Antiviral drugs used in OBG 1) ART drugs A) NRTIs i) Zidovudine (AZT) ii) Lamivudine iii) Tenofovir B) NNRTIs i) Efavirenz ii) Nevirapine (NVP) C) Protease Inhibitors i) Lopinavir D) Integrase inhibitors i) Dolutigravir Anti Hepatitis drugs i) Lamivudine ii) Tenofovir
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive notes covering all the antiviral drugs used in OBG that you listed:
Antiviral Drugs in Obstetrics & Gynaecology
PART 1: ANTIRETROVIRAL THERAPY (ART) DRUGS
The goal of ART in OBG is Prevention of Mother-to-Child Transmission (PMTCT) of HIV, also called prevention of vertical transmission. All pregnant women with HIV should be on effective ART.
The general principle: the same ART regimen recommended for nonpregnant adults applies in pregnancy, with some important exceptions noted below.
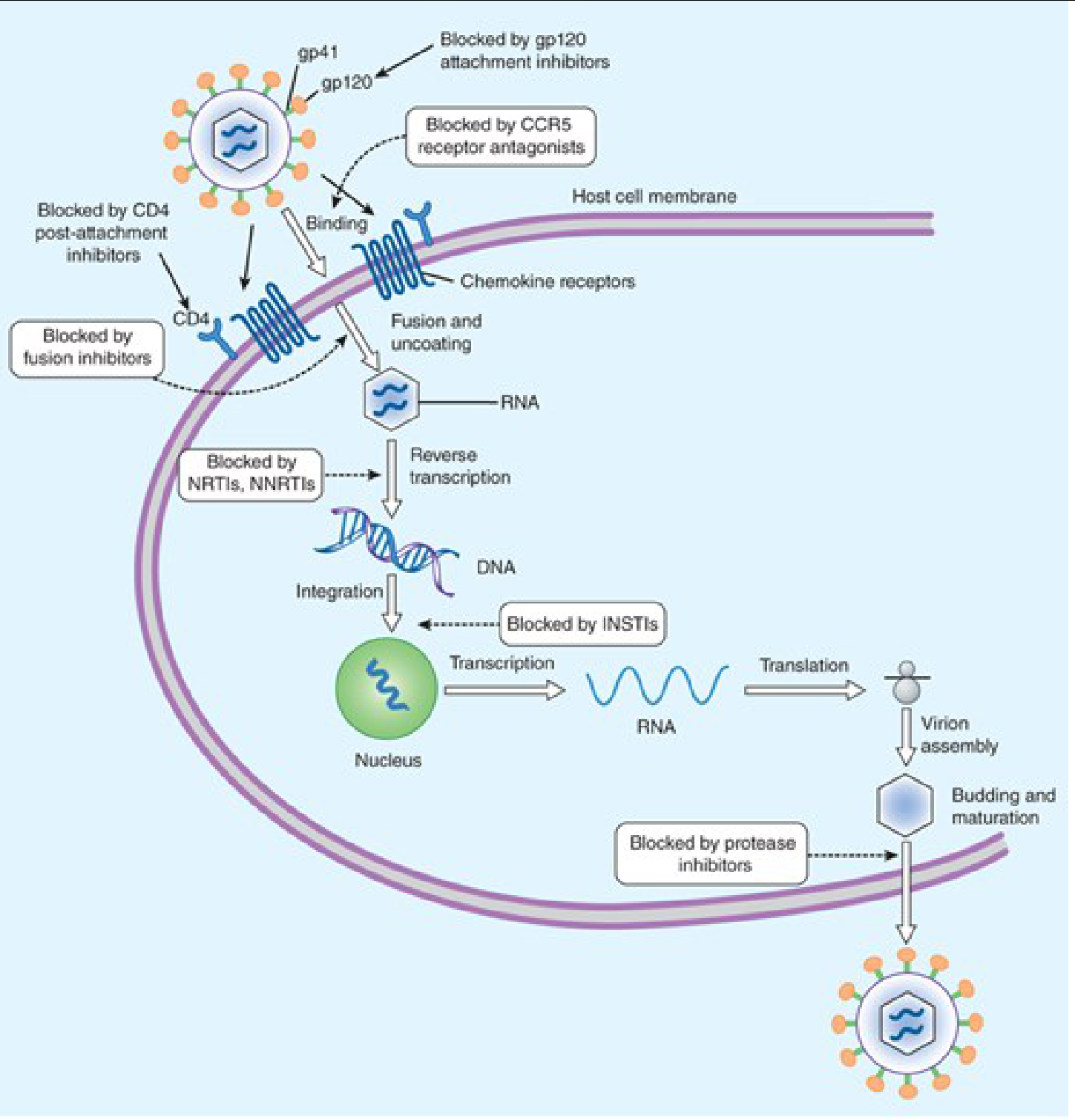
A) NRTIs - Nucleoside/Nucleotide Reverse Transcriptase Inhibitors
Mechanism of Action:
- Require intracellular phosphorylation to their active triphosphate form
- Act as chain terminators - they lack a 3'-hydroxyl group, so they terminate DNA elongation once incorporated
- Competitively inhibit HIV reverse transcriptase (the enzyme that converts viral RNA into DNA)
i) Zidovudine (AZT / ZDV)
| Feature | Detail |
|---|---|
| Class | NRTI (thymidine analogue) |
| Historical landmark | First antiretroviral drug approved (1987); first proven for PMTCT |
| OBG use | Reduce perinatal (vertical) HIV transmission |
| PMTCT efficacy | AZT regimen (maternal + intrapartum + neonatal) reduced perinatal transmission by 65-75% - from ~25% to <2% |
| Route | Oral (also IV intrapartum) |
| Dose in pregnancy | 300 mg twice daily orally; IV ZDV during labor in women with viral load >1000 copies/mL (historical recommendation - now oral ART continued if VL undetectable) |
| Neonatal dosing | ZDV for 6 weeks after birth (+ 3 doses nevirapine in first week if high-risk) |
Key adverse effects:
- Bone marrow suppression - anemia (most important; dose-limiting), neutropenia
- Myopathy (with prolonged use)
- Headache, nausea, fatigue
- Nail pigmentation (melanonychia)
- Lactic acidosis (rare but serious - class effect of NRTIs)
Note: AZT reduces transmission at all levels of maternal viral load. Even a short course reduces transmission by ~50%.
- Jawetz Melnick & Adelbergs Medical Microbiology 28E, p.673
- Creasy & Resnik's Maternal-Fetal Medicine, p.1174
ii) Lamivudine (3TC)
| Feature | Detail |
|---|---|
| Class | NRTI (cytidine analogue) |
