Bronchial asthma. Describe drug mechanism of ac-action of any one drug. Enumerate group of drug with one example and MOA. Classify drugs to adverse effect of any one of them.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed to give a thorough, well-structured answer. Here is the complete response:
Bronchial Asthma - Drug Pharmacology
Classification of Drugs Used in Bronchial Asthma
Drugs are broadly classified into Bronchodilators (Relievers) and Anti-inflammatory Agents (Controllers).
Group 1: β2-Adrenoceptor Agonists (Sympathomimetics)
| Subclass | Example |
|---|---|
| Short-Acting (SABA) | Salbutamol (Albuterol) |
| Long-Acting (LABA) | Salmeterol, Formoterol |
Group 2: Methylxanthines
Example: Theophylline, Aminophylline
Group 3: Anticholinergics (Muscarinic Antagonists)
| Subclass | Example |
|---|---|
| Short-Acting (SAMA) | Ipratropium bromide |
| Long-Acting (LAMA) | Tiotropium |
Group 4: Inhaled Corticosteroids (ICS)
Examples: Beclomethasone, Budesonide, Fluticasone
Group 5: Leukotriene Modifiers
Examples: Montelukast (receptor antagonist), Zileuton (synthesis inhibitor)
Group 6: Mast Cell Stabilizers
Example: Sodium cromoglycate, Nedocromil
Group 7: Biologicals / Monoclonal Antibodies
Examples: Omalizumab (anti-IgE), Mepolizumab (anti-IL-5)
Drug Mechanism of Action (Detailed) - Salbutamol (β2-Agonist)
Salbutamol is a selective β2-adrenoceptor agonist and the prototype short-acting bronchodilator.
Step-by-step mechanism:
- Salbutamol binds to β2-adrenoceptors on airway smooth muscle cells (these receptors are abundant in bronchial smooth muscle).
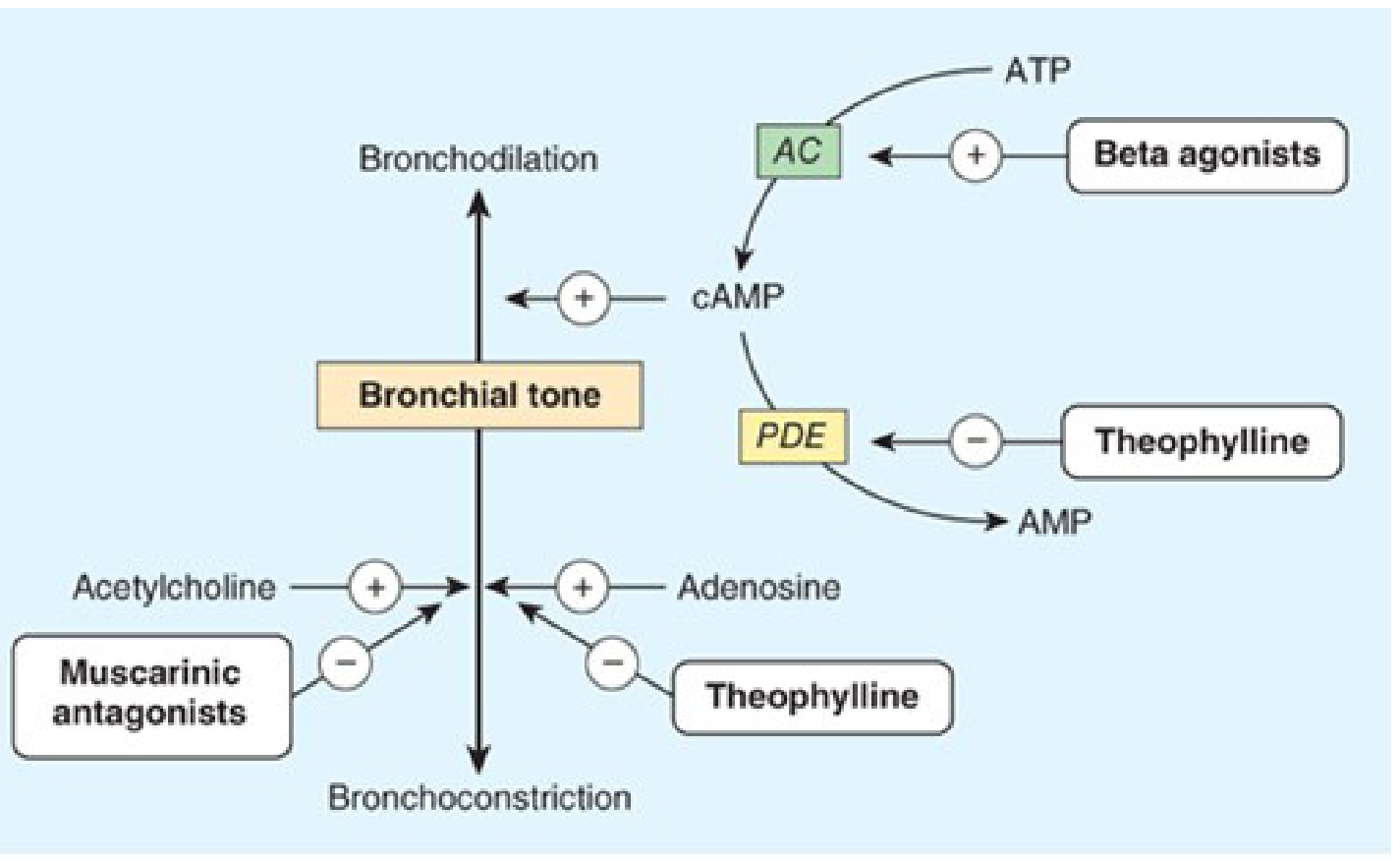
- The receptor is coupled to Gs protein, which activates adenylyl cyclase (AC).
