Orris care
- Do you have a medical or health question?
- Are you looking for information about a specific topic?
- Do you need help with a task or document?
Paediatric tuberculosis
"pediatric tuberculosis"[MeSH Terms] AND "diagnosis"[MeSH Terms]
"tuberculosis"[MeSH Terms] AND "child"[MeSH Terms] AND "treatment"
Paediatric Tuberculosis
Epidemiology
- Age <5 years (up to 20% develop disease within 2 years of infection due to an immature immune system)
- Malnutrition
- HIV co-infection
- Immunosuppressive therapy
- Close contact with a smear-positive case
Young age is a specific risk factor for disseminated disease (miliary TB, TB meningitis).
Clinical Features
- Persistent fever ≥2 weeks without a known cause
- Unremitting cough ≥2 weeks
- Weight loss ≥5% in 3 months, or failure to gain weight over 3 months
- Fatigue, night sweats (less prominent than in adults)
- Children rarely produce sputum and are rarely smear-positive
- TB lymphadenitis (most common EPTB in children, esp. cervical)
- TB meningitis
- Miliary TB
- Pleural TB, abdominal TB, osteoarticular TB
Diagnosis
Step 1 - Microbiological Confirmation
- CBNAAT (Cartridge-Based Nucleic Acid Amplification Test - GeneXpert) is the preferred first-line test. It also detects rifampicin resistance.
- If CBNAAT unavailable, use smear microscopy (at least 2 specimens).
- Specimen sources: sputum, gastric aspirate (morning, x3), induced sputum, bronchoalveolar lavage, pleural fluid, CSF, urine, tissue biopsy.
- Culture (solid media up to 10 weeks, liquid media 1-6 weeks) remains the gold standard.
Step 2 - If Microbiological Confirmation Fails
- Chest X-ray - highly suggestive findings include:
- Hilar/mediastinal lymphadenopathy
- Miliary pattern
- Chronic fibrocavitatory shadows
- Tuberculin Skin Test (TST/Mantoux) using 2 TU of PPD RT 23
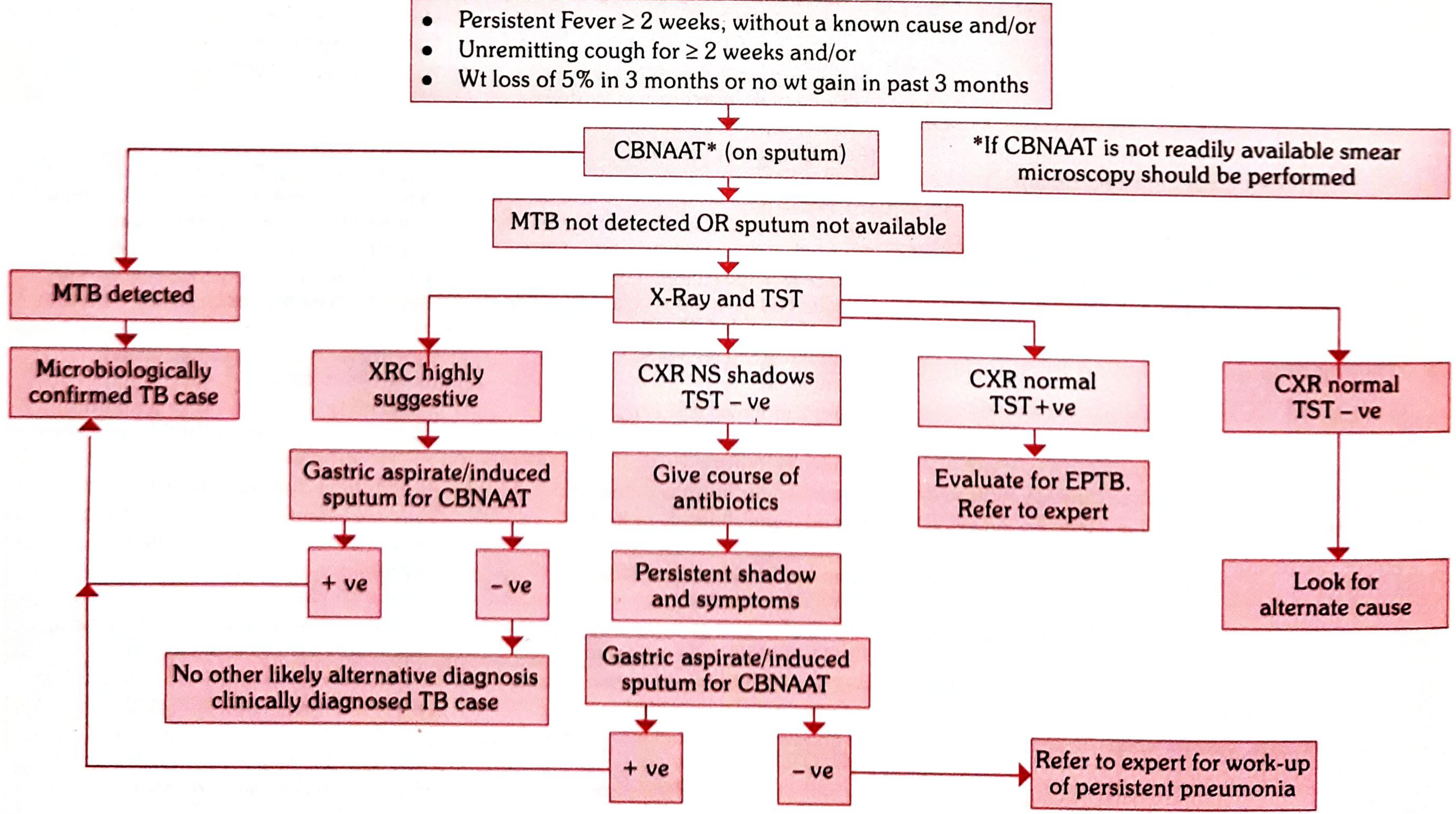
Diagnostic Algorithm (RNTCP/NTEP - India):
TST Interpretation (AAP criteria - Harriet Lane):