| OBG use | Component of preferred ART regimens in HIV-positive pregnant women; also used in Hepatitis B in pregnancy |
| Route | Oral, once or twice daily |
| HIV dose | 300 mg/day (150 mg BD) |
| HBV dose | 100 mg/day |
OBG significance:
- Part of standard combination ART regimens alongside tenofovir + dolutegravir (TLD)
- For Hepatitis B in pregnancy: lamivudine administered in the last trimester reduces perinatal HBV transmission in women with high viral loads
- Safety in pregnancy: Not teratogenic in animal studies; used safely in HIV and HBV-infected pregnant women
Resistance concern:
- With long-term monotherapy for HBV, YMDD mutations develop (M204V/I) at a rate of 15-30%/year, reaching 70% by year 5 - this is why it is no longer preferred as first-line monotherapy for HBV
- HIV resistance also emerges rapidly with lamivudine monotherapy
Adverse effects: Generally well-tolerated; headache, nausea, fatigue; lactic acidosis (rare)
- Harrison's Principles of Internal Medicine 22E (2025), p. HBV chapter
iii) Tenofovir (TDF / TAF)
| Feature | Detail |
|---|---|
| Class | NRTI - nucleotide analogue (prodrug) |
| Forms | TDF = Tenofovir Disoproxil Fumarate; TAF = Tenofovir Alafenamide |
| OBG use | Preferred NRTI in pregnancy (HIV); drug of choice for HBV in pregnancy |
| Route | Oral, once daily |
HIV in pregnancy:
- TDF is a recommended NRTI backbone in pregnancy as part of combination ART (e.g., TDF + 3TC + DTG = TLD regimen)
- TDF + Emtricitabine (FTC) = the only FDA-approved combination for PrEP (pre-exposure prophylaxis) - recommended for HIV-negative women at high risk, including pregnant/breastfeeding women
HBV in pregnancy:
- Tenofovir disoproxil fumarate is the current drug of choice for hepatitis B treatment in pregnancy
- RCTs and meta-analyses confirm it is safe for mother and infant, and effective in reducing mother-to-child transmission of HBV when given in the 2nd/3rd trimester to women with high viremia
- TAF has less renal and bone toxicity than TDF; also approved for HBV
Adverse effects of TDF:
- GI symptoms (nausea, vomiting, flatulence)
- Nephrotoxicity - Fanconi syndrome, acute renal failure, nephrogenic diabetes insipidus; monitor creatinine
- Bone demineralization / loss of bone mineral density (proximal renal tubulopathy causes renal phosphate/calcium wasting)
- Not recommended in patients with pre-existing renal/bone disease
TAF advantages over TDF: ~90% lower plasma tenofovir concentrations; less renal and bone toxicity; but more weight gain and lipid elevation.
