Liver abscess
Reading File
Finding Sources
Searching PubMed
"liver abscess" management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading Article
PMID: 40958348
Loading Image
Loading Image
I now have comprehensive material from multiple authoritative textbooks and recent evidence. Here is a thorough, well-structured answer.
Liver Abscess
A liver abscess is a collection of pus within the hepatic parenchyma. Three major categories exist: pyogenic (bacterial), amebic, and fungal. Pyogenic liver abscess (PLA) accounts for the majority of cases in developed countries. Incidence is approximately 1 per 5,000 hospital admissions. - Bailey & Love's Short Practice of Surgery 28th Ed.
1. Classification & Etiology
| Type | Cause | Key Feature |
|---|---|---|
| Pyogenic (PLA) | Bacteria (polymicrobial) | Most common in developed world |
| Amebic (ALA) | Entamoeba histolytica | Travel to endemic areas |
| Fungal | Candida spp. | Immunocompromised hosts |
2. Pyogenic Liver Abscess (PLA)
Routes of Infection
Five main pathways for hepatic seeding:
- Biliary tract disease (most common, ~35%) - cholangitis, cholecystitis, biliary obstruction from stones or malignancy, post-biliary surgery/endoscopy
- Portal vein pyemia (~20%) - ascending infection from appendicitis, diverticulitis, IBD, perforated peptic ulcer, peritonitis
- Trauma - blunt or penetrating hepatic injury
- Hematogenous - via hepatic artery from systemic bacteremia (e.g., endocarditis)
- Cryptogenic (~40%) - no identifiable source; frequently associated with Klebsiella pneumoniae and occult colonic malignancy
The historic paradigm of young patients with appendicitis causing PLA via pylephlebitis has given way to older men with biliary disease as the most common scenario - Sleisenger & Fordtran's GI and Liver Disease
Cryptogenic PLA and colon cancer: Multiple studies have linked cryptogenic PLA to underlying colonic malignancy, and some guidelines recommend colonoscopy after diagnosis of cryptogenic PLA to rule out occult cancer. - Current Surgical Therapy 14e
Risk Factors
- Age
- Diabetes mellitus (increases recurrence risk 12-38%)
- Biliary malignancy or instrumentation
- Immunosuppression
- Liver transplant
- Proton pump inhibitor use (independent risk factor - may allow gut bacterial overgrowth)
- Cirrhosis
Microbiology
Most PLAs are polymicrobial. Common organisms:
Gram-negative aerobes: E. coli, Klebsiella pneumoniae, Proteus, Pseudomonas
Gram-positive aerobes: Streptococcus milleri (anginosus) group, Enterococcus
Anaerobes: Bacteroides fragilis, Fusobacterium necrophorum, anaerobic streptococci
Special patterns:
- Biliary-origin PLAs: E. coli, Klebsiella, Enterococcus
- Enteric-origin PLAs: Bacteroides and anaerobes
- Cryptogenic PLAs: often monomicrobial K. pneumoniae (virulent strains can cause metastatic infection - endophthalmitis, meningitis)
- Fungal abscesses (Candida): hematologic malignancy patients
3. Clinical Features
| Feature | Frequency |
|---|---|
| Fever | ~90% |
| Leukocytosis | ~90% |
| Abdominal pain (RUQ) | ~60% |
| Elevated alkaline phosphatase | ~80% |
| Hyperbilirubinemia | ~50% |
| Transaminitis | ~50% |
Other findings: malaise, weight loss, anorexia, hepatomegaly, liver tenderness on percussion. Jaundice is a late and poor prognostic sign. A cough from diaphragmatic irritation may be present. Splenomegaly is unusual except in chronic abscess. - Sleisenger & Fordtran's
4. Diagnosis
Imaging
CT with IV contrast is the gold standard (sensitivity approaching 100%). PLAs appear hypoattenuated with possible loculations and peripheral rim enhancement (present in <20% but specific for abscess). CT also detects gas within the abscess (associated with higher mortality) and identifies underlying biliary etiology.
Ultrasound is less sensitive but is lower cost, radiation-free, and preferred in pediatrics. It can detect abscesses as small as 1 cm and guide needle aspiration.
Laboratory
- Blood cultures (positive in >50% of PLA cases)
- Aspiration cultures (90% yield if pre-antibiotic)
- CBC: leukocytosis, anemia
- LFTs: elevated ALP, bilirubin, transaminases
- Elevated ESR
Differential Diagnosis
Simple hepatic cysts, hydatid cyst, necrotic tumor (HCC, metastases), hepatic hematoma, biloma.
5. Treatment
A. Pyogenic Liver Abscess
Antibiotics
Empiric broad-spectrum therapy should cover streptococci, gram-negative bacilli, and anaerobes until culture results guide de-escalation:
- Piperacillin/tazobactam (monotherapy) - standard first-line
- Ceftriaxone + metronidazole - alternative
- Carbapenems - if history of biliary instrumentation/transplant (ESBL coverage)
Metronidazole or clindamycin are critical for anaerobic coverage and excellent abscess penetration. Third-generation cephalosporins and aminoglycosides cover gram-negatives effectively.