| Induration | Positive if... |
|---|---|
| ≥5 mm | Close TB contact; suspected active TB; immunosuppressed / HIV-positive |
| ≥10 mm | Age <4 yrs; underlying conditions (cancer, DM, renal failure, malnutrition); endemic country travel/birth |
| ≥15 mm | Children ≥4 years with no risk factors |
- IGRAs (QuantiFERON-TB Gold, T-SPOT-TB) offer high specificity and can be used in children ≥2 years old. Preferred in BCG-vaccinated children.
Additional Investigations:
- CT chest is preferred over CXR when available for active disease workup
- Lumbar puncture: mandatory in children <12 months with confirmed TB; consider in older children with neurological signs
- All confirmed TB cases should be offered HIV testing
Important: Do NOT use fluoroquinolones, linezolid, or amoxicillin-clavulanate as empiric antibiotics for suspected TB - these have anti-TB activity and can confound diagnosis.
Treatment
Drug-Sensitive TB (Standard Regimens)
- 2 months of HRZE (Isoniazid + Rifampicin + Pyrazinamide + Ethambutol) intensive phase
- 4 months of HR (Isoniazid + Rifampicin) continuation phase
| Drug | Paediatric Dose |
|---|---|
| Isoniazid (H) | 7-15 mg/kg/day (max 300 mg) |
| Rifampicin (R) | 10-20 mg/kg/day (max 600 mg) |
| Pyrazinamide (Z) | 30-40 mg/kg/day (max 2000 mg) |
| Ethambutol (E) | 15-25 mg/kg once daily |
Latent TB Infection (LTBI) Treatment
| Regimen | Duration | Notes |
|---|---|---|
| Rifampin alone | 4 months | Preferred, especially for children ≤5 years |
| Isoniazid + Rifapentine (weekly) | 12 weeks | Preferred if ≥2 years old |
| Isoniazid alone | 9 months | Alternative |
| Isoniazid + Rifampin | 3 months | Alternative |
TB Preventive Therapy (Chemoprophylaxis)
- Asymptomatic contacts aged <6 years of a smear-positive case (after ruling out active disease)
- HIV-infected children with known TB exposure or TST positive (≥5 mm)
- TST-positive children on immunosuppressive therapy (nephrotic syndrome, leukaemia, etc.)
