Congenital diaphragmatic hernia in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"congenital diaphragmatic hernia"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have all the information needed for a comprehensive, well-cited answer. Let me compile it:
Congenital Diaphragmatic Hernia (CDH)
Definition and Epidemiology
Congenital diaphragmatic hernia (CDH) is a spectrum of developmental conditions marked by a defect in the diaphragm that allows abdominal contents to herniate into the thoracic cavity, disrupting lung and pulmonary vascular development. The reported incidence is approximately 1:2,000 to 5,000 live births, with most cases sporadic, isolated, and non-syndromic.
- Left-sided (Bochdalek): 85% of cases
- Right-sided: 13%
- Bilateral or complete agenesis: <2%
- Isolated CDH (no associated anomalies): ~60% of cases; if associated with other anomalies, mortality exceeds 85%
(Sabiston Textbook of Surgery, p. 2675; Creasy & Resnik's Maternal-Fetal Medicine, p. 776)
Embryology and Types
The diaphragm develops embryologically from four structures:
- Septum transversum
- Pleuroperitoneal folds
- Components of the abdominal wall
- Dorsal mesentery
These begin fusing at 3-4 weeks gestation, separating the pleural and peritoneal cavities. Muscular ingrowth is complete by ~9 weeks gestation. Incomplete fusion at different locations results in distinct hernia types:
| Type | Location | Frequency |
|---|---|---|
| Bochdalek | Posterolateral | 70-75% |
| Morgagni | Anterior/retrosternal | 23-28% |
| Central | Central tendon | 2-7% |
Bochdalek hernias are most common on the left side (85%) because the right side is protected by the early-developing liver. Morgagni hernias are often asymptomatic until childhood or adulthood.
(Sabiston Textbook of Surgery, p. 2675)
Pathophysiology
Once abdominal organs herniate through the defect (during the 2nd trimester), a cascade of consequences occurs:
Pulmonary Hypoplasia
- The ipsilateral lung is compressed and undergoes reduced bronchial branching and reduced alveolar surface area
- The contralateral lung is also affected by compression and intrinsic genetic factors (e.g., FOG2, GATA4 mutations)
- Lungs have smaller bronchi, fewer airway branches, and less alveolar area on both sides
Pulmonary Hypertension
- Pulmonary vascular smooth muscle is hypertrophied, with increased arteriolar wall thickness
- Arteriolar vasculature is hypersensitive to vasoactive stimuli
- This leads to right-to-left shunting (persistent fetal circulation) at the foramen ovale and ductus arteriosus
Cardiac Effects
- Mediastinal shift compresses the contralateral lung and distorts cardiac anatomy
- Significant congenital heart defects co-occur in 25-50% of CDH patients
- Left ventricular hypoplasia may occur from reduced preload
Genetic Associations
- Trisomies, microdeletions, and single gene defects are all possible
- Array CGH detects abnormalities in ~6.3% of CDH cases
- Associated syndromes: Turner syndrome, Fryns syndrome, VACTERL association
(Bailey & Love's Surgery, p. 1763; Creasy & Resnik's, p. 776; Sabiston, p. 2675)
Prenatal Diagnosis and Imaging
Ultrasound screening has led to prenatal diagnosis in roughly two-thirds of cases, sometimes as early as 15 weeks gestation.
Sonographic Features:
- Visualization of stomach, bowel, or liver in the thorax
- Rightward cardiac/mediastinal shift (in left CDH)
- Polyhydramnios
- Absence of the normal stomach bubble below the diaphragm
Right-sided CDH is harder to detect: the liver's echogenicity mimics fetal lung. Doppler of the umbilical vein, hepatic vessels, and gallbladder position are used as landmarks. Cardiac compression and polyhydramnios are indirect signs.
Differential Diagnoses (Prenatal):
- Congenital pulmonary airway malformation (CPAM)
- Bronchopulmonary sequestration
- Bronchogenic/enteric cysts
- Mediastinal teratoma
In all these conditions, intraabdominal organs are NOT displaced.