Duration: guided by clinical response and imaging resolution at 4-6 weeks follow-up. - Current Surgical Therapy 14e
Drainage - Standard of Care
Drainage is the cornerstone of PLA management:
| Abscess Size | Approach |
|---|---|
| <3 cm | Antibiotics alone may suffice |
| >5 cm | Percutaneous catheter drainage (PCD) recommended |
| >10 cm | PCD (may need multiple catheters) |
| Ruptured / concurrent intra-abdominal abscess | Surgical drainage |
Percutaneous catheter drainage (PCD) is recommended over needle aspiration alone for abscesses >5 cm. A 2025 meta-analysis of 12 studies (1,290 patients) found that PCD showed:
- Higher treatment success (RR 1.19, 95% CI 1.10-1.29, p<0.001)
- Faster clinical improvement (1.92 days shorter, p<0.001)
- Lower 6-month recurrence (RR 0.44, 95% CI 0.26-0.75, p<0.001)
- With comparable complication rates
Surgery
Open or laparoscopic drainage is reserved for cases failing percutaneous approaches, abscess rupture with peritonitis, or concurrent intra-abdominal pathology requiring surgical correction (e.g., perforated viscus, biliary reconstruction).
Recurrent/Refractory Abscesses
Usually occur when the initial abscess was large, there are multiple abscesses, or there is ongoing biliary communication. Surgical drainage or hepatic resection may be needed in this setting. - Bailey & Love's
6. Amebic Liver Abscess (ALA)
Epidemiology & Pathophysiology
- Caused by Entamoeba histolytica (protozoan)
- 10:1 male-to-female predominance
- Usually single abscess in the right hepatic lobe, near the diaphragm
- Cysts ingested via fecally contaminated food/water → colitis → trophozoites invade intestinal mucosa → portal seeding → hepatic abscess, typically 2-4 months after colonic amebiasis
- Classic abscess contents: thick, proteinaceous, brown "anchovy paste" fluid
Diagnosis
Presentation similar to PLA (fever, RUQ pain, leukocytosis, elevated ALP). Imaging cannot reliably distinguish PLA from ALA.
Key diagnostic steps:
- Travel history to endemic areas (Mexico, India, Africa, Southeast Asia)
- Amebic serology (ELISA, indirect hemagglutination) - highly sensitive
- Antigen testing more specific than antibody serology (1/3 of prior E. histolytica infection patients retain antibodies without active infection)
- Stool O&P: positive in only ~50%
Comparison Table: PLA vs ALA
| Parameter | Pyogenic (PLA) | Amebic (ALA) |
|---|---|---|
| Number | Often multiple | Usually single |
| Location | Either lobe | Right hepatic lobe, near diaphragm |
| Presentation | Subacute | Acute |
| Age/sex | Older patients, male predominance | Young to middle-aged, strong male predominance (10:1) |
| Travel history | No | Yes (endemic area) |
| Serology | Negative | Positive |
| Organisms | Bacteria | E. histolytica |
| Abscess contents | Pus (foul-smelling) | "Anchovy paste" |
- Sleisenger & Fordtran's
Treatment of ALA
Antiparasitic regimen (dual therapy required):
- Oral metronidazole 500-750 mg TID x 7-10 days - highly effective (>90% response)
- PLUS luminal agent to eliminate intestinal cysts and prevent recurrence:
- Paromomycin 10 mg/kg TID x 7 days, OR
- Diiodohydroxyquin (iodoquinol) 650 mg TID x 20 days
Drainage is NOT routinely indicated for ALA. Prospective studies have not demonstrated benefit of early aspiration. Reserve PCD for:
- No clinical response to antibiotics
- Suspicion of secondary bacterial superinfection (broaden antibiotics + drain)
Important contrast: Drainage is standard of care for PLA but not indicated for uncomplicated ALA. - Current Surgical Therapy 14e
7. Fungal Hepatic Abscess
- Almost exclusively in immunocompromised patients, particularly those with hematologic malignancies (leukemia, lymphoma)
- Highest mortality among all types
- Caused mainly by Candida species
- Treated with systemic antifungals (amphotericin B or azoles based on species)
8. Complications
- Rupture into peritoneum (peritonitis), pleural cavity (empyema, fistula), or pericardium (tamponade)
- Right pleural effusion / subphrenic abscess
- Portal vein thrombosis / portal hypertension
- Septicemia, multi-organ failure
- Metastatic infection (with virulent K. pneumoniae strains: endophthalmitis, meningitis)
9. Prognosis
Mortality has declined significantly with improved imaging, percutaneous drainage techniques, and effective antibiotics. Prognosis is now largely determined by the underlying cause and comorbidities rather than the abscess itself. Recurrence risk is 12-38%, especially in diabetics and when the responsible organism is not identified. - Bailey & Love's
Sources:
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Ch. 84
- Bailey and Love's Short Practice of Surgery, 28th Ed., Ch. 69
- Current Surgical Therapy, 14th Ed.