- Katzung's Basic & Clinical Pharmacology 16th Ed., p.1362
- Harrison's Principles of Internal Medicine 22E (2025)
- Yamada's Textbook of Gastroenterology 7th Ed.
B) NNRTIs - Non-Nucleoside Reverse Transcriptase Inhibitors
Mechanism of Action:
- Bind directly and allosterically to HIV-1 reverse transcriptase at a site near (but distinct from) the NRTI binding site
- Cause conformational change that inhibits RNA-dependent and DNA-dependent DNA polymerase activity
- Do NOT require intracellular phosphorylation (unlike NRTIs)
- Do NOT compete with nucleoside triphosphates (unlike NRTIs)
- Active only against HIV-1 (not HIV-2)
Class effects:
- Long half-life (>24 hours for most) - allows once daily dosing
- Metabolized by CYP450 system - significant drug interactions
- Skin rash (can rarely be severe: Stevens-Johnson syndrome)
- Resistance: single point mutation can cause resistance; K103N and Y181C are common
i) Efavirenz (EFV)
| Feature | Detail |
|---|---|
| Class | NNRTI (1st generation) |
| OBG use | Previously a component of standard first-line ART (now being replaced by dolutegravir-based regimens) |
| Dose | 600 mg once daily at night |
| Metabolism | CYP3A4 substrate; mixed inducer/inhibitor |
Key OBG considerations:
- Teratogenicity concerns: Early case reports suggested neural tube defects with first-trimester use; however, larger studies showed no clear signal. Current WHO/DHHS guidelines now permit its use in pregnancy when no safer alternative is available, but it is NOT the preferred agent - dolutegravir-based regimens are preferred
- Avoid in first trimester if possible (historical precaution still observed in many guidelines)
- CNS side effects: vivid dreams, dizziness, insomnia, mood disturbance - may affect adherence
Adverse effects:
- CNS effects (most common) - vivid dreams, dizziness, confusion, depression (take at bedtime to reduce)
- Rash (5-10%; usually mild)
- Hepatotoxicity
- Hyperlipidemia
- CYP inducer - reduces levels of oral contraceptives, methadone, many other drugs
ii) Nevirapine (NVP)
| Feature | Detail |
|---|---|
| Class | NNRTI (1st generation) |
| Historical OBG use | Single-dose NVP to mother at onset of labor + single dose to neonate reduced PMTCT by ~50% - the "HIVNET 012" regimen used widely in developing countries |
| Current use | Neonatal prophylaxis (3 doses in first week of life for high-risk infants), as part of combination regimens |
| Dose | 200 mg/day for 14 days, then 200 mg BD (lead-in to reduce rash) |
Key OBG considerations:
- Single-dose NVP (SD-NVP) has been the backbone of PMTCT programs in resource-limited settings due to low cost and simplicity
- Risk of NNRTI resistance after SD-NVP use - can compromise future NVP/EFV-based ART if resistance mutations persist
- Induction of CYP3A4 - major drug interactions; reduces levels of many drugs
Adverse effects:
- Hepatotoxicity - most serious adverse effect, especially in the first 18 weeks; fatal hepatic necrosis reported - risk higher in women with CD4 >250 cells/mm³ (do NOT initiate NVP in women with CD4 >250 for treatment purposes)
- Skin rash - common; the 14-day lead-in dose reduces rash incidence; Stevens-Johnson syndrome possible
- Fever, nausea
C) Protease Inhibitors (PIs)
Mechanism of Action:
- Inhibit HIV aspartyl protease, which is responsible for the post-translational cleavage of the Gag-Pol polyprotein into individual functional proteins
- Without protease, immature, non-infectious virions are produced (viral budding occurs but maturation is blocked)
- Act at a late stage of the HIV life cycle (after integration)
i) Lopinavir/Ritonavir (LPV/r)
| Feature | Detail |
|---|---|
| Class | Protease Inhibitor (co-formulated with ritonavir as pharmacokinetic booster) |
| OBG use | Second-line PI-based ART during pregnancy (now largely replaced) |
| Dose | LPV 400 mg / RTV 100 mg twice daily |
Key OBG considerations:
- Lopinavir is always co-administered with ritonavir (a low-dose "booster") which inhibits CYP3A4, increasing LPV plasma levels significantly
