Explain In Detail About our Intestine Both Small and Large Intestine
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive, authoritative content from multiple textbooks. Let me compile the complete, detailed answer.
The Intestine: Small and Large - A Complete Guide
Sources: Gray's Anatomy for Students, Medical Physiology (Boron & Boulpaep), Costanzo Physiology 7e, Junqueira's Basic Histology 17e, Histology: A Text and Atlas, Sleisenger & Fordtran's GI and Liver Disease
Overview
The intestine occupies most of the abdominal cavity and is divided into two structurally and functionally distinct parts. The small intestine (~6 m long) is the primary site for digestion and nutrient absorption, while the large intestine (~1.5-2.4 m long) absorbs water and electrolytes and converts the remaining material into feces. Together, they process every meal you eat from start to finish.
PART I: THE SMALL INTESTINE
1. Anatomy and Divisions
The small intestine runs from the pylorus of the stomach to the ileocecal valve, where it meets the large intestine. It has three distinct segments:
| Segment | Length | Key Features |
|---|---|---|
| Duodenum | ~25 cm (C-shaped) | First and shortest; receives bile and pancreatic secretions; mostly retroperitoneal |
| Jejunum | ~2.5 m | Thicker wall, more prominent folds; most nutrient absorption occurs here |
| Ileum | ~3.5 m | Thinner wall; contains Peyer's patches (lymphoid tissue); absorbs vitamin B12 and bile salts |
The jejunum and ileum are suspended from the posterior abdominal wall by the mesentery, allowing mobility inside the abdominal cavity.
2. Wall Layers (from inside out)
The wall of the small intestine - like the rest of the GI tract - is built in four concentric layers:
-
Mucosa - the innermost layer, consisting of:
- Epithelium (simple columnar, with villi and crypts)
- Lamina propria (loose connective tissue with immune cells, blood vessels, lymphatics/lacteals)
- Muscularis mucosae (thin smooth muscle layer)
-