- Neonates born to mothers with TB during pregnancy (after ruling out congenital TB), followed by BCG vaccination
Drug-Resistant TB in Children
- Always treat in consultation with an expert
- Include at least 4-6 bactericidal drugs to which the strain is known/likely susceptible
- Do not add a single drug to a failing regimen
- Treat for at least 12 months after culture conversion to negative; extend to 24 months for HIV or cavitatory lesions
| Drug | Dose |
|---|---|
| Levofloxacin (≤5 yrs) | 15-20 mg/kg in 2 divided doses |
| Levofloxacin (>5 yrs) | 10-15 mg/kg once daily |
| Moxifloxacin | 7.5-10 mg/kg |
| Linezolid | 10 mg/kg 3x daily (+ pyridoxine) |
| Meropenem | 20-40 mg/kg IV every 8 hours |
| Cycloserine | 10-20 mg/kg |
BCG Vaccination
TB in HIV-Infected Children
- TB-HIV co-infection dramatically increases risk of dissemination and death
- Both conditions must be treated simultaneously (with attention to drug interactions, especially rifampicin and antiretrovirals)
- TST threshold is reduced to ≥5 mm in HIV-positive children
- All diagnosed TB cases should be tested for HIV
Recent Evidence (PubMed, 2023-2026)
Create a clinical summary document on paediatric TB screening and treatment
mkdir -p /home/daytona/workspace/paediatric-tb && ls /home/daytona/workspace/pae…
~/paediatric-tb/generate.js
const {
Document, Packer, Paragraph, TextRun, Table, TableRow, TableCell,
HeadingLevel, AlignmentType, BorderStyle, WidthType, ShadingType,
VerticalAlign, PageNumber, Header, Footer, TabStopType, TabStopPosition,
PageBreak
} = require('docx');
const fs = require('fs');
// ── Colour palette ──────────────────────────────────────────────────────────
const NAVY = "1F3864"; // deep navy – headings
const TEAL = "0D6B6E"; // teal – section bars
const LTBLUE = "D9E8F5"; // light blue – table header shading
const LTGREY = "F2F2F2"; // light grey – alternate table rows
const WHITE = "FFFFFF";
const BLACK = "000000";
const RED = "C0392B"; // warning text
const ORANGE = "D35400"; // highlight
// ── Helper: Coloured section heading bar ────────────────────────────────────
function sectionHeading(text) {
return new Paragraph({
spacing: { before: 280, after: 100 },
shading: { type: ShadingType.SOLID, color: TEAL, fill: TEAL },
indent: { left: 0 },
children: [
new TextRun({
text: text.toUpperCase(),
bold: true,
color: WHITE,
size: 22,
font: "Calibri"
})
]
});
}
// ── Helper: Sub-heading ──────────────────────────────────────────────────────
function subHeading(text) {
return new Paragraph({
spacing: { before: 180, after: 60 },
children: [
new TextRun({
text,
bold: true,
color: NAVY,
size: 21,
font: "Calibri"
})
]
});
}
// ── Helper: Body paragraph ───────────────────────────────────────────────────
function body(text, { bold = false, italic = false, color = BLACK, indent = 0 } = {}) {
return new Paragraph({
spacing: { after: 80 },
indent: { left: indent },
children: [
new TextRun({ text, bold, italic, color, size: 20, font: "Calibri" })
]
});
}
// ── Helper: Bullet ───────────────────────────────────────────────────────────
function bullet(text, level = 0) {
return new Paragraph({
bullet: { level },
spacing: { after: 60 },
indent: { left: 360 + level * 360 },
children: [
new TextRun({ text, size: 20, font: "Calibri", color: BLACK })
]
});
}
// ── Helper: Warning box ──────────────────────────────────────────────────────
function warningBox(text) {
return new Paragraph({
spacing: { before: 140, after: 140 },
shading: { type: ShadingType.SOLID, color: "FFF3CD", fill: "FFF3CD" },
border: {
left: { style: BorderStyle.SINGLE, size: 18, color: ORANGE }
},
indent: { left: 200 },
children: [
new TextRun({ text: "⚠ " + text, size: 20, font: "Calibri", color: ORANGE, bold: true })
]
});
}
// ── Helper: simple table ─────────────────────────────────────────────────────
function makeTable(headers, rows, colWidths) {
const headerRow = new TableRow({
tableHeader: true,