- Li & Pan, Medicine 2025 - Meta-analysis: PCD vs PA for liver abscess (PMID 40958348)
Describe the various minimally invasive treatment modalities for hydatid cysts of the liver
Reading File
Finding Sources
Searching PubMed
"hydatid cyst" liver percutaneous treatment
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I have excellent, comprehensive material from four major surgical textbooks. I now have enough to write a thorough, well-structured response.
Minimally Invasive Treatment Modalities for Hydatid Cysts of the Liver
Overview and General Principles
Hepatic hydatid cysts (caused by Echinococcus granulosus) present a unique management challenge because of the risk of anaphylaxis and peritoneal seeding if cyst contents spill. Three overarching principles govern all approaches - including minimally invasive ones:
- Eradication of the parasite within the cyst
- Protection of the host against spillage of scoleces (using scolicidal agents)
- Management of residual cavity and complications
Asymptomatic, inactive, or small (<4 cm) deeply located cysts can be managed conservatively with observation. Active cysts should receive a full course of albendazole before any intervention. - Bailey & Love's
Contraindications to minimally invasive approaches include: biliary communication, pulmonary communication, and peritoneal rupture - all of which mandate open surgery. - Maingot's Abdominal Operations
Role of Medical Therapy (Anthelmintic - Adjunct to All Approaches)
Albendazole is the drug of choice. It is well absorbed from the intestine and activated by hepatic metabolism to its active sulfoxide form. Mebendazole is poorly absorbed and inactivated by the liver, making it inferior.
- Used alone, benzimidazoles achieve only ~30% success rate
- Given for at least 3 months preoperatively, albendazole reduces cyst viability, recurrence risk, and the consequences of inadvertent spillage
- If spillage occurs intraoperatively, therapy should continue for at least 1 month postoperatively
- Praziquantel may be added preoperatively to further reduce scolex viability
Medical therapy alone (without drainage) is reserved for widely disseminated disease or patients unfit for any procedural intervention. - Maingot's, Sabiston
1. PAIR (Puncture - Aspiration - Injection - Re-Aspiration)
PAIR is the most widely used and best-studied percutaneous technique. The historic taboo against percutaneous puncture of hydatid cysts (due to fear of anaphylaxis and seeding) was challenged by Fornage in 1983, who reported an accidental puncture without clinical consequences. Multiple successful series followed.
Steps of the PAIR Technique
- Puncture: The cyst wall is punctured under ultrasound or CT guidance using a fine needle (typically 18-22 gauge)
- Aspiration: Cyst fluid is aspirated completely - fluid is characteristically clear and colorless ("hydatid water"). Suction must be capable of high negative pressures
- Injection: A protoscolecidal (scolicidal) agent is instilled into the cyst cavity and left for 15-30 minutes. Contrast may be injected first to opacify the cyst and rule out biliary communication
- Re-aspiration: The scolicidal solution and residual contents are completely re-aspirated
Scolicidal Agents Used in PAIR
| Agent | Concentration | Notes |
|---|---|---|
| Hypertonic saline | 15-20% | Most common; must rule out biliary communication first (risk of hypernatremia/sclerosing cholangitis) |
| Ethanol | 95% | Effective; used alone or combined with saline |
| Hypertonic saline + ethanol | 30% + 95% | Combined regimen |
| Povidone-iodine | 10% | Effective scolicidal |
| Cetrimide | 0.5% | Relatively low risk per WHO |
| Chlorhexidine gluconate | 0.04% | Emerging agent - non-toxic to bile ducts, not dilution-sensitive, 100% effective on protoscoleces; may become preferred |
Important safety rule: No agent should be injected pre-evacuation due to high intracyst pressure - injection before aspiration risks rupture and systemic spread. - Maingot's
WHO classification of scolicidal agents (by safety):
- Relatively low risk: ethanol (70-95%), hypertonic saline (15-20%), cetrimide 0.5%
- Formalin and hydrogen peroxide have been abandoned due to toxic biliary effects
Patient Selection for PAIR (WHO-PAIR criteria)
- Gharbi type I or II cysts (unilocular, non-complicated)
- Anterior and peripheral cysts
- 1-3 cysts
- Small-to-moderate size
- No calcification or minimal calcification
- No biliary communication (must be confirmed prior to scolicidal injection)
Results
- Two small randomized trials compared PAIR with surgery and with medical therapy, showing similar success rates, though both had methodologic limitations
- PAIR is now accepted in centers experienced with the technique and is endorsed by WHO as an alternative to surgery in selected patients
- Sabiston Textbook of Surgery
2. Percutaneous Catheter Drainage (Modified PAIR / MoCAS)
An extension of PAIR where a drainage catheter is left in situ rather than simple needle aspiration and re-aspiration. This allows:
- Prolonged evacuation of cyst contents
- Repeated irrigations with scolicidal agents
- Management of infected cysts
- Drainage of biliary communication (if identified post-procedure)
Sometimes called MoCAS (Modified Catheter Aspiration and Suction) in the literature. It is preferred over simple PAIR for:
- Larger cysts
- Infected cysts (functioning like a pyogenic abscess drain)
- When daughter cysts or debris preclude complete single-session aspiration
Both PAIR and percutaneous drainage are contraindicated when biliary or pulmonary communication is demonstrated - scolicidal agents injected into the biliary tree cause sclerosing cholangitis. - Maingot's
3. Laparoscopic Cyst Surgery
Laparoscopy is increasingly used and offers the advantages of minimally invasive access while allowing direct visualization, more complete clearance of daughter cysts, and formal management of biliary communications.