Upon diagnosis, referral to a tertiary center is mandatory for advanced imaging (MRI for fetal lung volumes), genetic testing, echocardiography, and multidisciplinary counseling.
(Creasy & Resnik's, p. 776)
Prognostic Assessment
Two key prenatal prognostic tools:
1. Lung-to-Head Ratio (LHR)
The contralateral lung area is divided by the head circumference at the level of the atria.
| LHR | Prognosis |
|---|---|
| <1.0 | Poor (severe pulmonary hypoplasia) |
| 1.0-1.4 | Moderate |
| >1.4 | Near 100% survival |
2. Observed-to-Expected LHR (O/E LHR)
Corrects LHR for gestational age using normal reference values:
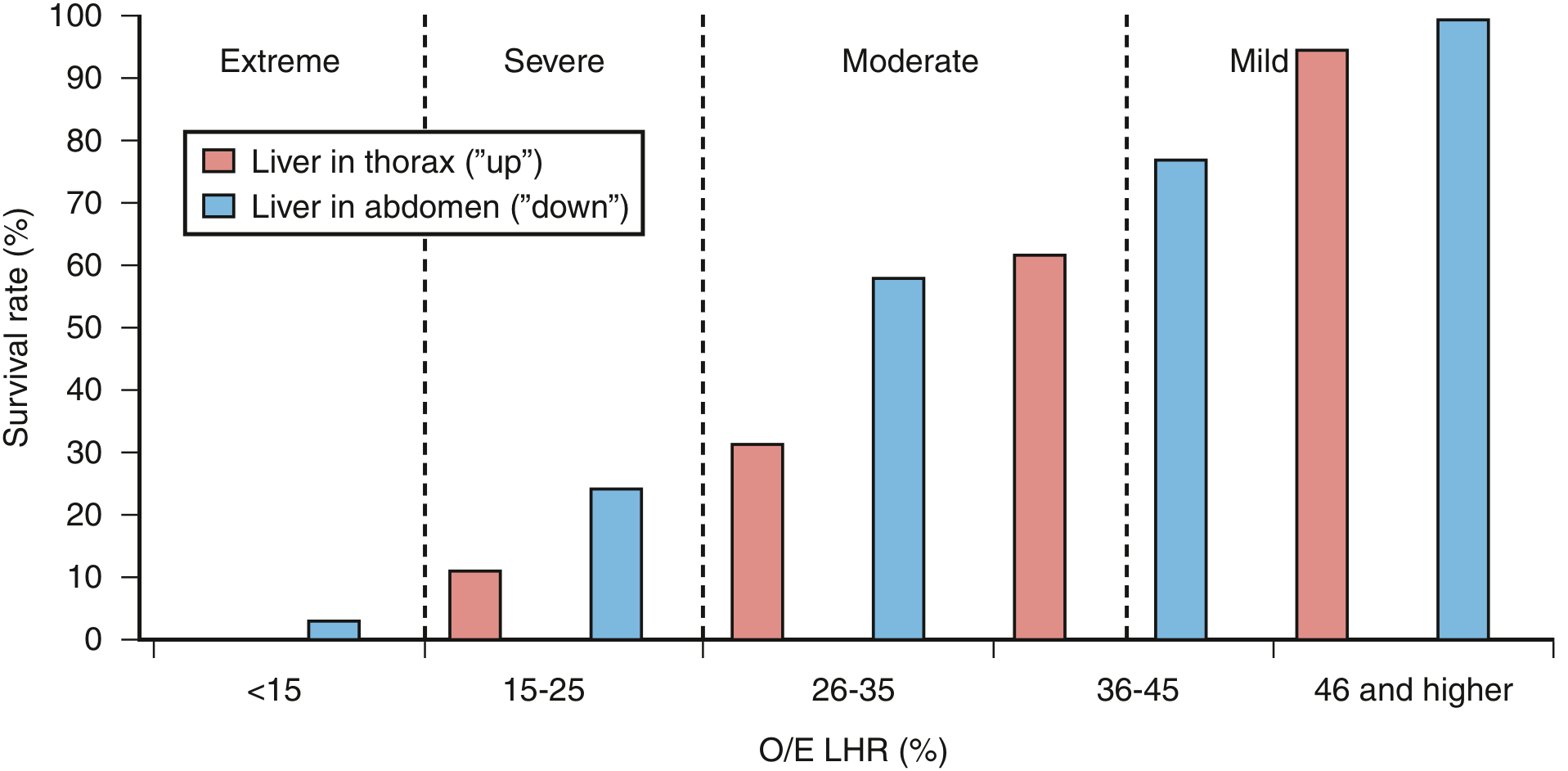
Figure: Relationship between O/E LHR, liver herniation, and survival. Liver "up" (in thorax) consistently worsens prognosis at every LHR category. (Creasy & Resnik's Maternal-Fetal Medicine)
| O/E LHR | Severity | Survival (expectant) |
|---|---|---|
| <15% | Extreme | ~0-3% |
| 15-25% | Severe | ~11-25% |
| 26-35% | Moderate | 31-58% |
| 36-45% | Moderate-mild | 62-77% |
| >46% | Mild | ~95-100% |
Liver herniation ("liver up") independently worsens prognosis at every severity level.