children: headers.map((h, i) =>
new TableCell({
width: { size: colWidths[i], type: WidthType.DXA },
shading: { type: ShadingType.SOLID, color: NAVY, fill: NAVY },
verticalAlign: VerticalAlign.CENTER,
children: [new Paragraph({
alignment: AlignmentType.CENTER,
children: [new TextRun({ text: h, bold: true, color: WHITE, size: 19, font: "Calibri" })]
})]
})
)
});
const dataRows = rows.map((row, ri) =>
new TableRow({
children: row.map((cell, ci) =>
new TableCell({
width: { size: colWidths[ci], type: WidthType.DXA },
shading: { type: ShadingType.SOLID, color: ri % 2 === 0 ? WHITE : LTGREY, fill: ri % 2 === 0 ? WHITE : LTGREY },
verticalAlign: VerticalAlign.CENTER,
children: [new Paragraph({
children: [new TextRun({ text: String(cell), size: 19, font: "Calibri", color: BLACK })]
})]
})
)
})
);
return new Table({
width: { size: 9026, type: WidthType.DXA },
rows: [headerRow, ...dataRows]
});
}
// ── Helper: spacer ───────────────────────────────────────────────────────────
function spacer(size = 100) {
return new Paragraph({ spacing: { after: size }, children: [] });
}
// ═══════════════════════════════════════════════════════════════════════════
// DOCUMENT CONTENT
// ═══════════════════════════════════════════════════════════════════════════
const children = [
// ── TITLE BLOCK ────────────────────────────────────────────────────────
new Paragraph({
spacing: { before: 0, after: 80 },
shading: { type: ShadingType.SOLID, color: NAVY, fill: NAVY },
alignment: AlignmentType.CENTER,
children: [
new TextRun({ text: "PAEDIATRIC TUBERCULOSIS", bold: true, color: WHITE, size: 36, font: "Calibri" })
]
}),
new Paragraph({
spacing: { after: 60 },
shading: { type: ShadingType.SOLID, color: TEAL, fill: TEAL },
alignment: AlignmentType.CENTER,
children: [
new TextRun({ text: "Clinical Summary: Screening, Diagnosis & Treatment", color: WHITE, size: 22, font: "Calibri", italic: true })
]
}),
new Paragraph({
spacing: { after: 20 },
shading: { type: ShadingType.SOLID, color: LTBLUE, fill: LTBLUE },
alignment: AlignmentType.CENTER,
children: [
new TextRun({ text: "Sources: Park's Textbook of Preventive & Social Medicine | Harriet Lane Handbook 23rd Ed. (Johns Hopkins) | WHO / NTEP / AAP Guidelines", color: NAVY, size: 17, font: "Calibri" })
]
}),
spacer(200),
// ══════════════════════════════════════════════════════════════════════
// 1. EPIDEMIOLOGY
// ══════════════════════════════════════════════════════════════════════
sectionHeading("1. Epidemiology & Risk Factors"),
subHeading("Burden"),
bullet("Children <15 years = 6–8% of all TB cases globally"),
bullet("Most common age group: 1–4 years"),
bullet("Children are rarely sputum smear-positive; they are not significant sources of transmission"),
bullet("Childhood TB largely reflects failure of adult TB control in the community"),
spacer(80),
subHeading("Risk Factors for Infection & Progression"),
makeTable(
["Risk Category", "Specific Risk Factors"],
[
["Age", "< 5 years: up to 20% progress to disease within 2 years of infection"],
["Exposure", "Household contact with smear-positive PTB; infant of TB-positive mother"],
["Immunity", "HIV infection, malnutrition, immunosuppressive therapy (steroids, TNF-blockers)"],
["Comorbidities", "Cancer, diabetes mellitus, chronic renal failure, nephrotic syndrome"],
["Geography", "Born in / travelled to TB-endemic country"],
["Dissemination", "Young age is the principal risk factor for miliary TB and TB meningitis"]
],
[2500, 6526]
),
spacer(200),
// ══════════════════════════════════════════════════════════════════════
// 2. CLINICAL FEATURES
// ══════════════════════════════════════════════════════════════════════
sectionHeading("2. Clinical Features"),
subHeading("Cardinal Symptoms (Presumptive TB – NTEP Criteria)"),
bullet("Persistent fever ≥ 2 weeks without a known cause"),
bullet("Unremitting cough ≥ 2 weeks"),
bullet("Weight loss ≥ 5% in 3 months OR no weight gain in the past 3 months"),
