheterized/immunocompromised patients)
Pathogenesis of Ascending Infection
The most common route is ascending from the urethra:
- Perineal colonization (mostly E. coli)
- Ascent through urethra to bladder (cystitis)
- Ascent through ureters to renal pelvis and parenchyma (pyelonephritis)
- Bacterial fimbriae (pili) attach to urothelial receptors, facilitating ascent
UTI and Renal Damage - The GFB Connection
Pyelonephritis affects the glomerular filtration barrier indirectly through:
- Direct parenchymal bacterial infiltration causing inflammation that can extend to glomeruli
- Reflux nephropathy (VUR + recurrent UTI) leading to renal scarring, interstitial fibrosis, and reduced GFR
- Obstructive uropathy + UTI leading to hydronephrosis and permanent nephron loss
- Sepsis from pyelonephritis causing hemodynamic compromise → acute kidney injury (reduced GFR via decreased Kf and reduced glomerular capillary pressure)
UTI in Special Clinical Populations Affecting the Filtration Barrier
Renal Transplant Patients (Brenner & Rector, Pediatric Transplant Section):
- UTI risk is increased post-transplant; ureteral stents and immunosuppression are risk factors
- Allograft pyelonephritis may cause graft dysfunction (reduced GFR) during acute episodes
- TMP-SMX prophylaxis reduces UTI incidence; VUR should be addressed to prevent recurrent UTI
Pregnancy (Comprehensive Clinical Nephrology 7th Ed.; Rosen's Emergency Medicine):
- Progesterone-induced smooth muscle relaxation → ureteral dilation + stasis → increased risk of ascending UTI
- ASB affects 2-9% of pregnant women; 30% of untreated ASB progresses to pyelonephritis
- Pyelonephritis in pregnancy: sepsis, permanent renal injury, premature labor
- US Preventive Services Task Force: screen with urine culture at 12-16 weeks gestation (Grade A)
- Treatment of ASB reduces pyelonephritis incidence by >80%
Management of UTI (Rosen's Emergency Medicine)
| Condition | Treatment |
|---|---|
| ASB/Cystitis (pregnant) | Cephalexin 500 mg BID × 3-7 days, OR nitrofurantoin 100 mg BID × 3-7 days, OR amoxicillin 500 mg TID × 7 days (avoid nitrofurantoin near term) |
| Pyelonephritis (outpatient) | Oral fluoroquinolone × 7 days (if not pregnant); guided by local susceptibilities |
| Pyelonephritis (pregnant/inpatient) | IV ceftriaxone 1 g daily; adjust per culture; IV hydration + obstetric consultation |
| Recurrent UTI | Identify and treat anatomical abnormalities (VUR, obstruction); low-dose antibiotic prophylaxis |
6. Summary: GFB-UTI Clinical Integration
| GFB Impairment Mechanism | Resulting Condition | Clinical Link to UTI |
|---|---|---|
| Charge loss (HSP depletion) | Proteinuria (MCD-like) | Infections can trigger MCD relapse via TLR ligands (LPS from gram-negative bacteria, poly-IC from viruses) |
| GBM inflammation/breach | Post-infectious GN | Group A Streptococcal infections - both pharyngeal and skin infections; urinary infections less commonly implicated |
| Reflux nephropathy from recurrent UTI | Renal scarring → reduced GFR | Progressive loss of filtration surface area |
| Septic AKI from pyelonephritis | Reduced GFR (intrinsic + pre-renal) | Hemodynamic compromise + direct tubular toxicity |
| Allograft pyelonephritis | Acute graft dysfunction | Transient GFR reduction; long-term graft function may be preserved |
Sources:
- Costanzo Physiology 7th Ed., Chapter 6 - Renal Physiology
- Brenner & Rector's The Kidney 2-Volume Set - Chapters on Podocyte Development and Structure
- Comprehensive Clinical Nephrology 7th Ed. - UTI in Pregnancy, Loss of Anionic Charges in GFB
- Robbins, Cotran & Kumar Pathologic Basis of Disease - Glomerular Filtration Barrier and Injury Patterns
- Rosen's Emergency Medicine - UTI Management in Pregnancy
- Medical Physiology (Boron & Boulpaep) - Filterability of Solutes
Recent evidence note: A 2025 systematic review (PMID: 41368354) confirms that genetic and environmental factors altering filtration slit proteins (nephrin, podocin) play a significant role in proteinuric kidney diseases - consistent with the above textbook content.
This is a shared conversation. Sign in to Orris to start your own chat.