Patient Selection
Best suited for:
- Anteriorly placed, superficial cysts
- Cysts without thick calcified walls
- Segments VI-VII cysts (via right lateral approach)
- Gharbi type I or II cysts
- Not suitable for: posterior/central cysts, multiple (>3) cysts, heavily calcified cysts, biliary communication requiring formal repair
Technique: Laparoscopic Marsupialization (Deroofing)
This is the most commonly performed laparoscopic procedure:
- An 11 mm trocar is placed just above the cyst
- Scolicidal agent (10% povidone-iodine-soaked sponges, or hypertonic saline) is applied around the cyst field
- The cyst is aspirated with a 14-gauge needle (the endocyst shrinks back from the pericyst wall)
- The pericyst is opened (deroofed), and daughter cysts and germinal membrane are evacuated using suction and graspers
- The cyst cavity is irrigated with scolicidal solution
- Any biliary communication is identified and oversewn
- A pedicled omentum flap (omentoplasty) is sutured to the margins of the residual cavity to obliterate it, reduce bile leak, and prevent fluid collection
Technique: Laparoscopic Cystopericystectomy
For small, superficial cysts in experienced centers, the entire cyst is removed intact (cystopericystectomy/total pericystectomy) without entering the cyst, eliminating any risk of spillage. This is the most "radical" laparoscopic approach and carries the lowest recurrence rate but requires advanced laparoscopic hepatobiliary skills. - Bailey & Love's
Advantages of Laparoscopy over Open Surgery
- Reduced hospital stay
- Less postoperative pain
- Faster recovery
- Lower wound complications
- Similar efficacy for suitable cysts
Spillage Prevention (Critical)
- Trocar sites and peritoneal cavity are lined with hypertonic saline-soaked packs before cyst opening
- Closed aspiration systems are used to prevent aerosol contamination
- Preoperative albendazole (+ praziquantel) reduces scolex viability
- Intraoperative spillage of cyst contents is the primary cause of recurrence (8.5-25% postoperative recurrence rate in conservative surgery) - Maingot's
4. Endoscopic Retrograde Cholangiopancreatography (ERCP)
ERCP is not a primary treatment for hydatid cysts but plays an important adjunctive role when biliary communication exists:
- Biliary communication occurs in up to 80% of cases as cysts enlarge (through compression-related decubitus erosion of bile ducts) - Maingot's
- Clinical manifestations: jaundice, cholangitis, cyst infection, external biliary fistula post-surgery
- ERCP with sphincterotomy decompresses the biliary tree and can extract extruded membranes or daughter cysts that have entered the common bile duct
- Biliary stenting via ERCP can also manage postoperative biliary fistulae (12-33% of patients with biliary communication require biliary drainage postoperatively)
- ERCP is preferred over surgical bile duct exploration in many centers when the communication is not amenable to simple suture repair
5. Summary: Selection Framework
| Feature | Preferred Approach |
|---|---|
| Gharbi I/II, anterior, peripheral, 1-3 cysts, no biliary comms | PAIR or laparoscopic marsupialization |
| Infected cyst meeting above criteria | Percutaneous catheter drainage |
| Small, superficial cyst in expert center | Laparoscopic cystopericystectomy |
| Biliary communication present | Open surgery + ERCP if needed |
| Posterior/central/multiple/>3 cysts, heavy calcification | Open evacuation or resection |
| Peritoneal rupture | Open surgery |
| Pulmonary communication | Open surgery |
| Widely disseminated / unfit for procedures | Albendazole alone |
Recurrence Rates
| Approach | Recurrence Rate |
|---|---|
| Open-cyst evacuation (conservative) | 10-30% |
| Laparoscopic (conservative) | 8.5-25% (spillage-related) |
| Total pericystectomy / hepatic resection | 1-5% (in experienced centers) |
| PAIR | Low in selected cases; comparable to surgery in small trials |
Recurrence is primarily caused by:
- Intraoperative spillage of protoscolex-rich fluid
- Incomplete removal of the germinal membrane
- Continued biliary communication
Sources:
- Maingot's Abdominal Operations - Ch. 43
- Sabiston Textbook of Surgery, 21e - Ch. 89
- Bailey & Love's Short Practice of Surgery, 28th Ed. - Ch. 69
- Schwartz's Principles of Surgery, 11th Ed. - Ch. 31
Describe the various minimally invasive treatment modalities for hydatid cysts of the liver
The answer to this question was covered in detail in my previous response. Here is the complete answer again for reference:
Minimally Invasive Treatment Modalities for Hydatid Cysts of the Liver
Overview and General Principles
Hepatic hydatid cysts (caused by Echinococcus granulosus) present a unique management challenge because of the risk of anaphylaxis and peritoneal seeding if cyst contents spill. Three overarching principles govern all approaches - including minimally invasive ones:
- Eradication of the parasite within the cyst
- Protection of the host against spillage of scoleces (using scolicidal agents)
- Management of residual cavity and complications
Asymptomatic, inactive, or small (<4 cm) deeply located cysts can be managed conservatively with observation. Active cysts should receive a full course of albendazole before any intervention. - Bailey & Love's
Contraindications to minimally invasive approaches include: biliary communication, pulmonary communication, and peritoneal rupture - all of which mandate open surgery. - Maingot's Abdominal Operations
Role of Medical Therapy (Albendazole - Adjunct to All Approaches)
Albendazole is the drug of choice. It is well absorbed and hepatically metabolized to its active sulfoxide form. Mebendazole is inferior due to poor absorption and hepatic inactivation.
