
Solve with reason
Answer: B — Acute anterior MI
Reasoning, step by step:
1. Symptoms point to ACS
- Central chest pain radiating to the jaw = classic ischaemic pain (vagal referral along C3–C5 dermatomes shared with the jaw)
- Sweating (diaphoresis) and vomiting = sympathetic/vagal activation seen in acute MI
- Age 55, male = high-risk demographic
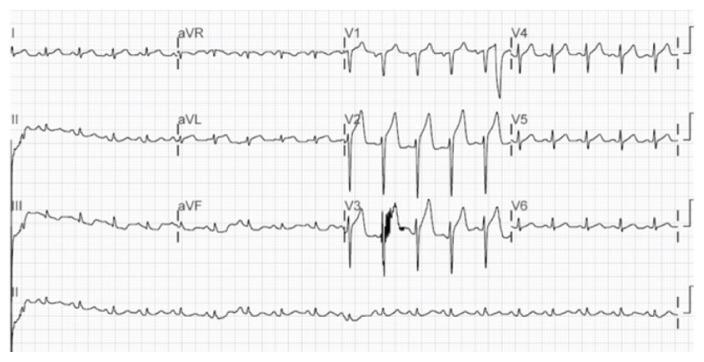
2. ECG is the key discriminator
| Lead group | Territory | Artery |
|---|---|---|
| V1–V4 (anterior) | Anterior LV wall + septum | LAD (Left Anterior Descending) |
| II, III, aVF (inferior) | Inferior LV wall | RCA or LCx |
| I, aVL, V5–V6 (lateral) | Lateral LV wall | LCx |
ST elevation in V1–V4 localises the infarct to the anterior wall, supplied by the LAD. This is the hallmark of an anterior STEMI.
3. Why the other options are wrong
| Option | Why excluded |
|---|---|
| A – Unstable angina | UA causes ST depression or no ST change — never ST elevation. No troponin rise expected. |
| C – Acute inferior MI | Inferior MI shows ST elevation in leads II, III, aVF, not V1–V4. |
| D – Pericarditis | Pericarditis causes diffuse (saddle-shaped) ST elevation in multiple lead groups simultaneously, plus PR depression. It is rarely this focal. |
Conclusion: ST elevation in V1–V4 + classic ischaemic symptoms = Acute Anterior STEMI (LAD occlusion) → Answer B.
Also explain the discussed topic
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching Images
anterior STEMI ST elevation V1 V4 ECG leads LAD occlusion
Loading Image
Loading Image
Finding Sources
Here is a comprehensive explanation of the full topic: Acute Anterior STEMI (ST-Elevation Myocardial Infarction)
Acute Myocardial Infarction — Complete Overview
1. Definition
A Myocardial Infarction (MI) is the irreversible death (necrosis) of cardiac muscle caused by sustained ischemia — most commonly due to sudden occlusion of a coronary artery. When this is accompanied by ST-elevation on ECG, it is termed a STEMI (ST-Elevation MI).