spacer(80),
subHeading("Pulmonary TB"),
bullet("Hilar / mediastinal lymphadenopathy (most common CXR finding)"),
bullet("Consolidation, miliary pattern, chronic fibrocavitatory shadows"),
bullet("Children rarely produce sputum – gastric aspirate is often required"),
spacer(80),
subHeading("Extrapulmonary TB (EPTB) – more common in children than adults"),
makeTable(
["Site", "Features"],
[
["Peripheral lymphadenitis", "Most common EPTB; cervical nodes most frequent; may suppurate"],
["TB meningitis", "Severe headache, vomiting, altered sensorium, neck stiffness; high mortality"],
["Miliary TB", "Diffuse miliary nodules on CXR; fever, hepatosplenomegaly"],
["Pleural TB", "Exudative pleural effusion; TST usually positive"],
["Abdominal TB", "Ascites, lymphadenopathy, obstruction"],
["Osteoarticular TB", "Pott's disease (spine), joint swelling, limp"]
],
[2800, 6226]
),
spacer(200),
// ══════════════════════════════════════════════════════════════════════
// 3. SCREENING
// ══════════════════════════════════════════════════════════════════════
sectionHeading("3. Screening"),
subHeading("AAP / Harriet Lane Screening Approach"),
body("Complete at-risk assessment at: first well-child visit → every 6 months in year 1 → then annually."),
spacer(60),
subHeading("Screen if Any of the Following Apply"),
bullet("Born outside US / travelled to TB-endemic country"),
bullet("Family member with positive TST or known TB exposure"),
bullet("Exposed to person with active TB disease"),
bullet("On immunosuppressive therapy (e.g. TNF-blockers, steroids)"),
bullet("Household contact with a person who: was incarcerated, uses illegal drugs, is HIV-positive"),
bullet("Consumes unpasteurised milk or milk products"),
spacer(200),
// ══════════════════════════════════════════════════════════════════════
// 4. DIAGNOSTIC TESTS
// ══════════════════════════════════════════════════════════════════════
sectionHeading("4. Diagnostic Tests"),
subHeading("4a. Tuberculin Skin Test (TST / Mantoux)"),
body("India: 2 TU PPD RT23 intradermally; read at 48–72 h. USA (AAP): standard PPD 5 TU."),
spacer(60),
body("Threshold for a POSITIVE result (Harriet Lane / AAP criteria):", { bold: true }),
spacer(40),
makeTable(
["Induration", "Population"],
[
["≥ 5 mm", "Close TB contact; suspected active TB; immunosuppressed / HIV-positive"],
["≥ 10 mm", "Age < 4 yrs; cancer, DM, CRF, malnutrition; born in / travelled to endemic country; contact with high-risk adults"],
["≥ 15 mm", "Children ≥ 4 years with NO risk factors"]
],
[1400, 7626]
),
spacer(120),
subHeading("4b. Interferon Gamma Release Assays (IGRAs)"),
bullet("QuantiFERON-TB Gold In-Tube and T-SPOT.TB"),
bullet("High specificity; not affected by prior BCG vaccination"),
bullet("Can be used in children ≥ 2 years old"),
bullet("Preferred over TST in BCG-vaccinated children in low-incidence settings"),
spacer(80),
subHeading("4c. Microbiological Tests"),
makeTable(
["Test", "Specimen", "Key Points"],
[
["CBNAAT (GeneXpert)", "Sputum / GA / IS / BAL", "PREFERRED first-line; detects rifampicin resistance; result in ~2 hrs"],
["Smear microscopy (ZN / fluorescent)", "Sputum (≥2 samples)", "Use if CBNAAT unavailable; low sensitivity in children"],
["Liquid culture (MGIT)", "Any specimen", "Gold standard; result in 1–6 weeks"],
["Solid culture (LJ medium)", "Any specimen", "Up to 10 weeks; DST available"],
["Nucleic acid amplification", "Various", "Rapid; may also detect rifampicin resistance"]
],
[2200, 2800, 4026]
),
spacer(80),
body("Specimen sources: sputum, gastric aspirate (morning x3), induced sputum, BAL, pleural fluid, CSF, urine, tissue biopsy."),
spacer(80),
subHeading("4d. Radiology"),
bullet("Chest X-ray: FIRST imaging step after positive screening test"),
bullet("Highly suggestive CXR findings: hilar/mediastinal lymphadenopathy, miliary pattern, fibrocavitatory shadows"),