- Alone, benzimidazoles achieve only ~30% success
- Given for at least 3 months preoperatively, albendazole reduces cyst viability and recurrence risk after spillage
- Praziquantel may be added preoperatively to further reduce scolex viability
- Post-procedure albendazole continues for at least 1 month if spillage occurs
Medical therapy alone is reserved for widely disseminated disease or patients unfit for any procedural intervention. - Maingot's, Sabiston
1. PAIR (Puncture - Aspiration - Injection - Re-Aspiration)
PAIR is the most widely used and best-studied percutaneous technique. The historic taboo against puncturing hydatid cysts was challenged in 1983 by Fornage, who reported an accidental puncture without clinical sequelae. It is now endorsed by the WHO as an alternative to surgery in selected patients.
Steps of PAIR
- Puncture - the cyst wall is punctured under ultrasound or CT guidance (fine needle, 18-22 gauge)
- Aspiration - all cyst contents are aspirated; fluid is typically clear ("hydatid water"). Contrast may be injected first to confirm no biliary communication
- Injection - a scolicidal agent is instilled and left for 15-30 minutes
- Re-aspiration - scolicidal solution and residual contents are fully re-aspirated
Critical rule: No scolicidal agent should be injected before aspiration because high intracyst pressure risks rupture and systemic seeding. - Maingot's
Scolicidal Agents
| Agent | Concentration | Notes |
|---|---|---|
| Hypertonic saline | 15-20% | Most commonly used; avoid if biliary comms present (hypernatremia, sclerosing cholangitis) |
| Ethanol | 70-95% | Used alone or combined with saline |
| Povidone-iodine | 10% | Widely available, effective |
| Cetrimide | 0.5% | WHO-approved low-risk agent |
| Chlorhexidine gluconate | 0.04% | Emerging preferred agent - non-toxic to bile ducts, not affected by dilution, 100% effective on protoscoleces and germinal membrane |
Formalin has been abandoned - it causes sclerosing cholangitis when it enters the biliary tree.
Patient Selection for PAIR
| Suitable | Unsuitable |
|---|---|
| Gharbi type I or II (unilocular/active) | Gharbi type IV or V (calcified/dead) |
| Anterior, peripheral cysts | Posterior or central cysts |
| 1-3 cysts | >3 cysts |
| No/minimal calcification | Heavy calcification |
| No biliary communication | Biliary communication present |
2. Percutaneous Catheter Drainage (Modified PAIR / MoCAS)
An evolution of PAIR where an indwelling drainage catheter is left in the cyst rather than performing a single-session aspiration. This allows:
- Prolonged and repeated drainage of cyst contents
- Serial irrigation with scolicidal agents over days
- Management of infected/superinfected cysts (functioning like a pyogenic abscess drain)
- Evacuation of viscous daughter cyst material that cannot be aspirated in a single session
This is preferred over simple PAIR for larger cysts, infected cysts, and those with thick debris. Both PAIR and catheter drainage are contraindicated when biliary or pulmonary communication is confirmed - scolicidal agents injected into the biliary system cause sclerosing cholangitis.
3. Laparoscopic Cyst Surgery
Laparoscopy is increasingly favored and bridges the gap between minimally invasive and open approaches, offering direct visualization, complete daughter cyst clearance, and the ability to formally manage biliary communications.