(Creasy & Resnik's, p. 776; Sabiston, p. 2716)
Clinical Presentation (Postnatal)
Classic Neonatal Presentation:
- Persistent respiratory distress at birth
- "Seesaw" or "rocking" respiratory pattern due to severely hypoplastic ipsilateral lung
- Persistent cyanosis and oxygen desaturation
- Scaphoid abdomen (hallmark - abdominal organs are displaced into chest)
- Bowel sounds audible in the chest
- Displacement of heart tones away from side of hernia
- Preductal and post-ductal SpO2 difference indicating right-to-left shunting
Delayed Presentation (10-20% of cases): CDH may present after the first 24 hours with feeding difficulties, recurrent respiratory infections, or pneumonia. Morgagni hernias are often asymptomatic until childhood.
(Sabiston, p. 2675; Tintinalli's Emergency Medicine)
Radiological Findings
Chest X-ray (confirmatory):
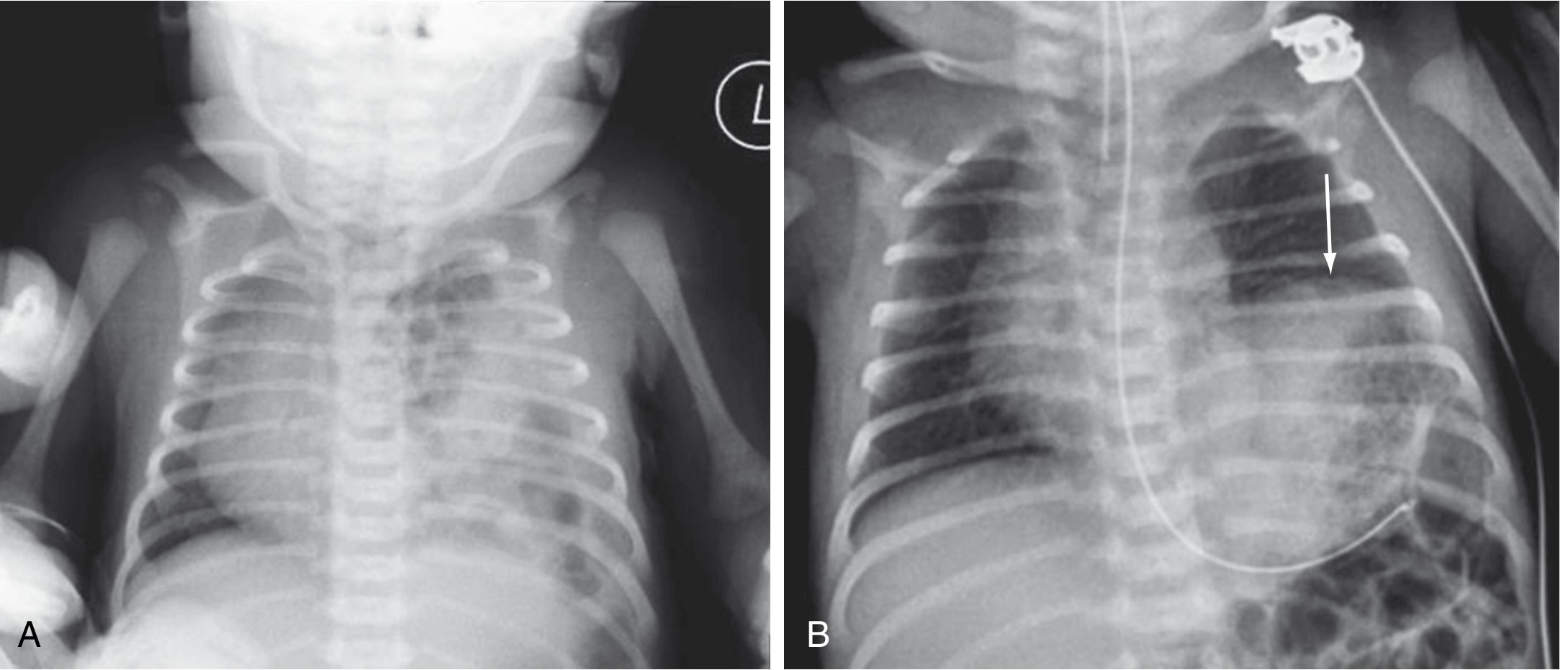
Figure: (A) Left CDH - multiple gas-filled bowel loops in the left hemithorax with mediastinal shift to the right. (B) Left diaphragmatic eventration for comparison (elevated hemidiaphragm, arrow). (Sabiston Textbook of Surgery)
Key X-ray findings:
- Gas-filled bowel loops within the hemithorax
- Mediastinal/cardiac shift to the contralateral side
- Absence or reduction of bowel gas in the abdomen
- Absence of visible diaphragmatic outline
(Sabiston, p. 2675; Grainger & Allison's Diagnostic Radiology)
Management
A. Emergency Stabilization (Birth/ER)