"MI is the death of cardiac muscle due to prolonged ischemia." — Robbins & Kumar Pathologic Basis of Disease
2. Epidemiology
- ~800,000 MIs/year in the US (nearly 1 every 40 seconds)
- 10% occur under age 40; 45% under age 65
- Males are at higher risk until menopause, after which female risk rises significantly
- Risk factors: atherosclerosis, hypertension, dyslipidemia, diabetes, smoking, family history
3. Pathogenesis (How It Happens)
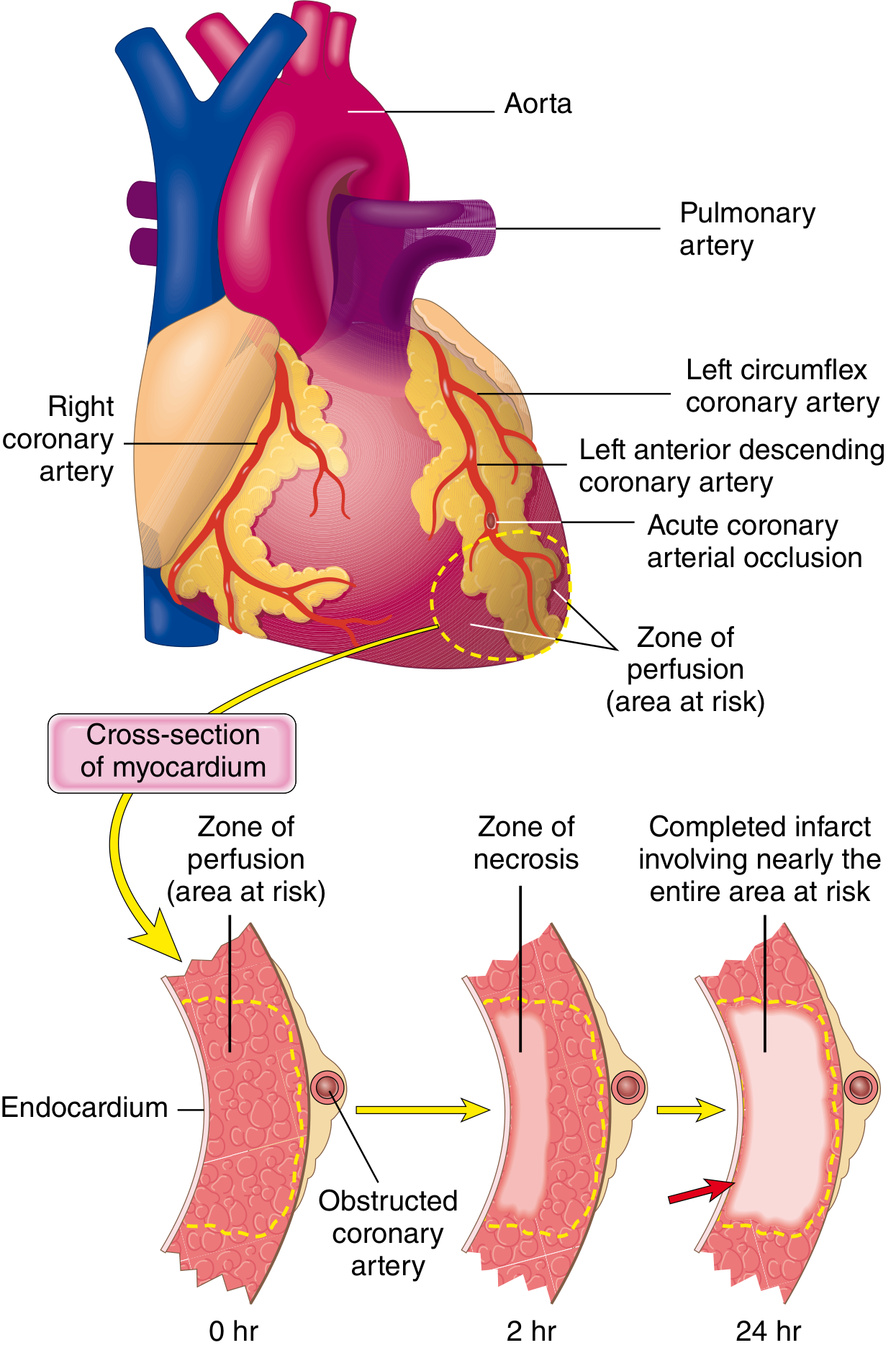
The sequence of events:
- Atherosclerotic plaque in a coronary artery ruptures or erodes
- Exposed collagen → platelet adhesion and aggregation → release of thromboxane A₂, ADP, serotonin
- Coagulation cascade activates → growing thrombus
- Complete occlusion of the coronary artery within minutes
Timeline of cellular injury:
| Event | Time |
|---|---|
| Onset of ATP depletion | Seconds |
| Loss of contractility | < 2 minutes |
| ATP reduced to 50% normal | 10 minutes |
| Irreversible cell injury (necrosis) | 20–40 minutes |
| Microvascular injury | > 1 hour |
| Complete necrosis | 6–12 hours |
This is why "time is muscle" — every minute of delay destroys more myocardium. — Robbins & Kumar
4. Coronary Artery Territories and ECG Localisation
The heart has 3 main coronary arteries, each supplying a specific wall:
| Coronary Artery | Wall Supplied | ECG Leads |
|---|---|---|
| LAD (Left Anterior Descending) | Anterior LV + septum | V1–V4 |
| RCA (Right Coronary Artery) | Inferior LV + RV | II, III, aVF |
| LCx (Left Circumflex) | Lateral LV | I, aVL, V5–V6 |
In this case → ST elevation in V1–V4 = LAD occlusion = Anterior STEMI
5. Why Does ST Elevation Occur?

Three simultaneous electrical changes occur in infarcted cells:
| Defect in Infarcted Cells | Current Flow | ECG Change |
|---|---|---|
| Rapid repolarization (K⁺ channels open) | Out of infarct | ST elevation |
| Decreased resting membrane potential | Into infarct during diastole | TQ depression (recorded as ST elevation) |
| Delayed depolarization | Out of infarct | ST elevation |
All three produce current of injury that causes ST segment elevation in leads overlying the infarcted zone. Leads on the opposite side show reciprocal ST depression.
"The hallmark of acute myocardial infarction is elevation of the ST segments in the leads overlying the area of infarction." — Ganong's Review of Medical Physiology
6. Evolution of ECG Changes Over Time
| Stage | Time | ECG Change |
|---|---|---|
| Hyperacute | First minutes–hours | Tall, peaked (hyperacute) T-waves |
| Acute | Hours | ST elevation, possible new Q waves |
| Subacute | Days | ST normalises, T-wave inversions develop |
| Chronic/Old | Weeks–months | Persistent Q waves (scar), T-waves may normalise |
7. Clinical Presentation
| Feature | Typical in MI |
|---|---|
| Chest pain | Central, crushing, "pressure-like"; >20 min |
| Radiation | Jaw, left arm, neck, back |
| Diaphoresis | Sympathetic activation |
| Nausea/vomiting | Vagal activation (especially inferior MI) |
| Dyspnoea | Due to pump failure |
| Hypotension | Cardiogenic shock in large MIs |
8. Diagnosis
3 Pillars:
- Symptoms — ischaemic chest pain
- ECG — ST elevation ≥1 mm in ≥2 contiguous leads (≥2 mm in V1–V3)
- Biomarkers — Rising troponin I/T (most sensitive and specific); also CK-MB, myoglobin
Unstable angina = ischaemic symptoms + no ST elevation + no troponin rise NSTEMI = ischaemic symptoms + no ST elevation + troponin POSITIVE STEMI = ischaemic symptoms + ST elevation + troponin POSITIVE
9. Distinguishing the 4 Answer Choices
| Condition | ECG Pattern | Key Feature |
|---|---|---|
| Unstable Angina | ST depression or normal | No troponin rise; no ST elevation |
| Acute Anterior MI ✓ | ST elevation V1–V4 | LAD occlusion; troponin rises |
| Acute Inferior MI | ST elevation II, III, aVF | RCA/LCx occlusion |
| Pericarditis | Diffuse saddle-shaped ST elevation in nearly all leads + PR depression | Not territory-specific; positional pain |
10. Management (STEMI Protocol)
The goal is rapid reperfusion — ideally within 90 minutes of first medical contact:
- Aspirin 300 mg + P2Y12 inhibitor (clopidogrel/ticagrelor)
- Anticoagulation (heparin/enoxaparin)
- Primary PCI (percutaneous coronary intervention) — preferred if available within 120 min
- Thrombolysis (e.g., streptokinase, alteplase) — if PCI unavailable within 120 min
- Beta-blockers, ACE inhibitors, statins — initiated early
- Oxygen only if SpO₂ < 90%
- Morphine/nitrates for pain (nitrates contraindicated in RV infarct)
"The benefits of reperfusion are greatest when it is achieved quickly." — Robbins & Kumar
Summary
This patient has a classic anterior STEMI caused by LAD occlusion:
- Central chest pain + jaw radiation + sweating + vomiting → ischaemic ACS presentation
- ST elevation in V1–V4 → anterior wall injury (LAD territory)
- This is a medical emergency requiring immediate reperfusion therapy (primary PCI)
This is a shared conversation. Sign in to Orris to start your own chat.