- LPV/r was historically used in pregnancy but is now not the preferred PI - darunavir/ritonavir (DRV/r) or atazanavir/ritonavir (ATV/r) are preferred when a PI-based regimen is required
- LPV/r-based regimens may increase risk of prematurity compared to other regimens
Adverse effects:
-
GI intolerance (nausea, diarrhea) - very common
-
Dyslipidemia (hypercholesterolemia, hypertriglyceridemia)
-
Hepatotoxicity
-
Lipodystrophy (fat redistribution - buffalo hump, central obesity, lipoatrophy)
-
Insulin resistance / hyperglycemia - early glucose screening recommended in pregnancy in women on PI-based regimens
-
Prolonged PR interval
-
Creasy & Resnik's Maternal-Fetal Medicine, p.1174
D) Integrase Inhibitors (INSTIs)
Mechanism of Action:
- Inhibit HIV integrase - the viral enzyme that catalyzes the integration of viral double-stranded DNA into the host cell genome
- Specifically block the strand transfer reaction (catalytic step of integration) - hence also called INSTIs (Integrase Strand Transfer Inhibitors)
- Once integration is blocked, proviral DNA cannot be established, and viral replication is halted
i) Dolutegravir (DTG)
| Feature | Detail |
|---|---|
| Class | INSTI (2nd generation) |
| OBG use | Currently the PREFERRED antiretroviral in pregnancy - drug of choice in combination ART regimens |
| Dose | 50 mg once daily (50 mg BD if on certain interacting drugs) |
| Standard regimen | TDF + 3TC + DTG (TLD) - WHO preferred first-line ART |
Why preferred in OBG?
- High potency and rapid virologic suppression
- High genetic barrier to resistance (unlike NNRTIs, requires multiple mutations)
- Favorable tolerability
- Once-daily dosing
- Per Creasy & Resnik: "Integrase strand transfer inhibitor-based antiretrovirals have become the treatment of choice during pregnancy, and treatment recommendations emphasize that the same ART regimen should be used in both pregnant and nonpregnant women, with dolutegravir being the preferred INSTI drug of choice."
Safety concern (historical):
- Early 2018 Botswana data raised concerns about neural tube defects (NTDs) with peri-conception DTG use (~0.9% vs ~0.1% background rate)
- Subsequent larger studies and meta-analyses have substantially reassured - the risk is very small and the benefits outweigh risks
- Current WHO/DHHS (2020+) guidelines recommend DTG in all trimesters including first trimester
- Folic acid supplementation is advised for all women of childbearing age on DTG
Adverse effects:
- Generally very well tolerated
- Insomnia, headache
- Mild weight gain
- Rarely: hypersensitivity reactions
PART 2: ANTI-HEPATITIS DRUGS IN OBG
The main concern in OBG is prevention of mother-to-child transmission (MTCT) of Hepatitis B Virus (HBV).
Context:
- Infants born to HBsAg-positive mothers should receive HBV vaccine + HBIG (Hepatitis B Immunoglobulin) within 12 hours of birth
- Antiviral therapy is added when maternal HBV DNA (viral load) is high (typically >200,000 IU/mL or >10^6 copies/mL) to reduce MTCT further
- Treatment is usually started at 28-32 weeks gestation and continued for 4-12 weeks postpartum
i) Lamivudine (for Hepatitis B)
| Feature | Detail |
|---|---|
| Mechanism | Inhibits HBV DNA polymerase (same cytidine analogue mechanism as in HIV) |
| Use in HBV pregnancy | Reduces perinatal HBV transmission when given in last trimester to mothers with high viremia |
| Evidence | RCTs and meta-analyses confirm efficacy and safety |
Limitations:
-
High resistance rate (YMDD mutations) with long-term use
-
No longer recommended as first-line for chronic HBV - largely replaced by tenofovir (which has superior resistance profile)
-
Still used in resource-limited settings due to low cost
-
Safety in pregnancy: not teratogenic in animal studies; used safely in practice
-
Harrison's Principles of Internal Medicine 22E (2025)
ii) Tenofovir (for Hepatitis B)
| Feature | Detail |
|---|---|
| Mechanism | Inhibits HBV DNA polymerase (nucleotide analogue - competes with deoxyadenosine triphosphate) |
| OBG role | Drug of choice for Hepatitis B treatment in pregnancy |
| Form used | Tenofovir disoproxil fumarate (TDF) preferred; TAF also approved for HBV |
Why preferred over lamivudine for HBV in pregnancy?