Best Suited For
- Anteriorly placed, superficial cysts
- Cysts without thick calcified walls
- Gharbi type I or II
- Segments VI-VII cysts (via right lateral port approach)
- 1-3 cysts
Not Suitable For
- Posterior/central/deeply embedded cysts
-
3 cysts or very large cysts
- Heavily calcified pericysts
- Confirmed biliary communication requiring formal biliary reconstruction
Technique A: Laparoscopic Marsupialization (Deroofing)
The most commonly performed laparoscopic procedure:
- An 11 mm port is placed just above the cyst
- Povidone-iodine-soaked sponges or hypertonic saline packs are placed around the field as a scolicidal barrier
- The cyst is aspirated with a 14-gauge needle (the endocyst shrinks away from the pericyst wall)
- The pericyst roof is resected (deroofed); daughter cysts and germinal membrane are evacuated with suction/graspers
- The cavity is irrigated with scolicidal solution
- Any biliary communication is identified and oversewn
- A pedicled omentum flap (omentoplasty) is sutured to the cyst margins to obliterate the dead space, reduce bile leak risk, and prevent fluid collection
Technique B: Laparoscopic Cystopericystectomy
For small, superficial cysts in expert centers - the entire cyst is excised intact without entering it (total pericystectomy). This eliminates all risk of spillage and carries the lowest recurrence rate, but demands advanced laparoscopic hepatobiliary expertise. - Bailey & Love's
Spillage Prevention (Critical)
- Peritoneal cavity and port sites lined with hypertonic saline-soaked packs before cyst opening
- Closed suction systems used throughout
- Preoperative albendazole (+/- praziquantel) reduces scolex viability before any manipulation
- Intraoperative spillage of protoscolex-rich fluid is the primary driver of recurrence (8.5-25% in conservative surgery) - Maingot's
4. ERCP (Endoscopic Retrograde Cholangiopancreatography)
ERCP is not a primary treatment but plays a critical adjunctive role when biliary communication exists.
- Biliary communication occurs in up to 80% of cases as enlarging cysts erode adjacent bile ducts
- Clinical presentations: jaundice, cholangitis, cyst superinfection, obstructive jaundice, external biliary fistula after surgery
- ERCP with sphincterotomy decompresses the biliary tree and allows extraction of membranes or daughter cysts that have migrated into the common bile duct
- Endoscopic biliary stenting manages postoperative biliary fistulae (12-33% of patients with biliary communication require postoperative biliary drainage) - Maingot's
- ERCP is preferred over open bile duct exploration for post-procedural biliary leak in many centers
5. Selection Framework Summary
| Cyst Characteristics | Recommended Approach |
|---|---|
| Gharbi I/II, anterior, peripheral, 1-3 cysts, no biliary comms | PAIR or laparoscopic marsupialization |
| Infected cyst (no biliary comms) | Percutaneous catheter drainage |
| Small, superficial cyst in expert center | Laparoscopic cystopericystectomy |
| Biliary communication confirmed | Open surgery ± ERCP |
| Posterior/central, multiple (>3), heavy calcification | Open evacuation or resection |
| Peritoneal rupture | Open surgery |
| Pulmonary communication | Open surgery |
| Disseminated disease / unfit for intervention | Albendazole alone |
Recurrence Rates Across Approaches
| Approach | Recurrence |
|---|---|
| Open conservative (evacuation only) | 10-30% |
| Laparoscopic (conservative, with spillage risk) | 8.5-25% |
| Total pericystectomy / hepatic resection | 1-5% in experienced centers |
| PAIR (selected patients) | Comparable to surgery in small RCTs |
Sources:
- Maingot's Abdominal Operations - Ch. 43
- Sabiston Textbook of Surgery, 21e - Ch. 89
- Bailey & Love's Short Practice of Surgery, 28th Ed. - Ch. 69
- Schwartz's Principles of Surgery, 11th Ed. - Ch. 31
Discuss the etiopathogenesis, classification, investigations and management of hepatic hydatid cyst
Reading File
Finding Sources
Finding Sources
Searching PubMed
"echinococcosis" AND "liver" AND "classification"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Hepatic Hydatid Cyst: Etiopathogenesis, Classification, Investigations, and Management
Part 1 - Etiopathogenesis
The Parasite
Hydatid disease (echinococcosis) is a zoonosis caused by the larval stage of the dog tapeworm Echinococcus granulosus (syn. Taenia echinococcus). Two species cause disease in humans:
- E. granulosus - most common; causes cystic echinococcosis; endemic in the Mediterranean, Middle East, South America, Australia, New Zealand, and Africa
- E. multilocularis - less common; causes alveolar echinococcosis; behaves like a malignant infiltrating tumor; 5-year mortality of ~70% and 10-year mortality ~94% untreated; endemic in central Europe, Russia, Turkey, China, Japan
Infection with echinococcal organisms is the most common cause of liver cysts in the world. Of all human infections, 50-75% involve the liver, 25% the lungs, and 5-10% follow the arterial system to other organs (spleen, brain, bone). - Maingot's
Life Cycle and Transmission
The life cycle requires two hosts:
Definitive host (dog/carnivore): The adult tapeworm lives in the proximal small bowel attached by hooklets. Thousands of eggs are shed daily into the feces. Eggs are highly resistant to temperature extremes and survive for long periods.