Submucosa - dense irregular connective tissue containing blood vessels, lymphatics, and the Meissner (submucosal) nerve plexus. In the duodenum, this layer also contains Brunner's glands, which secrete alkaline mucus to neutralize acidic chyme from the stomach.
-
Muscularis externa - two smooth muscle layers:
- Inner circular layer
- Outer longitudinal layer
- Between them lies the Auerbach (myenteric) plexus, which controls peristalsis
-
Serosa (peritoneum) - the outermost layer
3. Surface Area Amplification - The Key to Absorption
The small intestine has a total absorptive surface area of approximately 200 m² - roughly the size of a doubles tennis court. This is achieved through three levels of folding:
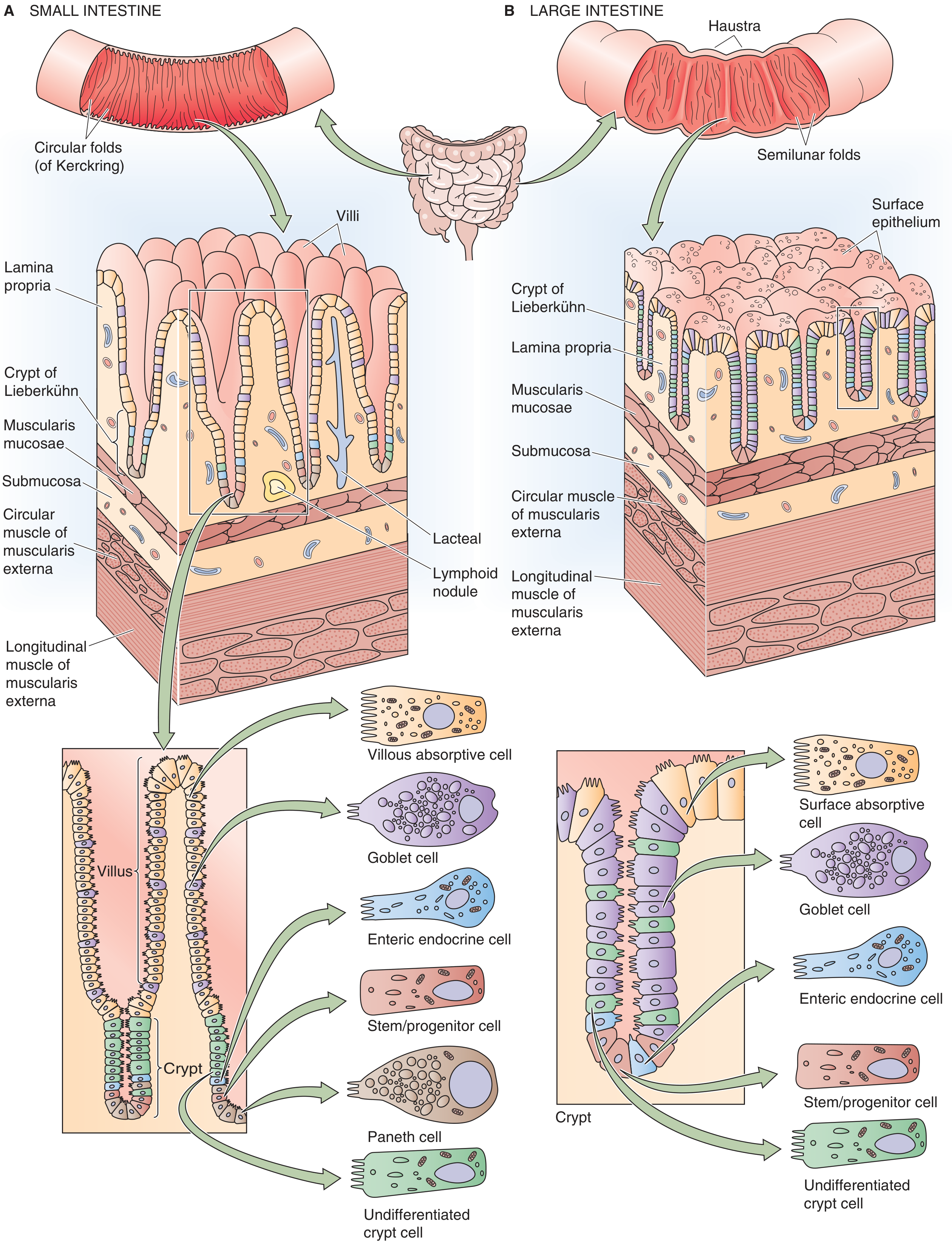
Fig: Small intestine (left) vs Large intestine (right) - showing villi, crypts of Lieberkühn, and cell types. Source: Medical Physiology
Level 1 - Folds of Kerckring (plicae circulares): Permanent macroscopic circular folds of the mucosa and submucosa. They are most prominent in the jejunum and force chyme to spiral through, slowing transit and maximizing contact. They amplify surface area 3-fold.
Level 2 - Villi: Finger-like or leaf-like projections (0.5-1.5 mm tall) of the mucosa that project into the intestinal lumen. The villi are tallest in the duodenum and shortest in the terminal ileum. Each villus contains a lacteal (lymphatic capillary for fat absorption) and a network of blood capillaries. Villi increase surface area a further 10-fold.
Level 3 - Microvilli (brush border): Tiny projections on the apical surface of each enterocyte (absorptive cell). Under light microscopy they create a "brush border" appearance. The microvilli amplify surface area by a further 20-fold.
In total, these three levels multiply surface area by 600-fold compared to a smooth hollow cylinder of the same dimensions. - Costanzo Physiology 7e
Between the villi are tube-like pits called crypts of Lieberkühn (intestinal glands), where new epithelial cells are produced. Intestinal epithelial cells turn over every 3-6 days - one of the fastest renewal rates in the body, which is why chemotherapy and radiation cause intestinal damage so readily.
