Hemoglobin degradation & Jaundice biochemistry
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the complete answer:
Hemoglobin Degradation & Jaundice Biochemistry
1. Overview of Heme Degradation
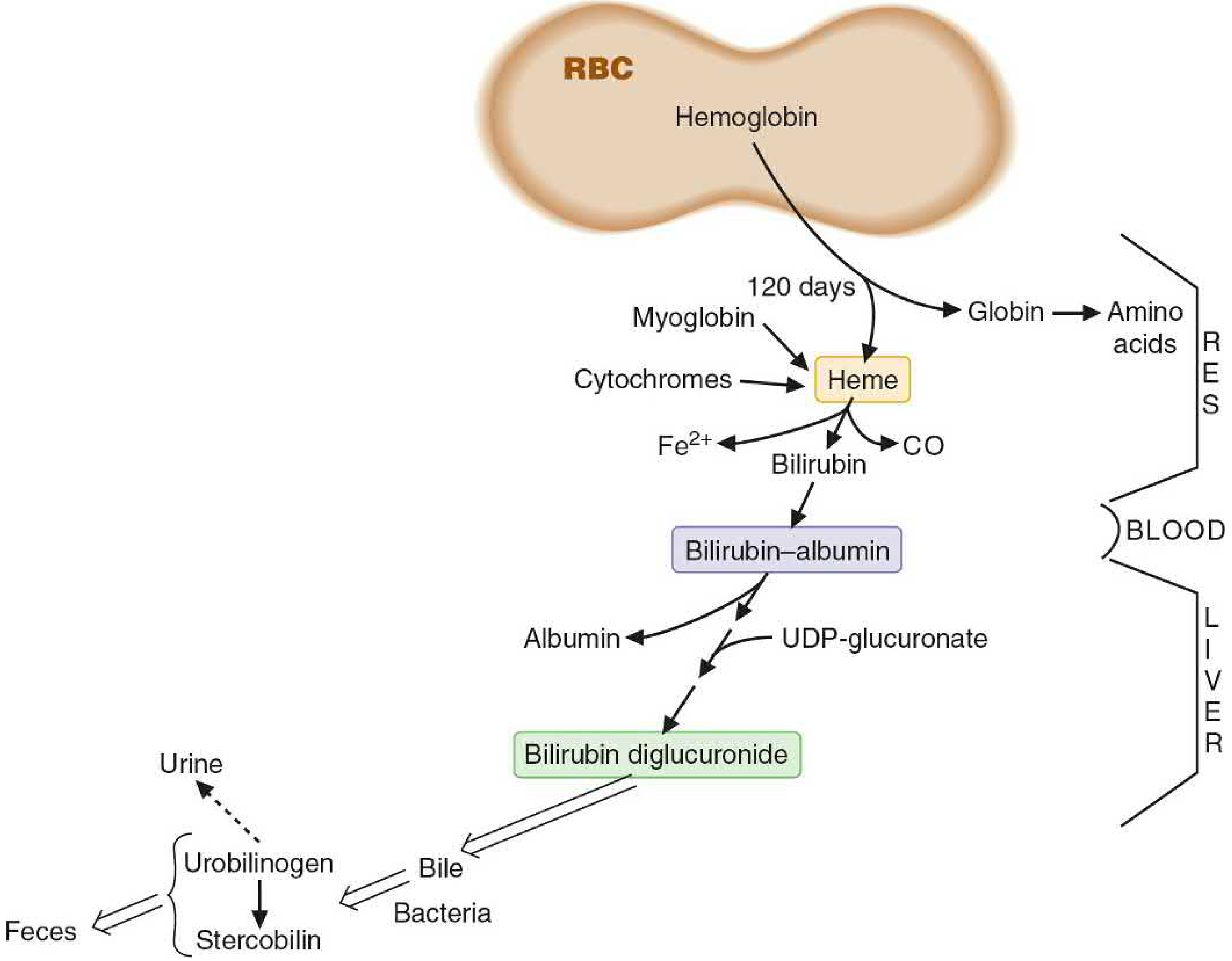
Overview of heme degradation — Basic Medical Biochemistry: A Clinical Approach, 6e
2. Step-by-Step Heme Catabolism
Step 1 — RBC Senescence & Phagocytosis
Red blood cells survive ~120 days. Senescent RBCs are phagocytosed by macrophages of the reticuloendothelial system (RES) — primarily in the spleen, liver (Kupffer cells), and bone marrow.