Critical "Do NOT" rule: Bag-mask ventilation is contraindicated - it inflates GI contents in the chest and further compromises ventilation.
Immediate steps:
- Immediate endotracheal intubation - avoid bag-mask ventilation
- Large-bore (10F) orogastric tube on continuous low suction - decompress herniated bowel
- Gentle ventilation: rate 40-50 bpm, lowest peak inspiratory pressure that allows normal chest rise (avoid barotrauma to hypoplastic lungs)
- Target PaCO2 30-35 mmHg (permissive hypercapnia is also acceptable) to reduce pulmonary vascular resistance
- Pulse oximetry monitoring pre- and post-ductal
(Tintinalli's Emergency Medicine)
B. ICU Stabilization - "Gentilation" Protocol
The mainstay is aggressive management of pulmonary hypertension before surgical repair. Surgery does NOT directly correct pulmonary hypertension - the child must be stabilized first.
Ventilation Strategy:
- High-frequency oscillatory ventilation (HFOV) - preferred in severe cases
- Permissive hypercapnia (limiting peak inspiratory pressures)
- Target pH 7.35-7.45, preductal SpO2 >85%
Pulmonary Hypertension Management:
- Inhaled nitric oxide (iNO) - selective pulmonary vasodilator
- Sildenafil (PDE-5 inhibitor) - oral/IV
- Prostacyclin (PGI2) and PGE1 (prostaglandins)
- Milrinone - inotrope + pulmonary vasodilator
- Inotropes for cardiac dysfunction
ECMO (Extracorporeal Membrane Oxygenation):
Reserved for the most severe cases not responding to maximal medical therapy. Used as a bridge to surgical repair or as rescue therapy.