4. Cell Types in the Small Intestine
| Cell Type | Location | Function |
|---|---|---|
| Enterocytes (absorptive cells) | Villi surface | Nutrient absorption via brush border enzymes and transporters |
| Goblet cells | Villi and crypts | Secrete mucus for lubrication and protection |
| Paneth cells | Base of crypts (ileum) | Secrete antimicrobial peptides (defensins, lysozyme); maintain crypt microenvironment |
| Enteroendocrine cells | Scattered throughout | Secrete hormones (CCK, secretin, GIP, GLP-1, etc.) |
| Stem/progenitor cells | Middle third of crypts | Generate all epithelial cell types |
| M cells | Over Peyer's patches | Sample luminal antigens for immune surveillance |
5. Digestion and Absorption
Carbohydrates
Only monosaccharides can be absorbed. Starch is broken down by:
- Salivary amylase (minor role, inactivated by stomach acid)
- Pancreatic amylase → yields maltose, maltotriose, and α-limit dextrins
- Brush border enzymes (maltase, sucrase, lactase, α-dextrinase) → final breakdown to glucose, galactose, fructose
Glucose and galactose are absorbed via SGLT-1 (sodium-glucose co-transporter, active transport). Fructose enters via GLUT-5 (facilitated diffusion). All three exit the enterocyte via GLUT-2 into the bloodstream. - Costanzo Physiology 7e
Lactase deficiency causes lactose intolerance - undigested lactose reaches the colon where bacteria ferment it, producing gas and osmotic diarrhea.
Proteins
Proteins are digested by:
- Gastric pepsin (initiates)
- Pancreatic proteases (trypsin, chymotrypsin, elastase, carboxypeptidase) → di- and tripeptides + amino acids
- Brush border peptidases → final amino acids
Absorption occurs via specific amino acid transporters; di- and tripeptides enter via PepT-1 and are hydrolyzed inside the enterocyte.
Lipids
Lipid digestion requires a special approach because fats are hydrophobic:
- Emulsification by bile salts in the small intestine - creates small droplets with large surface area
- Pancreatic lipase (with colipase) hydrolyzes triglycerides → monoglycerides + fatty acids
- Products are packaged into micelles (cylindrical discs ~50 Å diameter, with bile salt exterior)
- Micelles diffuse to the brush border; lipids are released and enter enterocytes by passive diffusion
- Inside the enterocyte, fatty acids are re-esterified into triglycerides in the smooth ER, packaged with cholesterol and apoproteins into chylomicrons in the Golgi
- Chylomicrons are secreted by exocytosis into the lacteals (lymphatics), bypassing the portal circulation - Costanzo Physiology 7e
Water and Electrolytes
The small intestine absorbs approximately 6-7 L of fluid per day (from dietary intake plus secretions). Sodium absorption drives water absorption osmotically. The colon absorbs most of the remaining ~1.5 L.
Vitamins and Minerals
- Fat-soluble vitamins (A, D, E, K): absorbed with lipids in micelles
- Vitamin B12: binds intrinsic factor (from stomach parietal cells); absorbed specifically in the terminal ileum via receptor-mediated endocytosis
- Iron: absorbed in the duodenum as Fe²⁺ via DMT-1 transporter
- Calcium: absorbed in the duodenum, regulated by vitamin D (calcitriol)
- Bile salts: reabsorbed in the terminal ileum and recycled back to the liver via the enterohepatic circulation
6. Motility of the Small Intestine
- Segmentation contractions: Rhythmic local contractions that mix chyme with digestive juices without net forward movement. This is the primary motility pattern after a meal.
- Peristalsis: Wave-like contractions that propel chyme distally toward the colon. Controlled by the enteric nervous system (Auerbach plexus).
- Migrating motor complex (MMC): Occurs during fasting; sweeps debris, bacteria, and undigested matter into the colon every ~90 minutes. Disruption of the MMC leads to small intestinal bacterial overgrowth (SIBO).
- Transit time through the small intestine is approximately 2-6 hours.
PART II: THE LARGE INTESTINE
1. Anatomy and Divisions
The large intestine extends from the ileocecal valve to the anus, spanning approximately 1.5 m in adults and averaging 6-7 cm in diameter (wider than the small intestine, despite its name referring to length in the small intestine's case).
