Explain about Ranula
Reading File
Finding Sources
Finding Sources
Searching PubMed
ranula oral floor mouth cyst
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive, well-sourced information with clinical images. Here is the full answer:
Ranula
Definition and Etymology
A ranula (Latin: rana = frog; literally "little frog") is a fluid-filled mucous extravasation pseudocyst arising from the floor of the mouth, most commonly from the sublingual salivary gland or its ducts. The name was coined because a large intraoral ranula resembles the translucent belly of a frog, and the associated voice change produces a frog-like croaking quality. It was first described by Banister in his surgical compilation of 1585.
The prevalence is approximately 0.2 cases per 1000 people, and it is most commonly detected in the second decade of life, with a possible female predisposition. - Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Classification
Ranulas are classified into two main types based on their anatomical extent:
| Type | Description |
|---|---|
| Simple (Intraoral) Ranula | Confined to the floor of the mouth, above the mylohyoid muscle |
| Plunging (Cervical / Diving) Ranula | Extends through or below the mylohyoid muscle into the neck (submandibular or submental region), with or without an intraoral component |
Simple ranulas are much more common than plunging ranulas. A plunging ranula may occasionally extend to the upper chest wall in rare cases. - Scott-Brown's Otorhinolaryngology Head & Neck Surgery - Vol 2
Aetiology and Pathogenesis
Ranulas are extravasation pseudocysts - they do not have a true epithelial lining but are instead walled off by loose connective tissue (this distinguishes them histologically from lymphatic malformations, which have a simple epithelial lining).
Causes:
- Obstruction of a sublingual salivary gland or its ducts (most common acquired cause)
- Trauma to the sublingual gland duct (e.g., following floor-of-mouth procedures or injury)
- Congenital - less common; a congenital predisposition to plunging ranula has been suggested based on higher incidence among certain ethnic groups and siblings
- HIV infection - increased occurrence documented in HIV-positive individuals, likely due to peri-ductal inflammation and fibrosis (HIV-associated salivary gland disease)