- 70–90% of bilirubin derives from hemoglobin of aging RBCs
- The remaining ~10–30% comes from myoglobin, cytochromes P450, and other heme-containing proteins (ineffective erythropoiesis also contributes)
Step 2 — Globin & Iron Separation
Within the macrophage:
- Globin chains are proteolyzed → free amino acids (recycled)
- Iron (Fe²⁺) is released and returned to the body's iron stores (ferritin / transferrin)
Step 3 — Heme → Biliverdin → Bilirubin
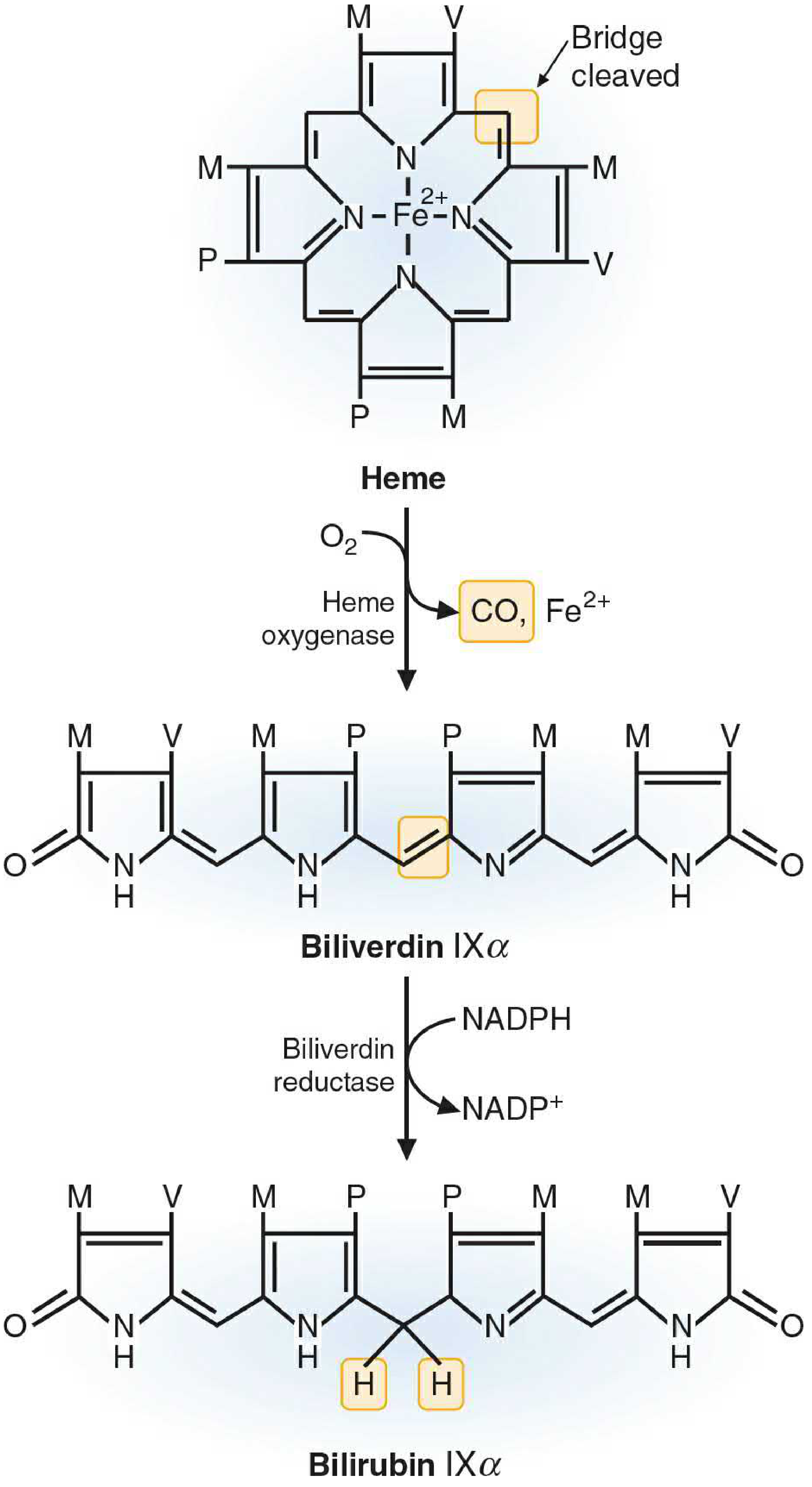
Conversion of heme to bilirubin — Basic Medical Biochemistry: A Clinical Approach, 6e
| Reaction | Enzyme | Co-factors | Product |
|---|---|---|---|
| Heme → Biliverdin IXα | Heme oxygenase | O₂, NADPH | Biliverdin + CO + Fe²⁺ |
| Biliverdin → Bilirubin IXα | Biliverdin reductase | NADPH → NADP⁺ | Bilirubin (unconjugated) |
- A methylene bridge in the porphyrin ring is oxidatively cleaved, releasing carbon monoxide (CO) — a clinically measurable marker of hemolysis
- Bilirubin IXα is the predominant isomer produced in humans
Step 4 — Transport in Blood (Unconjugated Bilirubin)
- Bilirubin is water-insoluble (lipophilic) due to extensive internal hydrogen bonding
- Transported in plasma tightly bound to albumin (non-covalently)
- Cannot be filtered at the glomerulus in this form → absent from normal urine
- Van den Bergh test: indirect-reacting (requires methanol to disrupt H-bonds before diazo reaction)
3. Hepatic Processing
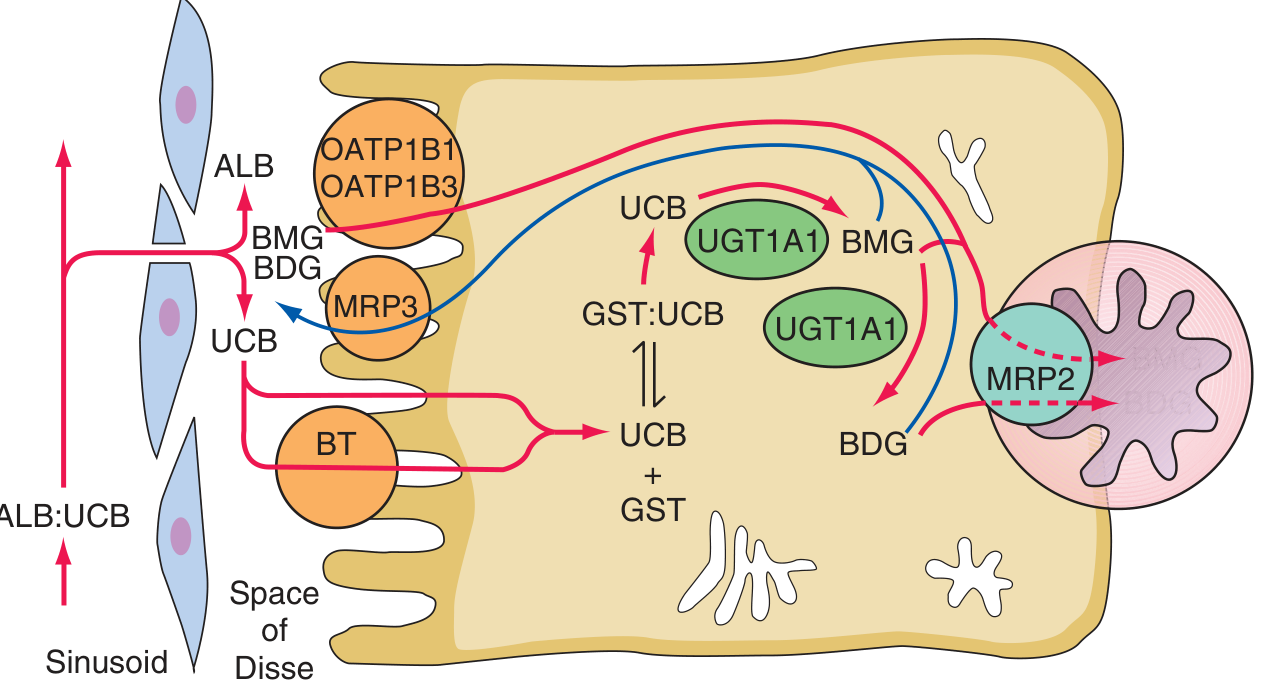
Hepatocellular bilirubin transport — Harrison's Principles of Internal Medicine 22E
Four steps at the hepatocyte level:
| Step | Process | Key Molecules |
|---|---|---|
| 1 | Uptake | Carrier-mediated (OATP1B1, OATP1B3, proposed BT transporter) |
| 2 | Intracellular binding | Glutathione-S-transferases (ligandins) keep bilirubin in solution |
