Placetal pervia
Reading File
Finding Sources
Searching PubMed
"placenta previa"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough overview of Placenta Previa (note the correct spelling: previa, not pervia), synthesized from multiple authoritative sources.
Placenta Previa
Definition
Placenta previa occurs when the placenta implants over or covers the internal cervical os. It is a leading cause of antepartum hemorrhage.
- Placenta previa: placenta covers the internal os
- Low-lying placenta: placental edge is within 2 cm of the internal os but does not cover it
- If the placental edge is >20 mm from the internal os, position is reported as "normal"
The older classification system (complete, partial, marginal previa) is no longer recommended. Modern practice uses only "previa" vs. "low-lying."
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1018
Incidence
- Affects approximately 0.5% of all third-trimester pregnancies
- Identified on 10% of mid-trimester ultrasounds
- At least 90% of low-lying placentas identified early in pregnancy resolve by the third trimester ("placental migration" - technically trophotropism, not true migration)
Pathogenesis & Risk Factors
The underlying cause is unknown but involves implantation in the lower uterine segment, often associated with prior endometrial damage or uterine scarring.
| Risk Factor | Increased Risk |
|---|---|
| Previous placenta previa | 8× |
| Previous cesarean section | 1.5-15× |
| Age >35 years | 4.73× |
| Age >40 years | 9× |
| Previous suction curettage for abortion | 1.33× |
| Multiparity | 1.1-1.73× |
| Smoking | Increased |
Bleeding mechanism: as the lower uterine segment elongates and the cervix effaces/dilates with advancing gestation or labor onset, marginal placental vessels are torn, causing hemorrhage.
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1018