The mechanism involves rupture of the main duct or obstructed acini of the sublingual gland, with mucous extravasation collecting in the floor of the mouth. In plunging ranulas, the mucus escapes through defects in the mylohyoid muscle - the so-called "boutonniere anomaly." - Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Clinical Features
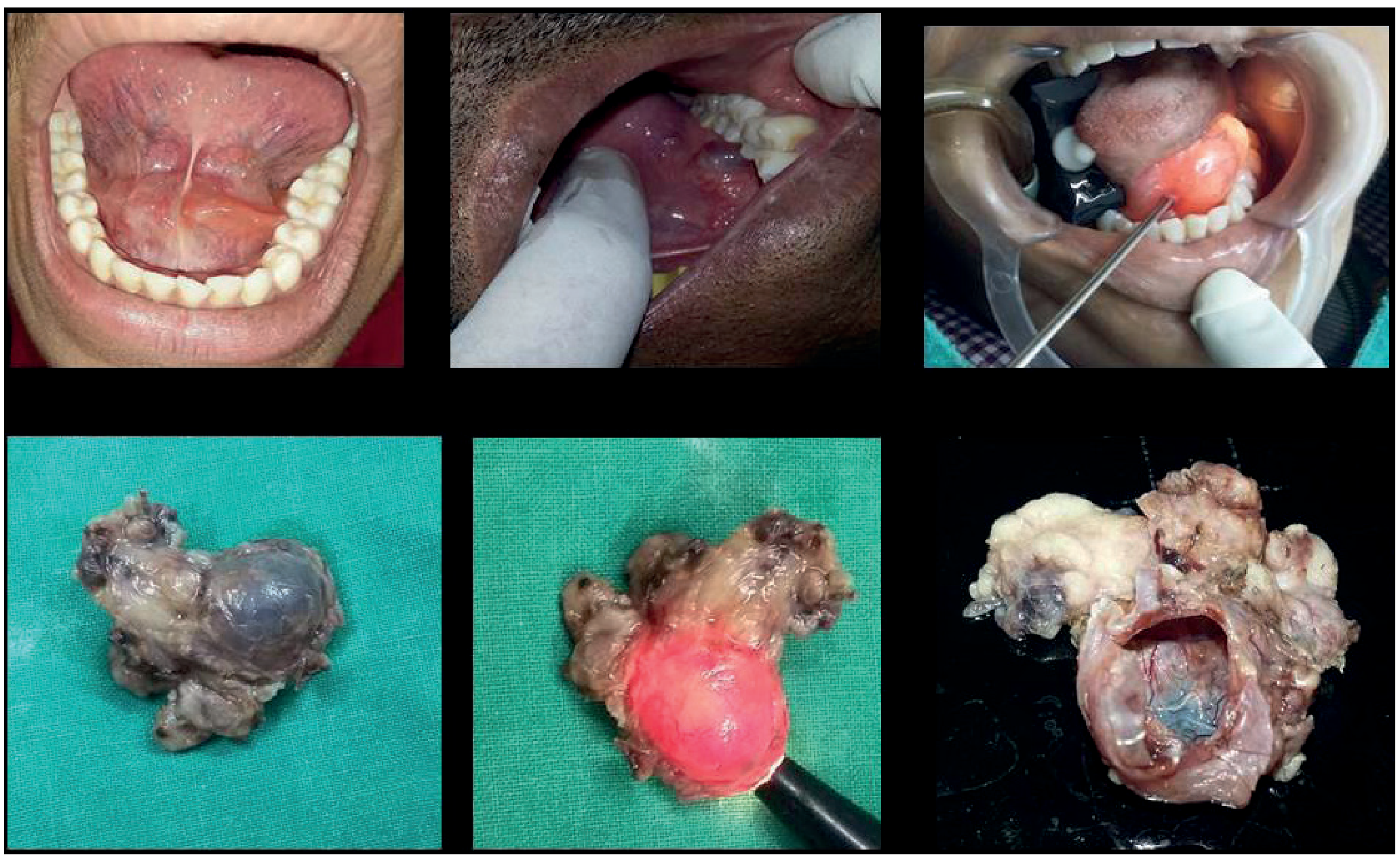
Simple (Intraoral) Ranula
- Smooth, soft, fluctuant, painless swelling in the floor of the mouth
- Characteristic bluish, translucent appearance (due to thin overlying mucosa and underlying fluid)
- Almost always unilateral, typically to one side of the frenulum linguae
- The submandibular (Wharton's) duct may be visible traversing the dome of the swelling
- Large ranulas may fill the entire floor of the mouth
- If large enough: may elevate the tongue and interfere with swallowing, speech, mastication, or respiration
Plunging (Cervical) Ranula
- Presents as a painless, persistent or recurrent neck swelling in the submandibular or submental region
- Bimanual palpation reveals cross-fluctuation between the floor of the mouth and the cervical extension
- Rarely spreads to the upper chest
- Respiratory obstruction is rare but can occur
- Clinically difficult to differentiate from a lymphatic malformation
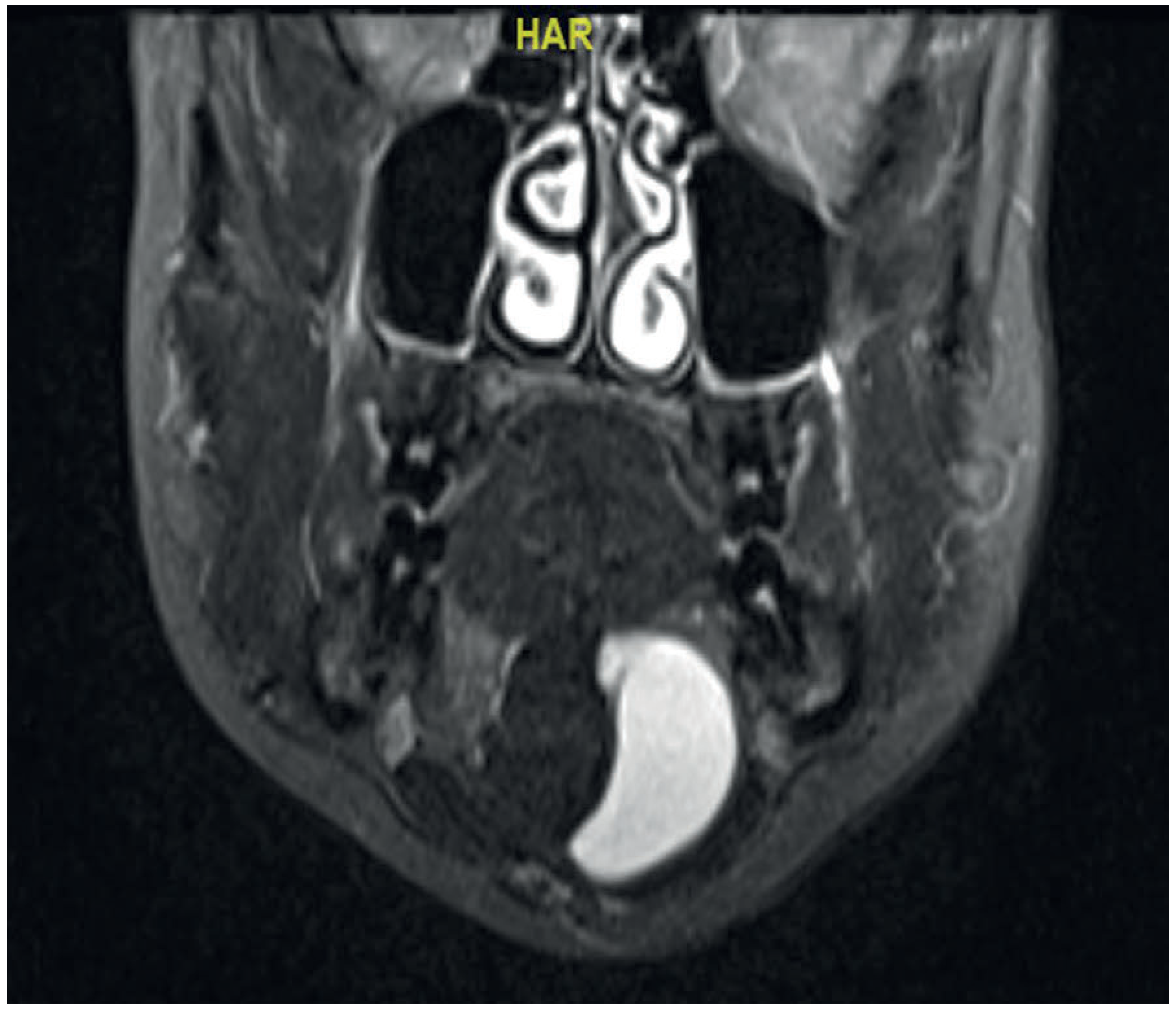
Investigations
- Simple intraoral ranula: Imaging is usually not needed for clinical diagnosis
- Indications for imaging: history of previous surgery, cervical component, or diagnostic uncertainty
- MRI is the preferred modality - it best delineates soft tissue anatomy and extent of a plunging ranula
- FNAC / aspiration: Yields thick, sticky, mucoid saliva - this distinguishes it from a lymphangioma (which yields clear watery fluid)
- FNA / cytological examination may be used for diagnostic confirmation alongside radiology
Differential Diagnosis
| Condition | Key Distinguishing Features |
|---|---|
| Lymphatic malformation | Epithelial-lined histologically; watery fluid on aspiration; may respond differently to treatment |
| Sublingual dermoid | Opaque, non-translucent; doughy on palpation; contains keratin debris |
| Thyroglossal cyst | Midline; moves on swallowing and tongue protrusion |
| Branchial cyst | Lateral neck; older presentation |
| Submandibular sialadenitis/calculus | Pain; firm swelling; calculus on imaging |
Treatment
Key Principle
Because the sublingual gland has multiple ducts, ranulas recur at high rates if the gland itself is not removed. Excision of the sublingual gland is the cornerstone of definitive management.
Surgical Options
| Method | Notes |
|---|---|