| 3 | Conjugation | UGT1A1 (bilirubin-UDP-glucuronosyltransferase) adds 1–2 glucuronic acid moieties using UDP-glucuronate → bilirubin mono- and diglucuronide |
| 4 | Biliary excretion | MRP2 (ABCC2) transports conjugated bilirubin across the canalicular membrane into bile |
Conjugation disrupts internal H-bonds → bilirubin becomes water-soluble → directly reactive on Van den Bergh (direct bilirubin). Conjugation is obligatory for biliary excretion.
A fraction of conjugated bilirubin is returned to portal circulation by MRP3 (sinusoidal efflux) → reuptake via OATP1B1/OATP1B3 (important in Rotor syndrome pathogenesis).
4. Intestinal Fate & Enterohepatic Circulation
- Bilirubin diglucuronide passes through the gut without mucosal reabsorption
- Intestinal bacteria deconjugate and reduce bilirubin → urobilinogen (colorless)
- Urobilinogen fate:
- Most → oxidized to stercobilin → excreted in feces (gives stool its brown color)
- ~20% reabsorbed (enterohepatic circulation) → re-excreted by liver
- Small amount enters systemic circulation → filtered by kidneys → urobilin in urine (normal trace amounts)
Clinical note: Conjugated bilirubin can appear in urine (bilirubinuria) because it is small enough for glomerular filtration — unlike unconjugated bilirubin.
5. Jaundice — Definition & Threshold
Jaundice = yellowish staining of skin, sclera, and mucous membranes by bilirubin. Clinically detectable when serum bilirubin rises above 2.5–3 mg/dL (normal < 1.0 mg/dL total). — Schwartz's Principles of Surgery, 11e
6. Classification of Jaundice (Prehepatic / Intrahepatic / Posthepatic)
A. Prehepatic (Hemolytic) Jaundice
Mechanism: Excess heme production overwhelms hepatic conjugation capacity
- Bilirubin type: Unconjugated (indirect) hyperbilirubinemia
- Hemolysis alone rarely causes serum bilirubin > 4 mg/dL (bone marrow can sustain only ~8× increase in RBC production; higher levels imply hepatic dysfunction)