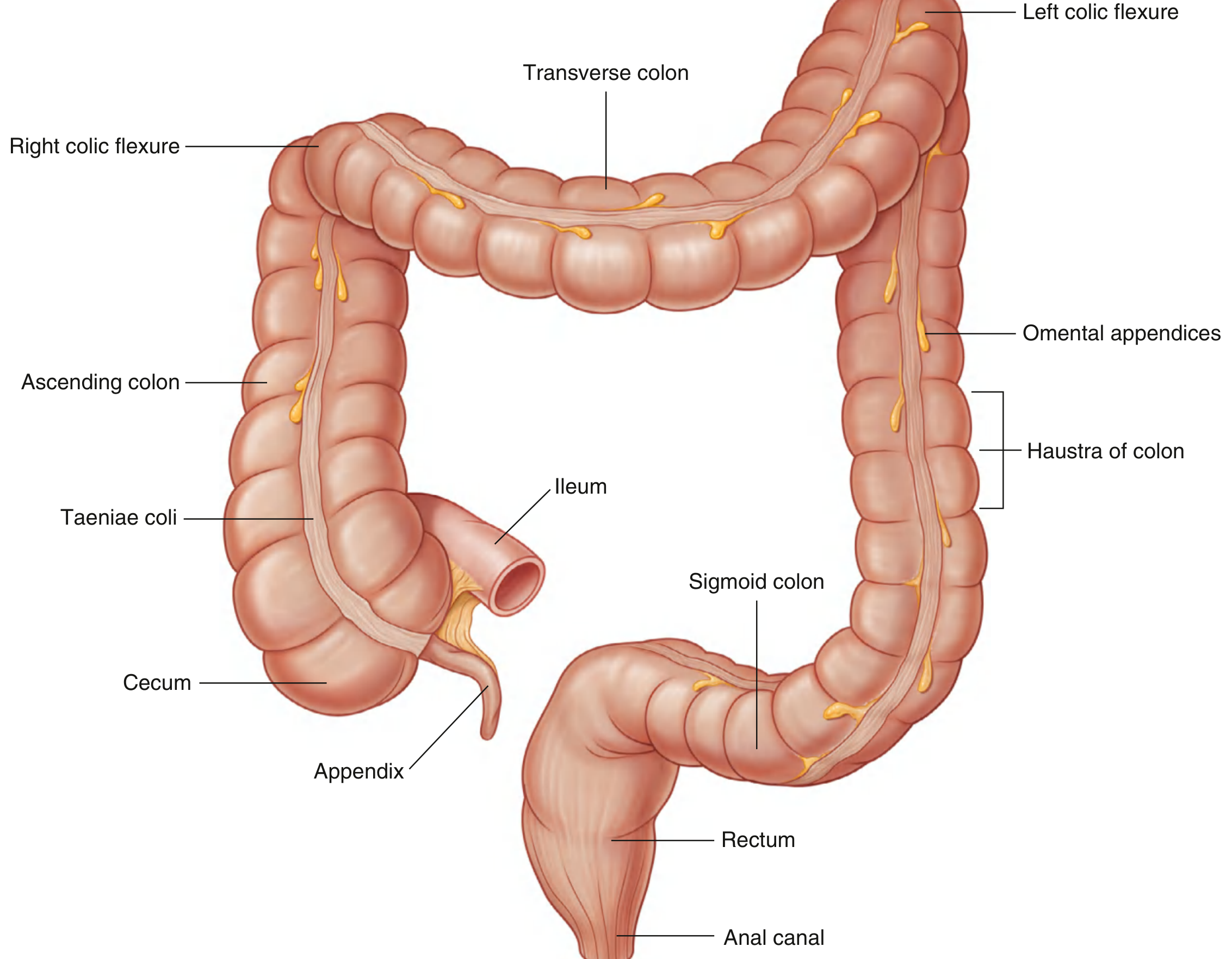
Fig: The large intestine with all major anatomical landmarks. Source: Gray's Anatomy for Students
Segments of the large intestine:
-
Cecum - A blind-ending pouch in the right iliac fossa below the ileocecal valve. It is intraperitoneal and has some mobility. The vermiform appendix arises from its posteromedial surface and contains dense lymphoid tissue (immune function).
-
Ascending colon - Travels superiorly through the right flank to the right hypochondrium. It is secondarily retroperitoneal (fixed to the posterior abdominal wall).
-
Right colic (hepatic) flexure - Where the ascending colon turns left, just inferior to the right lobe of the liver.