| Simple aspiration/drainage | Very high recurrence rate - not recommended as definitive treatment |
| Marsupialization | For plunging ranulas: 80% recurrence rate - inadequate alone |
| Excision of ranula + sublingual gland | Treatment of choice - recurrence rate as low as 3.6% in retrospective studies |
| Laser excision | Alternative for intraoral ranulas; low recurrence and complication rates reported |
| Transoral approach | Used for intraoral masses |
| External transcervical approach | Used for predominantly submental or cervical masses |
- During surgery, care must be taken to identify and preserve the lingual nerve (which lies in close proximity) and the Wharton's (submandibular) duct - K.J. Lee's Essential Otolaryngology
Non-Surgical / Minimally Invasive Options
- OK-432 (Picibanil) sclerotherapy: Injection of this streptococcal-derived immunomodulator has been reported as a primary, non-surgical treatment. Produces local inflammation and fibrosis. Experience in paediatric patients is still limited.
- Botulinum toxin injection: Has shown good success rates in some studies but requires further evaluation.
- Oral nickel gluconate: An emerging medical treatment; Garofalo et al. reported promising results with no recurrence in their case series, thought to promote salivary gland tissue repair.
Complications (Post-surgical)
- Injury to the lingual nerve (risk of sensory loss)
- Injury to the Wharton's duct - possible stenosis, obstructive sialadenitis
- Ductal laceration
- Bleeding and haematoma
Recent Evidence
A 2025 systematic review and meta-analysis (PMID: 39435706) titled "Sublingual ranulas, is it time for a new classification?" revisited the classification of ranulas, suggesting the existing simple vs. plunging dichotomy may need to be expanded to better reflect clinical and anatomical variability. This is the most current high-quality evidence on the topic.
Summary in brief: A ranula is a mucous extravasation pseudocyst of the sublingual gland presenting as a bluish, translucent floor-of-mouth swelling (simple type) or a neck mass (plunging type). Definitive treatment is excision together with the sublingual gland to prevent recurrence. MRI is preferred when the diagnosis is uncertain or when a cervical component is present.
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Vol 1 & 2), Bailey and Love's Short Practice of Surgery 28th Ed., K.J. Lee's Essential Otolaryngology, S. Das Manual on Clinical Surgery 13th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.