- No bilirubinuria (UCB too tightly albumin-bound)
- Urine urobilinogen: ↑↑ (more bilirubin delivered to gut → more urobilinogen formed)
- Stool color: dark (stercobilin ↑)
Causes:
- Hereditary: Sickle cell disease, hereditary spherocytosis, G6PD deficiency, thalassemia
- Acquired immune: Autoimmune hemolytic anemia (Coombs +)
- Acquired non-immune: Drug-induced RBC damage, mechanical hemolysis (prosthetic heart valves), microangiopathic hemolytic anemia, infections (malaria)
- Ineffective erythropoiesis: Thalassemia major, megaloblastic anemia, porphyria
B. Intrahepatic Jaundice
Mechanism: Failure of conjugation or intracellular transport within hepatocytes
Unconjugated type (conjugation defect):
| Disorder | Defect | Severity |
|---|---|---|
| Physiologic jaundice of newborn | Immature UGT1A1 (adult levels at 3–4 months) | Mild, resolves spontaneously |
| Breast milk jaundice | Bilirubin-deconjugating enzymes in breast milk | Mild |
| Gilbert syndrome | ↓ UGT1A1 activity (~30% of normal); promoter region mutation (TATAA box) | Benign; bilirubin rises with fasting/stress; 4–7% of population |
| Crigler-Najjar type I | Complete absence of UGT1A1 | Fatal without liver transplant; kernicterus |
| Crigler-Najjar type II (Arias) | Residual UGT1A1 activity | Responsive to phenobarbital |
Conjugated type (secretion/excretion defect):
| Disorder | Defect | Feature |
|---|---|---|
| Dubin-Johnson syndrome | MRP2 mutation → impaired canalicular export | Black liver (melanin-like pigment deposition); AR; benign |
| Rotor syndrome | OATP1B1 + OATP1B3 deficiency → impaired hepatic reuptake of conjugated bilirubin | AR; benign; no liver pigment |
Acquired intrahepatic causes:
- Viral hepatitis, alcoholic hepatitis, cirrhosis
- Drugs (acetaminophen toxicity, OCP, anabolic steroids)
- Sepsis, ischemia/hypoxia