- Rosen's Emergency Medicine, p. 3355
Clinical Features
- Cardinal symptom: Painless, bright-red vaginal bleeding (classically in the third trimester)
- "Herald bleeds" - small warning bleeds may precede major hemorrhage
- In ~10% of cases, no bleeding occurs until onset of labor
- ~20% of cases have some degree of uterine irritability (usually minor)
- Critical rule: All patients with painless second-trimester vaginal bleeding should be assumed to have placenta previa until proven otherwise
Do NOT perform digital or instrumental cervical examination before ruling out placenta previa by ultrasound - this can precipitate severe hemorrhage.
Diagnosis
Transvaginal ultrasound (TVUS) is the gold standard - it is safe, accurate, and provides precise measurement of the placenta-to-os distance. The bladder should be emptied before examination to avoid overdiagnosis.
Figure: Suspected placenta previa at 17 weeks (abdominal ultrasound - placenta centrally located over the cervix):
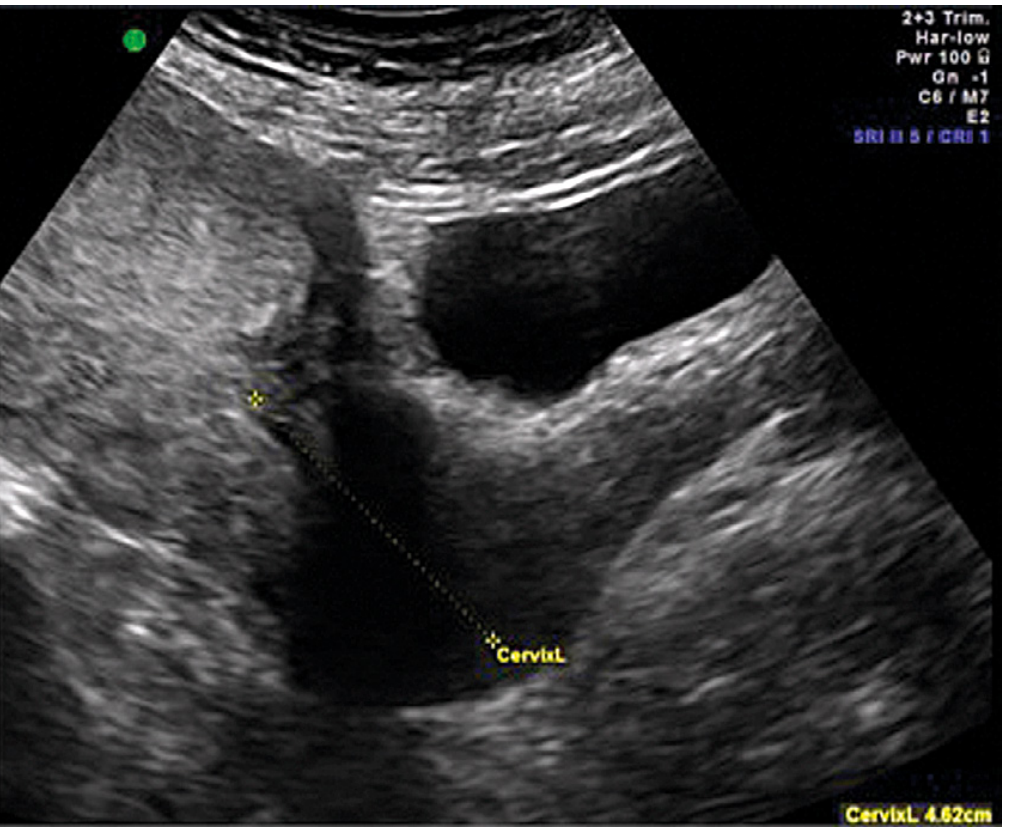
Figure: MRI of placenta previa - coronal T2-weighted MRI showing low-lying placenta (asterisk) covering the internal os:
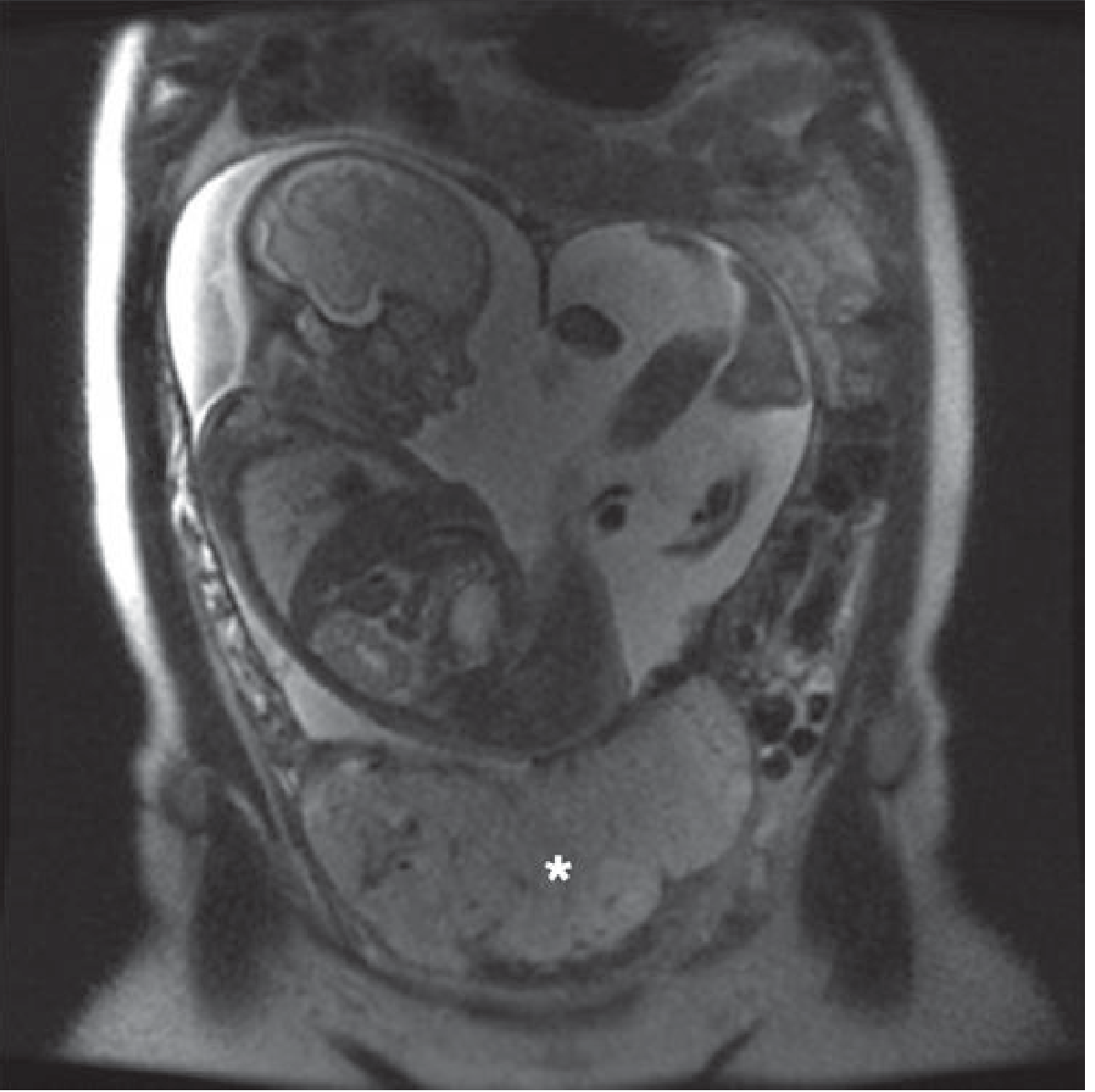
MRI is used in equivocal cases or when placenta accreta syndrome is suspected.
Differential Diagnosis
- Low-lying placenta
- Placental abruption (painful bleeding vs. painless)
- Localized uterine contraction mimicking low-lying placenta
- Placenta accreta
- Vasa previa
- Succenturiate lobe
- Vaginal/cervical lesions (hemorrhoids, polyps, cervicitis)
Associated Conditions
- Placenta accreta spectrum (abnormal invasion of placental tissue into the myometrium) - risk increases significantly with prior cesarean + anterior previa
- Vasa previa - umbilical cord vessels traverse fetal membranes overlying the os; rupture can cause rapid fetal exsanguination
Management