bullet("CT chest: preferred over CXR when active disease is suspected (Harriet Lane)"),
bullet("Non-specific CXR: consolidations, bronchopneumonia patterns – may require further workup"),
spacer(80),
subHeading("4e. CSF / Lumbar Puncture"),
bullet("Mandatory in all children < 12 months with confirmed TB"),
bullet("Consider in children > 12 months with neurological signs/symptoms"),
spacer(80),
warningBox("Do NOT use fluoroquinolones, linezolid, or amoxicillin-clavulanate as empiric antibiotics – they have anti-TB activity and will confound diagnosis and DST results."),
spacer(200),
// ══════════════════════════════════════════════════════════════════════
// 5. DIAGNOSTIC ALGORITHM SUMMARY
// ══════════════════════════════════════════════════════════════════════
sectionHeading("5. Diagnostic Algorithm (NTEP / RNTCP – Pulmonary TB)"),
makeTable(
["Step", "Action"],
[
["Presumptive TB", "Fever ≥2 wks AND/OR cough ≥2 wks AND/OR weight loss ≥5% in 3 months"],
["Step 1", "CBNAAT on sputum → MTB detected = Microbiologically confirmed TB → start treatment"],
["Step 2 (if CBNAAT –ve or no specimen)", "Chest X-ray + TST (Mantoux 2 TU PPD RT23)"],
["CXR highly suggestive", "Gastric aspirate / induced sputum for CBNAAT → +ve = confirmed; –ve = clinically diagnosed TB"],
["CXR NS shadows + TST –ve", "Trial of non-TB antibiotics → if shadows persist → gastric aspirate/IS for CBNAAT"],
["CXR normal + TST +ve", "Evaluate for EPTB; refer to specialist"],
["CXR normal + TST –ve", "Look for alternative diagnosis"],
["Rif-resistance on CBNAAT", "Manage as DR-TB; refer to DR-TB centre"]
],
[2000, 7026]
),
spacer(80),
body("Note: This algorithm applies only to drug-sensitive TB suspects (no prior ATT, not MDR/RR-TB contacts).", { italic: true, color: "666666" }),
spacer(80),
warningBox("All confirmed TB cases must be offered HIV testing."),
spacer(200),
// ══════════════════════════════════════════════════════════════════════
// 6. TREATMENT – DRUG-SENSITIVE TB
// ══════════════════════════════════════════════════════════════════════
sectionHeading("6. Treatment – Drug-Sensitive TB"),
subHeading("Standard Regimen"),
makeTable(
["Phase", "Duration", "Drugs", "Notes"],
[
["Intensive", "2 months", "Isoniazid + Rifampicin + Pyrazinamide + Ethambutol (HRZE)", "Daily under DOT"],
["Continuation", "4 months", "Isoniazid + Rifampicin (HR)", "Daily under DOT"],
["Total", "6 months", "—", "India: paediatric patient-wise fixed-dose boxes by weight band"]
],
[1500, 1300, 3800, 2426]
),
spacer(120),
subHeading("WHO Recommended Paediatric Drug Doses (< 30 kg)"),
makeTable(
["Drug", "Daily Dose", "Max Dose"],
[
["Isoniazid (H)", "7–15 mg/kg", "300 mg"],
["Rifampicin (R)", "10–20 mg/kg", "600 mg"],
["Pyrazinamide (Z)", "30–40 mg/kg", "2000 mg"],
["Ethambutol (E)", "15–25 mg/kg once daily", "—"]
],
[2800, 3000, 3226]
),
spacer(200),
// ══════════════════════════════════════════════════════════════════════
// 7. TREATMENT – LATENT TB INFECTION (LTBI)
// ══════════════════════════════════════════════════════════════════════
sectionHeading("7. Treatment – Latent TB Infection (LTBI)"),
body("Step 1: Always rule out active TB before starting LTBI treatment."),
spacer(80),
subHeading("AAP / Harriet Lane Recommended Regimens"),
makeTable(
["Regimen", "Duration", "Preferred?"],
[
["Rifampin (R) alone", "4 months daily", "Preferred, especially ≤ 5 years"],
["Isoniazid + Rifapentine (3HP) – weekly", "12 weeks", "Preferred if ≥ 2 years of age"],
["Isoniazid (H) alone", "9 months daily", "Alternative"],
["Isoniazid + Rifampin (HR)", "3 months daily", "Alternative"]
],
[2800, 2400, 3826]
),
spacer(120),
subHeading("NTEP / India: TB Preventive Therapy (TPT) Indications"),
body("INH dose: 10 mg/kg/day for 6 months. Indicated for:"),
bullet("Asymptomatic contacts < 6 years of a smear-positive PTB case (after ruling out active disease, regardless of BCG/nutritional status)"),
bullet("HIV-infected children with known TB exposure OR TST positive (≥ 5 mm) without active TB"),