-
Transverse colon - The longest and most mobile segment, suspended by the transverse mesocolon. It crosses the abdomen from right to left.
-
Left colic (splenic) flexure - A sharper bend than the hepatic flexure, located just inferior to the spleen. It is attached to the diaphragm by the phrenico-colic ligament and is higher and more posterior than the right flexure.
-
Descending colon - Travels inferiorly through the left flank; retroperitoneal.
-
Sigmoid colon - An S-shaped, highly mobile, intraperitoneal segment suspended by the sigmoid mesocolon. It enters the pelvic cavity and transitions to the rectum.
-
Rectum - ~12-15 cm long; located on the posterior wall of the pelvic cavity. It stores feces before defecation. The mucosa forms three horizontal folds called valves of Houston (transverse rectal folds).
-
Anal canal - The terminal 3-4 cm. The mucosa transitions from simple columnar to stratified squamous epithelium at the dentate (pectinate) line. The anal canal contains the internal anal sphincter (involuntary, smooth muscle) and external anal sphincter (voluntary, striated muscle).
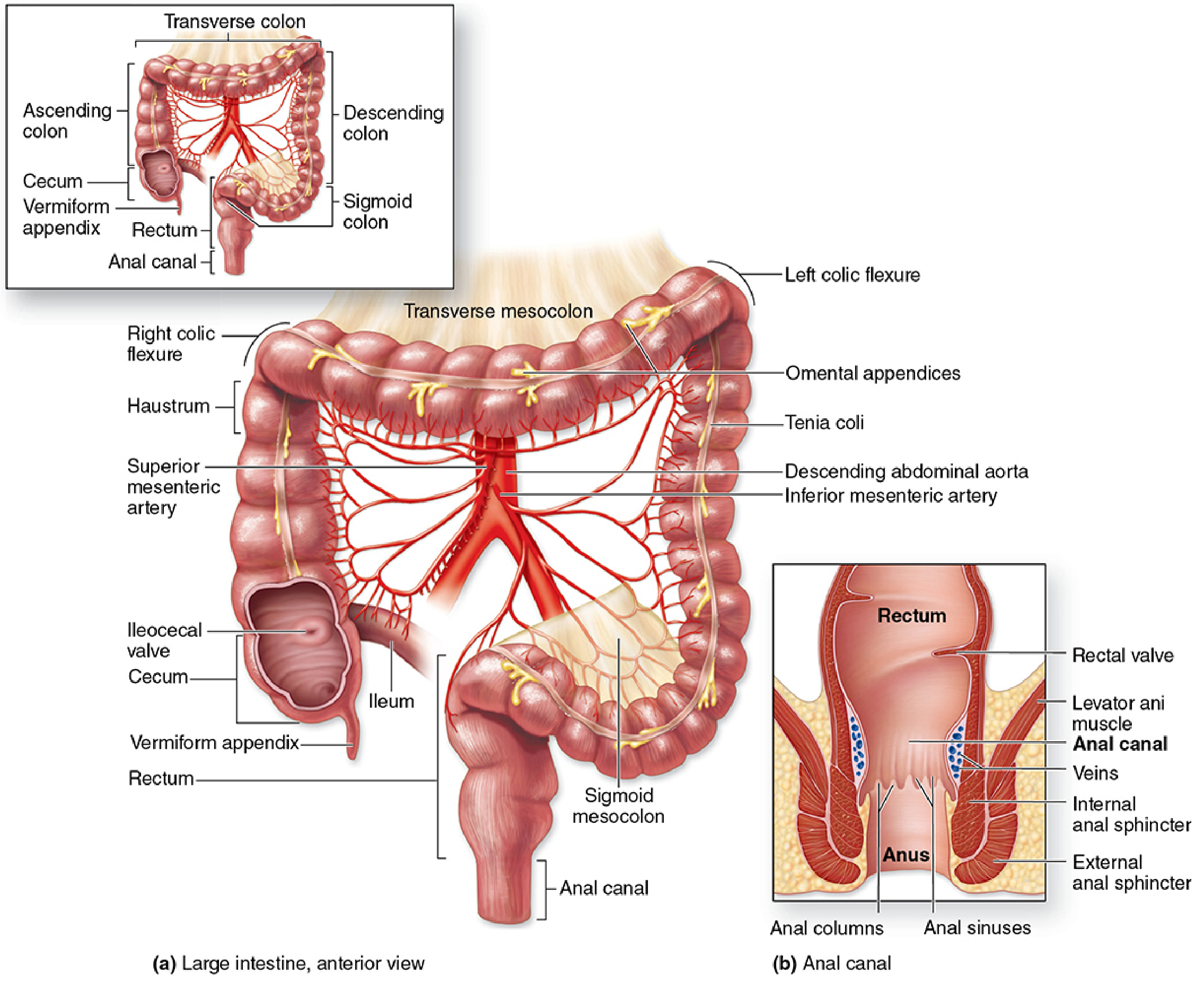
Fig: Large intestine with vascular supply and anal canal detail. Source: Junqueira's Basic Histology 17e
2. Distinguishing Features of the Large Intestine
Three external features immediately distinguish the colon from the small intestine:
1. Taeniae coli: The longitudinal smooth muscle layer is condensed into three narrow bands (rather than a continuous sheet). Running the full length of the cecum and colon, they are approximately 1 cm wide each. Because the taeniae are shorter than the colon wall, they cause the wall to pucker.
2. Haustra (haustra coli): The sacculations or outpocketings created by the puckering of the taeniae coli. They give the colon its characteristic scalloped appearance on X-ray. In the rectum, the taeniae merge back into a complete longitudinal muscle layer, so the rectum lacks haustra.
3. Omental appendices (epiploic appendages): Small, peritoneum-covered fat deposits attached to the outer surface of the colon. They are particularly prominent on the transverse and sigmoid colon.
The large intestine lacks villi - the mucosa is flat, with only shallow folds (plicae semilunares). The large intestinal surface area is approximately 25 m² compared to 200 m² for the small intestine.