- Adenylyl cyclase converts ATP → cyclic AMP (cAMP).
- Elevated intracellular cAMP activates protein kinase A (PKA).
- PKA phosphorylates myosin light chain kinase (MLCK), inactivating it, preventing actin-myosin cross-bridge formation.
- PKA also opens large-conductance Ca²⁺-activated K⁺ channels, causing membrane hyperpolarization and reducing intracellular Ca²⁺.
- Net result: bronchial smooth muscle relaxation → bronchodilation.
Additional effects:
- Inhibits mediator release from mast cells
- Inhibits microvascular leakage
- Stimulates mucociliary clearance
MOA of One Drug from Each Group (Enumerated)
| Group | Example Drug | Mechanism of Action |
|---|---|---|
| β2-Agonist | Salbutamol | Binds β2-receptor → activates adenylyl cyclase → ↑cAMP → PKA activation → smooth muscle relaxation (bronchodilation) |
| Methylxanthines | Theophylline | Inhibits phosphodiesterase (PDE) → prevents cAMP breakdown → ↑cAMP → bronchodilation; also antagonizes adenosine receptors on bronchial smooth muscle |
| Anticholinergics | Ipratropium | Competitively blocks muscarinic (M3) receptors on bronchial smooth muscle → prevents acetylcholine-mediated bronchoconstriction |
| Corticosteroids (ICS) | Budesonide | Binds intracellular glucocorticoid receptors → translocates to nucleus → inhibits transcription of pro-inflammatory cytokines (IL-4, IL-5, TNF-α) → reduces airway inflammation, eosinophil/mast cell infiltration, and bronchial hyperreactivity |
| Leukotriene antagonist | Montelukast | Competitively antagonizes CysLT1 receptors → blocks action of leukotrienes (LTC4, LTD4, LTE4) → reduces bronchoconstriction, mucus secretion, and airway edema |
| Mast cell stabilizer | Sodium cromoglycate | Blocks Ca²⁺ channels on mast cells → prevents mast cell degranulation → inhibits release of histamine, leukotrienes, and other mediators |
| Anti-IgE | Omalizumab | Monoclonal antibody that binds free IgE → prevents IgE binding to FcεRI receptors on mast cells and basophils → reduces allergen-triggered degranulation |
Adverse Effects - Theophylline (Classified)
Theophylline has a narrow therapeutic index (therapeutic range: 10-20 mcg/mL); toxicity is common.
Dose-related / Concentration-dependent ADRs
Mild (serum level > 20 mcg/mL):
- Nausea, vomiting, anorexia
- Headache
- Restlessness, insomnia
Moderate (serum level > 25 mcg/mL):
- Tachycardia, palpitations
- Tremors
- Diarrhea
Severe (serum level > 35 mcg/mL):
- Cardiac arrhythmias (ventricular tachycardia, atrial fibrillation)
- Seizures (life-threatening, may be refractory to diazepam)
- Hypotension
System-based Classification of Theophylline ADRs
| System | Adverse Effect |
|---|---|
| GI | Nausea, vomiting, gastric irritation, peptic ulceration |
| CNS | Headache, insomnia, restlessness, tremors, seizures |
| CVS | Tachycardia, arrhythmias, hypotension |
| Metabolic | Hypokalemia, hyperglycemia |
| Renal | Diuresis (due to adenosine antagonism) |
Note: Theophylline toxicity is worsened by drugs that inhibit CYP1A2 (e.g., ciprofloxacin, erythromycin, cimetidine) - these raise serum theophylline levels. Smoking induces CYP1A2 and lowers levels.
Sources: Katzung's Basic and Clinical Pharmacology, 16th Edition (Ch. 20); Lippincott Illustrated Reviews: Pharmacology, 8th Edition (Ch. on Respiratory Pharmacology).
This is a shared conversation. Sign in to Orris to start your own chat.