bullet("TST-positive children on immunosuppressive therapy (e.g., nephrotic syndrome, acute leukaemia)"),
bullet("Neonate born to a mother diagnosed with TB in pregnancy (after ruling out congenital TB) – followed by BCG vaccination after 6 months"),
spacer(200),
// ══════════════════════════════════════════════════════════════════════
// 8. TREATMENT – DRUG-RESISTANT TB
// ══════════════════════════════════════════════════════════════════════
sectionHeading("8. Treatment – Drug-Resistant TB (DR-TB)"),
subHeading("Principles"),
bullet("Always treat in consultation with a DR-TB specialist"),
bullet("Include at least 4–6 bactericidal drugs to which the strain is known/likely susceptible"),
bullet("Never add a single drug to a failing regimen"),
bullet("Treat for ≥ 12 months after culture conversion to negative"),
bullet("Extend to 24 months for HIV co-infection or cavitatory lesions"),
spacer(80),
subHeading("Selected WHO Paediatric DR-TB Drug Doses"),
makeTable(
["Drug", "Paediatric Dose"],
[
["Levofloxacin (≤ 5 yrs)", "15–20 mg/kg/day in 2 divided doses"],
["Levofloxacin (> 5 yrs)", "10–15 mg/kg once daily"],
["Moxifloxacin", "7.5–10 mg/kg once daily"],
["Linezolid", "10 mg/kg 3× daily (+ pyridoxine B6)"],
["Cycloserine", "10–20 mg/kg/day"],
["Ethionamide / Protionamide", "15–20 mg/kg/day"],
["Meropenem (IV)", "20–40 mg/kg every 8 hours"],
["p-Aminosalicylic acid", "200–300 mg/kg/day (< 30 kg)"],
["Amikacin / Kanamycin / Capreomycin", "15–30 mg/kg once daily (max 1000 mg)"]
],
[3500, 5526]
),
spacer(200),
// ══════════════════════════════════════════════════════════════════════
// 9. TB-HIV CO-INFECTION
// ══════════════════════════════════════════════════════════════════════
sectionHeading("9. TB-HIV Co-Infection in Children"),
bullet("HIV dramatically increases risk of TB infection progressing to disseminated disease and death"),
bullet("TST threshold is reduced to ≥ 5 mm in HIV-positive children"),
bullet("Both TB and HIV must be treated simultaneously; monitor for drug interactions (rifampicin strongly induces CYP450 – affects ART levels)"),
bullet("TPT with INH 10 mg/kg/day for 6 months is indicated for all HIV-positive children with TB exposure or positive TST without active disease"),
bullet("All TB-diagnosed children must be tested for HIV"),
spacer(200),
// ══════════════════════════════════════════════════════════════════════
// 10. BCG VACCINATION
// ══════════════════════════════════════════════════════════════════════
sectionHeading("10. BCG Vaccination"),
bullet("BCG given at birth provides strong protection against severe childhood TB: TB meningitis and miliary TB"),
bullet("Does not reliably prevent pulmonary TB in adults"),
bullet("After LTBI prophylaxis in a neonate of a TB-positive mother: give 6 months INH → then BCG vaccination"),
bullet("BCG scar failure does not require re-vaccination if the child is in a high-burden country (vaccination was effective)"),
spacer(200),
// ══════════════════════════════════════════════════════════════════════
// 11. MONITORING & FOLLOW-UP
// ══════════════════════════════════════════════════════════════════════
sectionHeading("11. Monitoring During Treatment"),
makeTable(
["Parameter", "Frequency / Notes"],
[
["Weight & clinical response", "Every 2–4 weeks; dose-adjust at each weight band threshold"],
["Sputum smear / culture", "End of intensive phase (month 2), month 5, end of treatment"],
["Chest X-ray", "End of treatment; or if clinical deterioration"],
["Liver function (if symptomatic)", "Isoniazid, rifampicin, pyrazinamide are hepatotoxic – monitor if symptomatic"],
["Pyridoxine (B6) supplementation", "Give with INH if malnourished, HIV-positive, or breastfeeding"],
["DOT compliance", "Every dose under direct observation until treatment completion"]
],
[3000, 6026]
),
spacer(200),
// ══════════════════════════════════════════════════════════════════════