3. Histology of the Large Intestine
The large intestine wall has the same four-layer organization as the small intestine, but with key differences:
- No villi - the luminal surface is relatively flat
- Abundant tubular intestinal glands (crypts of Lieberkühn) penetrate the full thickness of the mucosa
- Colonocytes (absorptive cells) have irregular microvilli and dilated intercellular spaces, indicating active water transport. Water absorption is passive, following active Na⁺ transport from the basolateral surface
- Goblet cells become increasingly numerous from cecum to rectum, producing large amounts of lubricating mucus to ease fecal passage
- Muscularis externa: Inner circular layer is continuous, but the outer longitudinal layer is condensed into the three taeniae coli
- Anal transitional zone: At the rectoanal junction, the simple columnar epithelium transitions to stratified squamous. Anal columns (columns of Morgagni) are longitudinal mucosal folds in the anal canal; between them are the anal sinuses. The submucosa here contains the rectal venous plexus (distension of these veins = hemorrhoids).
4. Functions of the Large Intestine
Water and Electrolyte Absorption
This is the primary function. The colon receives approximately 1.5 L of fluid per day from the ileum, and reduces this to just 100-200 mL in feces. Na⁺ is actively transported out of the lumen, and water follows osmotically. The colon also actively secretes K⁺, which is why severe diarrhea causes hypokalemia.
Microbiome and Fermentation
The colon hosts the body's largest and most diverse microbial community - an estimated 500-800 mL biomass with a daily turnover of 100-200 mL. Colonic bacteria ferment:
- Dietary fiber (non-digestible carbohydrates) → short-chain fatty acids (SCFAs: acetate, propionate, butyrate), CO₂, H₂, methane
- Butyrate is the primary energy source for colonocytes and has anti-inflammatory and anti-cancer properties
- Gas production increases rapidly after fermentable residues enter the colon - Sleisenger & Fordtran's GI and Liver Disease
Feces Formation
The residue from digestion, combined with dead bacteria, shed epithelial cells, bile pigments (giving stool its brown color), and mucus, is compacted into feces in the descending and sigmoid colon.