Acute hemorrhage (Emergency Department/Initial stabilization)
- Two large-bore IV lines + fluid resuscitation
- Continuous fetal monitoring
- Baseline CBC (hemoglobin), type and crossmatch
- Coagulation studies: platelet count, PT, aPTT, fibrinogen (normal in pregnancy: 400-450 mg/dL; <300 mg/dL = significant coagulopathy)
- Fresh-frozen plasma or fresh whole blood if coagulopathy develops
- Rh-negative patients: 300 µg Rh immune globulin within 72 hours if not yet given at 28 weeks
- Urgent obstetric consultation; transfer to obstetric unit
Ongoing management (Obstetric care)
| Scenario | Management |
|---|---|
| Placental edge >20 mm from os | Normal vaginal delivery may be possible |
| Placenta ≤1 cm from os or covering os | Cesarean section recommended |
| Unstable/major hemorrhage | Emergency cesarean delivery |
| Mid-trimester previa, stable | Expectant management; repeat ultrasound in third trimester |
- Rosen's Emergency Medicine, pp. 3355-3356
- Creasy & Resnik's Maternal-Fetal Medicine, p. 1018
- Grainger & Allison's Diagnostic Radiology, p. 915
Key Points to Remember
- Painless third-trimester bleeding = placenta previa until proven otherwise
- Never do digital vaginal exam before ultrasound
- TVUS is the diagnostic method of choice - it is safe even in previa
- Old terminology (complete/partial/marginal) is obsolete; use "previa" or "low-lying"
- Most mid-trimester previas resolve by term (trophotropism)
- Always check for associated placenta accreta, especially with prior uterine surgery
Recent evidence note: A 2025 meta-analysis (PMID: 40472373) confirmed significantly elevated risk of postpartum hemorrhage in patients with low-lying placenta, reinforcing current guideline recommendations for cesarean delivery when the placental edge is ≤1 cm from the os.
This is a shared conversation. Sign in to Orris to start your own chat.