// 12. KEY REFERENCES
// ══════════════════════════════════════════════════════════════════════
sectionHeading("12. References & Sources"),
bullet("Park's Textbook of Preventive and Social Medicine – RNTCP / NTEP Paediatric TB Guidelines, pp. 218–230"),
bullet("The Harriet Lane Handbook, 23rd Edition – The Johns Hopkins Hospital, pp. 620–621 (AAP / WHO Recommendations)"),
bullet("WHO Guidelines for Treatment of Drug-Susceptible Tuberculosis, 2022 Update"),
bullet("Martinez L et al. Effectiveness of preventive treatment across age groups. Lancet Respir Med. 2024 Aug. [PMID: 38734022]"),
bullet("Duong T et al. Levofloxacin for contacts of MDR-TB. NEJM Evid. 2025 Jan. [PMID: 39693627]"),
spacer(100),
new Paragraph({
spacing: { before: 200 },
alignment: AlignmentType.CENTER,
children: [
new TextRun({ text: "Clinical Summary Document | Prepared by Orris | July 2026", size: 17, font: "Calibri", color: "888888", italic: true })
]
})
];
// ── Build & write document ──────────────────────────────────────────────────
const doc = new Document({
creator: "Orris Clinical AI",
title: "Paediatric Tuberculosis – Clinical Summary",
description: "Clinical summary covering screening, diagnosis and treatment of paediatric TB",
styles: {
default: {
document: {
run: { font: "Calibri", size: 20 }
}
}
},
sections: [{
properties: {
page: {
margin: { top: 720, bottom: 720, left: 900, right: 900 }
}
},
headers: {
default: new Header({
children: [
new Paragraph({
shading: { type: ShadingType.SOLID, color: NAVY, fill: NAVY },
children: [
new TextRun({ text: "PAEDIATRIC TUBERCULOSIS – Clinical Summary", bold: true, color: WHITE, size: 18, font: "Calibri" }),
new TextRun({ text: " | Orris Clinical AI | July 2026", color: "AAAAAA", size: 17, font: "Calibri" })
]
})
]
})
},
footers: {
default: new Footer({
children: [
new Paragraph({
alignment: AlignmentType.CENTER,
children: [
new TextRun({ text: "Page ", size: 17, font: "Calibri", color: "888888" }),
new PageNumber()
]
})
]
})
},
children
}]
});
Packer.toBuffer(doc).then(buffer => {
fs.writeFileSync("/home/daytona/workspace/paediatric-tb/Paediatric_TB_Clinical_Summary.docx", buffer);
console.log("✓ Document written successfully.");
}).catch(err => {
console.error("Error:", err);
process.exit(1);
});
cd /home/daytona/workspace/paediatric-tb && node generate.js
cd /home/daytona/workspace/paediatric-tb && node -e "const d = require('docx'); …
cd /home/daytona/workspace/paediatric-tb && node -e "const {PageNumber, PageNumb…
~/paediatric-tb/generate.js
Error: String not found in file: ' PageNumber, PageBreak
} = require('docx');'~/paediatric-tb/generate.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/paediatric-tb/generate.js'
~/paediatric-tb/generate.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/paediatric-tb/generate.js'
cd /home/daytona/workspace/paediatric-tb && node generate.js
python /home/daytona/skills/docx/scripts/office/validate.py /home/daytona/worksp…
python3 -c " import zipfile, os path = '/home/daytona/workspace/paediatric-tb/Pa…
Paediatric TB Clinical Summary
Word Document · DOCX
- Epidemiology & Risk Factors - burden, age distribution, risk factor table
- Clinical Features - presumptive TB criteria, pulmonary + EPTB table
- Screening - AAP/Harriet Lane at-risk questionnaire approach
- Diagnostic Tests - TST interpretation table, IGRAs, CBNAAT/culture/smear table, radiology, LP indications
- Diagnostic Algorithm - NTEP step-by-step flowchart summary table
- Treatment - Drug-Sensitive TB - standard 2HRZE/4HR regimen + WHO paediatric dose table
- Treatment - LTBI - AAP regimen table + NTEP TPT indications
- Treatment - Drug-Resistant TB - principles + full DR-TB drug dose table
- TB-HIV Co-infection - key management points
- BCG Vaccination - role and limitations
- Monitoring During Treatment - parameter/frequency table
- References - Park's, Harriet Lane, WHO, and 2024-2025 PubMed citations