5. Motility of the Large Intestine
- Haustral shuttling: Contents are moved back and forth between haustra to maximize water absorption - slow, non-propulsive
- Mass movements (mass peristalsis): Powerful propulsive contractions that move colonic contents a long distance (several segments at once) toward the rectum. Occur 1-3 times per day, typically triggered by eating (gastrocolic reflex).
- Defecation reflex: When feces enter the rectum and distend it, stretch receptors trigger the urge to defecate. The internal anal sphincter relaxes (involuntary). Defecation is completed voluntarily by contraction of abdominal muscles and relaxation of the external anal sphincter.
- Total transit time through the large intestine: 12-72 hours (highly variable).
6. Blood Supply
| Structure | Arterial Supply | Venous Drainage |
|---|---|---|
| Small intestine | Superior mesenteric artery (SMA) | Superior mesenteric vein → portal vein |
| Cecum, ascending colon, right 2/3 transverse colon | SMA (ileocolic, right colic, middle colic arteries) | Superior mesenteric vein |
| Left 1/3 transverse colon, descending, sigmoid | Inferior mesenteric artery (IMA) | Inferior mesenteric vein → portal vein |
| Rectum/anal canal (upper) | Superior rectal artery (from IMA) | Superior rectal vein → portal vein |
| Rectum/anal canal (lower) | Middle/inferior rectal arteries | Middle/inferior rectal veins → systemic (IVC) |
The junction between SMA and IMA territories (around the splenic flexure) is a watershed area prone to ischemia during low-flow states.
7. Key Comparison Table
| Feature | Small Intestine | Large Intestine |
|---|---|---|
| Length | ~6 m | ~1.5 m |
| Diameter | 2.5-4 cm | 6-7 cm |
| Absorptive surface area | ~200 m² | ~25 m² |
| Villi | Present | Absent |
| Crypts of Lieberkühn | Present | Present |
| Microvilli | Present | Present (less regular) |
| Longitudinal muscle | Complete layer | Condensed into 3 taeniae coli |
| Haustra | Absent | Present |
| Paneth cells | Present (ileum) | Absent |
| Goblet cells | Moderate, increasing distally | Abundant (especially in rectum) |
| Primary function | Digestion and nutrient absorption | Water/electrolyte absorption + feces formation |
| Nutrient absorption | Yes (all macronutrients) | No |
| K⁺ secretion | No | Yes (active) |
| Transit time | 2-6 hours | 12-72 hours |
8. Clinically Important Conditions
| Condition | Segment Affected | Brief Mechanism |
|---|---|---|
| Celiac disease | Small intestine (duodenum/jejunum) | Immune-mediated destruction of villi; malabsorption of all nutrients |
| Crohn's disease | Any segment (skip lesions); often terminal ileum | Transmural granulomatous inflammation; B12 and bile salt malabsorption |
| Ulcerative colitis | Large intestine (rectum spreading proximally) | Mucosal/submucosal inflammation; bloody diarrhea |
| Appendicitis | Appendix | Obstruction (fecalith or lymphoid hyperplasia) → bacterial invasion → perforation risk |
| Colorectal cancer | Large intestine (rectum, sigmoid most common) | Adenomatous polyps → adenocarcinoma; linked to low-fiber diet |
| Hemorrhoids | Anal canal | Swollen rectal venous plexus from constipation, low fiber, straining |
| Intestinal obstruction | Any | Mechanical (adhesions, hernia, tumor) or functional (ileus) |
| Lactase deficiency | Small intestine (brush border) | Absent brush-border lactase → osmotic + fermentative diarrhea |
References:
- Gray's Anatomy for Students, pp. 379-382 (Large Intestine Anatomy)
- Costanzo Physiology 7e, pp. 380-386 (Digestion, Absorption, Small Intestine Structure)
- Medical Physiology (Boron & Boulpaep), pp. 1338-1339 (Surface Area Amplification, Structural Comparison)
- Junqueira's Basic Histology 17e, pp. 793-798 (Large Intestine Histology)
- Histology: A Text and Atlas (Pawlina), pp. 1519-1634 (GI Tract Histology)
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease, pp. 245-246 (Colonic Microbiome and Gas)
This is a shared conversation. Sign in to Orris to start your own chat.