- Autoimmune hepatitis, primary biliary cholangitis, primary sclerosing cholangitis
C. Posthepatic (Obstructive) Jaundice
Mechanism: Obstruction of bile flow at or below the bile ducts
- Bilirubin type: Conjugated (direct) hyperbilirubinemia
- Bilirubinuria: present (dark urine — "Coca-Cola" urine)
- Urine urobilinogen: ↓ or absent (no bilirubin reaching gut)
- Stool color: pale/clay-colored (no stercobilin)
- Alkaline phosphatase + GGT: markedly elevated (cholestatic pattern)
Intrinsic causes: Cholelithiasis (gallstones), choledocholithiasis, cholangiocarcinoma, primary sclerosing cholangitis, benign biliary stricture, disorders of the ampulla of Vater
Extrinsic causes: Carcinoma of the head of the pancreas (classic), chronic pancreatitis, pancreatic pseudocyst
7. Differential Diagnosis Summary Table
| Feature | Prehepatic | Intrahepatic (Unconj.) | Intrahepatic (Conj.) | Posthepatic |
|---|---|---|---|---|
| Bilirubin type | Unconjugated ↑ | Unconjugated ↑ | Conjugated ↑ | Conjugated ↑ |
| Bilirubinuria | ✗ | ✗ | ✓ | ✓ |
| Urine urobilinogen | ↑↑ | ↑ | ↓ | ↓/absent |
| Stool color | Dark | Normal | Pale | Pale/clay |
| ALT/AST | Normal | ↑↑ | ↑ | Normal/↑ |
| ALP/GGT | Normal | ↑ | ↑ | ↑↑↑ |
| Coombs test | ± positive | Negative | Negative | Negative |
8. Special Notes on Bilirubin Measurement
- Van den Bergh reaction (diazo method):
- Direct bilirubin = conjugated (reacts directly with diazo reagent in aqueous)
- Indirect bilirubin = unconjugated (requires methanol to release from albumin)
- Total bilirubin = direct + indirect
- Normal total serum bilirubin: 0.3–1.0 mg/dL (< 0.3 mg/dL direct)
Sources: Basic Medical Biochemistry: A Clinical Approach 6e; Harrison's Principles of Internal Medicine 22E; Schwartz's Principles of Surgery 11e; Robbins, Cotran & Kumar Pathologic Basis of Disease; Sleisenger & Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.