(Sabiston, p. 2676; Miller's Anesthesia; Bailey & Love's)
C. Fetal Intervention - FETO
Fetoscopic Endoluminal Tracheal Occlusion (FETO) is offered at specialized centers for severe CDH:
- A balloon is inserted into the fetal trachea under fetoscopic guidance between the vocal cords and carina
- Typically performed at 27-29 weeks gestation
- Tracheal occlusion prevents lung fluid egress → lung fluid accumulation → lung growth
- Balloon is retrieved fetoscopically or percutaneously at ~34 weeks
- If removal fails, an EXIT procedure at delivery ensures airway patency
TOTAL Trials Results:
- Severe CDH (O/E LHR <25%): FETO improved survival to 40% vs. 15% with expectant management (stopped early for efficacy)
- Moderate CDH (O/E LHR 25-35%): FETO at 30-32 weeks showed no survival benefit over expectant management
Risks of FETO: Preterm labor, premature rupture of membranes (PROM), preterm birth, fetal demise.
(Sabiston, p. 2716; Creasy & Resnik's, p. 776)
D. Surgical Repair
Timing: Surgery is delayed until pulmonary hypertension is controlled and the infant is hemodynamically stable. Unlike traumatic hernias, urgent reduction of bowel in CDH does NOT improve gas exchange.
Approach Options:
| Approach | Route |
|---|---|
| Open subcostal (transabdominal) | Most common for complex cases |
| Thoracoscopic | Minimally invasive option |
| Thoracotomy | Less common |
Technique:
- Herniated viscera (stomach, bowel, occasionally liver/spleen) are reduced back into the abdomen
- The diaphragmatic defect is assessed:
- Small defect: Primary repair with interrupted non-absorbable sutures
- Large defect: Patch repair using Gore-Tex (PTFE) or Silastic/conical patch
- A hernia sac may be present - it can be excised or plicated
- Chest drain placed to expand lung
Anesthesia Considerations:
- Avoid bag-mask ventilation pre-intubation
- High risk of pneumothorax (ipsilateral or contralateral) from barotrauma to hypoplastic lungs
- Avoid hypoxemia and excessive hypercapnia to prevent pulmonary hypertension crisis
- Deep general anesthesia to blunt stress response
(Sabiston, p. 2676; Bailey & Love's, p. 1787; Miller's Anesthesia)
Outcomes and Survival
- Overall survival: 65-90% at specialized centers
- Prenatal diagnosis is paradoxically associated with worse prognosis (larger defects are more visible prenatally)
- Total lung volume >45% of normal is predictive of survival
Chronic Morbidities in Survivors:
| System | Complication |
|---|---|
| Pulmonary | Bronchopulmonary dysplasia (BPD), recurrent respiratory infections, obstructive/restrictive lung disease |
| Cardiovascular | Persistent pulmonary hypertension, left ventricular hypoplasia |
| GI | Gastroesophageal reflux disease (GERD), feeding difficulties |
| Nutritional | Failure to thrive |
| Structural | Thoracic deformity, scoliosis after repair |
| Neurodevelopmental | Hearing loss, developmental delay |
(Creasy & Resnik's, p. 776; Sabiston, p. 2676)
Summary
| Feature | Key Points |
|---|---|
| Incidence | 1:2,000-5,000 births |
| Most common type | Left-sided Bochdalek (85%) |
| Core pathology | Pulmonary hypoplasia + pulmonary hypertension |
| Prenatal diagnosis | Ultrasound (2/3 of cases); confirmed by MRI |
| Key prognostic tool | O/E LHR + liver position |
| Emergency rule | NO bag-mask ventilation; intubate immediately |
| Medical Rx | iNO, sildenafil, HFOV, ECMO for severe cases |
| Fetal intervention | FETO for severe CDH (O/E LHR <25%) |
| Surgery | After stabilization; primary suture or patch repair |
| Survival | 65-90% at tertiary centers |
Sources:
- Sabiston Textbook of Surgery, 21st Ed., pp. 2675-2676, 2716
- Creasy & Resnik's Maternal-Fetal Medicine, pp. 776-778
- Bailey & Love's Short Practice of Surgery, 28th Ed., p. 1763
- Tintinalli's Emergency Medicine
- Miller's Anesthesia, 10th Ed.
- Pye's Surgical Handicraft, 22nd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.