- Superior potency - more effective suppression of HBV replication
- Minimal resistance - no significant resistance mutations reported even with years of use
- Proven safety in pregnancy (FDA Category B; extensive safety data from HIV-positive pregnant women)
- Effectively reduces risk of perinatal HBV transmission
- RCT evidence confirms: TDF in 3rd trimester significantly reduces infant HBV infection rate even in highly viremic mothers (HBV DNA >200,000 IU/mL)
Monitoring during pregnancy:
-
Renal function (creatinine, urinalysis for proteinuria/glycosuria)
-
HBV DNA levels
-
ALT (watch for post-partum flare when stopping therapy)
-
Yamada's Textbook of Gastroenterology 7th Ed.
-
Harrison's Principles of Internal Medicine 22E (2025)
Quick Summary Table
| Drug | Class | Primary OBG Use | Key Adverse Effect | Preferred in Pregnancy? |
|---|---|---|---|---|
| Zidovudine (AZT) | NRTI | PMTCT - IV/oral during labor & neonatal prophylaxis | Anemia, bone marrow suppression | Alternative (historical backbone) |
| Lamivudine (3TC) | NRTI | HIV combination ART; HBV MTCT prevention | Well tolerated; HBV resistance (YMDD) | Yes (part of TLD) |
| Tenofovir (TDF) | NRTI | HIV ART (PrEP); HBV - drug of choice | Nephrotoxicity, bone loss | Yes - preferred |
| Efavirenz | NNRTI | HIV ART (being phased out in favor of DTG) | CNS effects, rash, teratogen concerns | Avoid 1st trimester; not preferred |
| Nevirapine (NVP) | NNRTI | Neonatal PMTCT prophylaxis (3 doses) | Hepatotoxicity, rash | Neonatal use; avoid initiating in women with CD4 >250 |
| Lopinavir/r | PI | HIV 2nd line (historical) | GI, dyslipidemia, preterm birth risk | Not preferred (DRV/r preferred PI) |
| Dolutegravir (DTG) | INSTI | Preferred ART in pregnancy (TLD regimen) | Generally well tolerated; weight gain | Preferred - 1st line |
| Lamivudine | Anti-HBV | HBV MTCT prevention (resource-limited settings) | HBV resistance common | Alternative |
| Tenofovir | Anti-HBV | Drug of choice for HBV in pregnancy | Nephrotoxicity, bone loss | Drug of choice |
Key OBG Points to Remember
- Current preferred ART regimen in pregnancy: TDF + 3TC + DTG (TLD) - same as non-pregnant adults
- Dolutegravir is the preferred INSTI and the overall preferred third agent in pregnancy (replaced NVP and EFV)
- Tenofovir is both: the backbone NRTI for HIV and the drug of choice for HBV in pregnancy
- Zidovudine: historically pivotal for PMTCT; now mainly used for neonatal prophylaxis (6 weeks) + intrapartum in specific situations
- Nevirapine single dose: still used for neonatal prophylaxis (3 doses in first week for high-risk infants); resist using as maternal treatment if CD4 >250 due to hepatotoxicity risk
- Lopinavir/r: if a PI is needed, prefer DRV/r or ATV/r over LPV/r in pregnancy
- For HBV in pregnancy: vaccine + HBIG to neonate at birth PLUS antiviral (TDF preferred) to the mother if high viral load (>200,000 IU/mL)
- Elective cesarean is recommended for HIV-positive women with viral load >1000 copies/mL at delivery
Sources: Creasy & Resnik's Maternal-Fetal Medicine | Katzung's Basic & Clinical Pharmacology 16th Ed. | Jawetz Melnick & Adelbergs Medical Microbiology 28E | Harrison's Principles of Internal Medicine 22E (2025) | Yamada's Textbook of Gastroenterology 7th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.