Intermediate host (sheep, cattle, pigs - and humans accidentally):
- Ingestion of ova from environment contaminated by dog feces (via contaminated food, water, vegetables, or direct contact with infected dogs)
- In the human duodenum, the protective chitinous layer is dissolved by gastric juice
- The released hexacanth embryo (oncosphere) burrows through the intestinal wall
- It enters the portal circulation (or lymphatics) and is transported to the liver - the first-pass filter and most frequently involved organ
- Those passing through the liver are trapped in the pulmonary capillary bed; the few escaping to systemic circulation may seed the brain, bones, or spleen
The definitive host closes the cycle by consuming the viscera (containing cysts) of slaughtered intermediate hosts.
Humans are accidental dead-end intermediate hosts - there is no human-to-human transmission. - Sabiston, Maingot's
Prevention: Handwashing after contact with dogs, avoiding ground-level vegetables, and prohibiting the feeding of animal entrails to dogs are effective public health measures.
Cyst Growth and Structure
Once in the liver, cysts grow:
- 1 cm in the first 6 months
- 2-3 cm annually thereafter
- They are frequently very large at presentation (often >10 cm) because growth is slow and initially asymptomatic
The fully developed hydatid cyst has a three-layer wall:
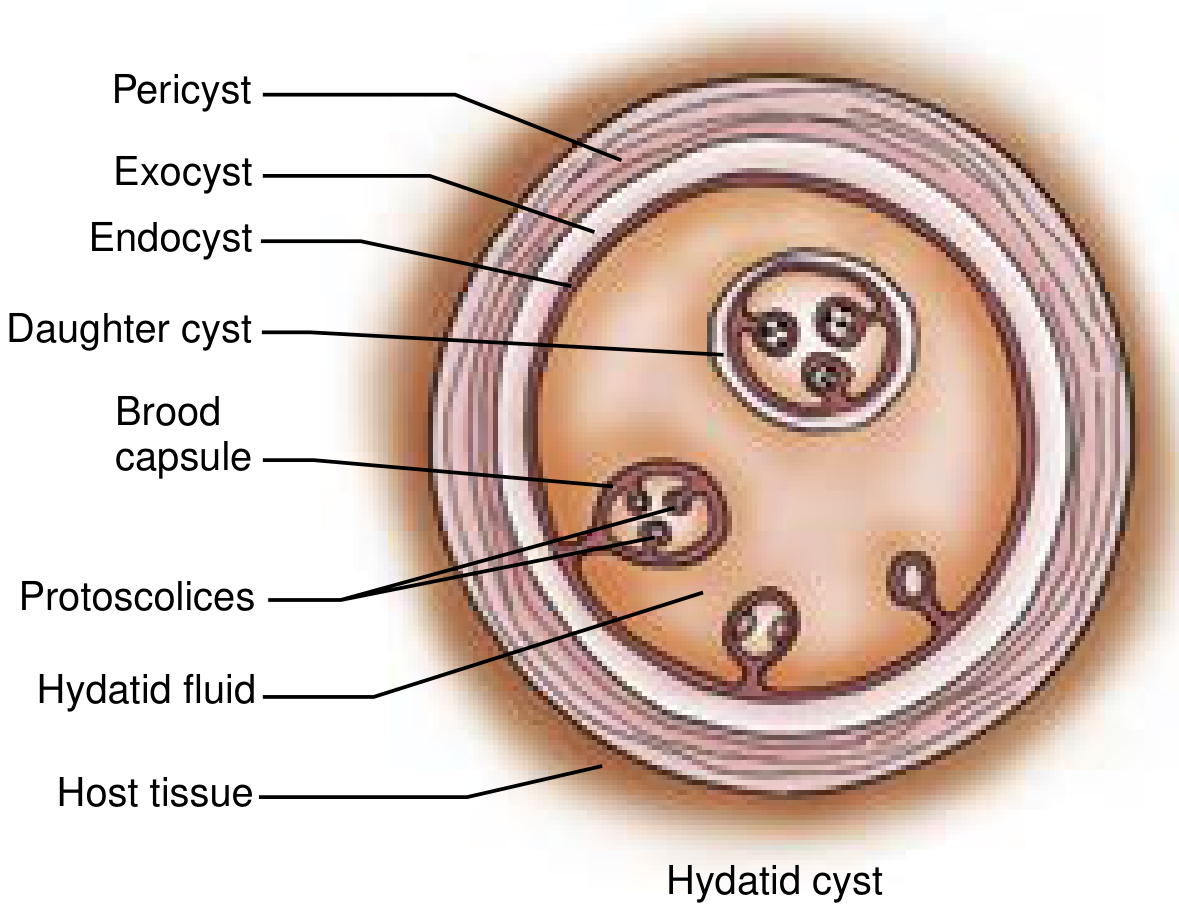
| Layer | Also Called | Origin | Structure & Function |
|---|---|---|---|
| Outermost | Pericyst | Host tissue reaction | Compressed host hepatocytes + fibrous tissue. Acts as mechanical support and metabolic interface. Incorporates bile ducts and blood vessels as it expands - explaining biliary/hemorrhagic complications. Calcifies over time (in ~50% of patients) |
| Middle | Ectocyst / Exocyst / Laminated membrane | Parasite-derived | Bluish-white, gelatinous, chitinous layer ~0.5 cm thick. Acellular (no nuclei). Acts as a selective barrier - blocks bacteria but allows protein molecules through. Non-infective |
| Innermost | Endocyst / Germinal layer | Parasite-derived | 10-25 μm thick. The biologically active layer. Produces hydatid fluid, the ectocyst, brood capsules, scoleces, and daughter cysts |
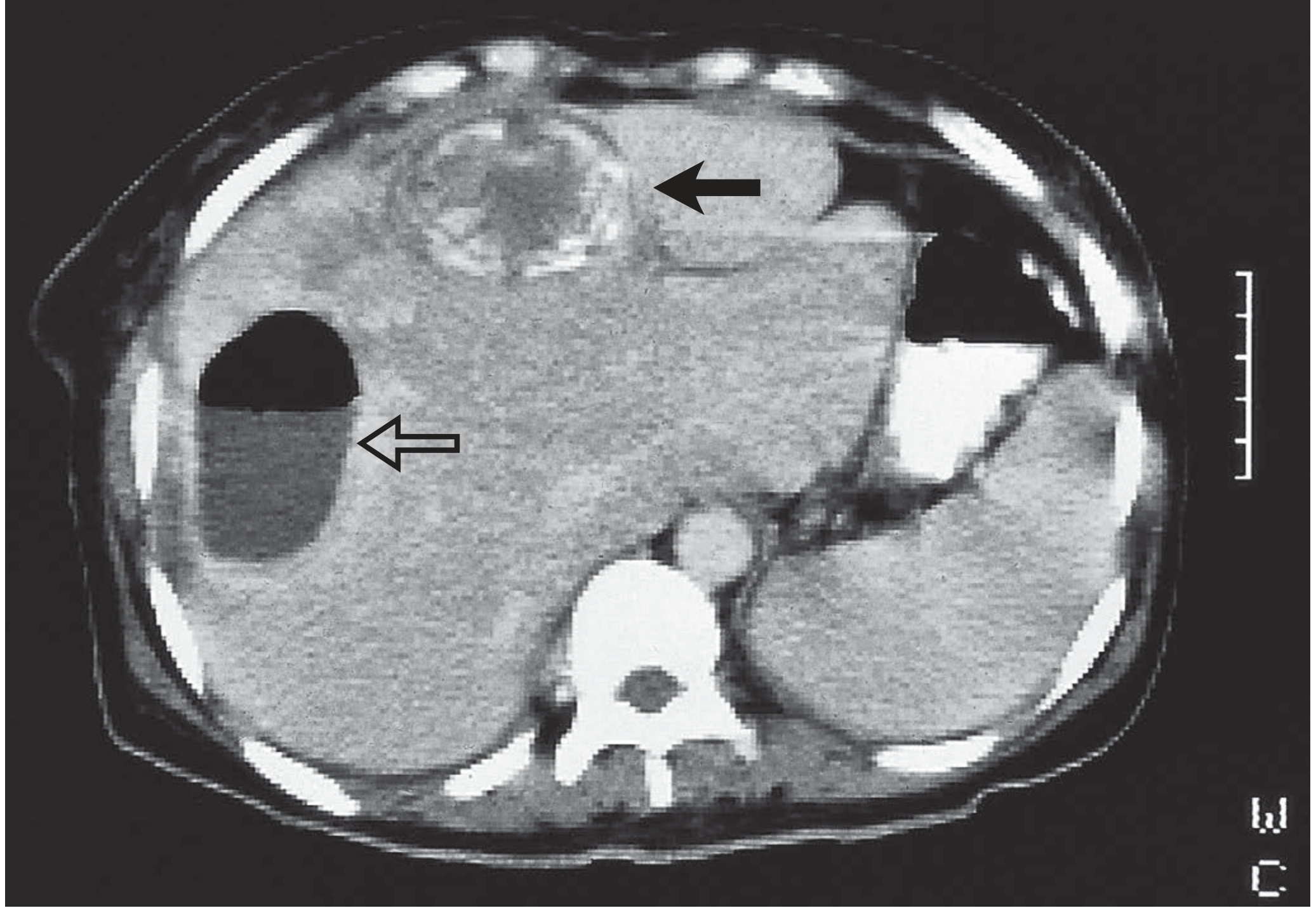
Contents of the cyst:
- Hydatid fluid: clear, colorless, antigenic; contains salts, enzymes, proteins, and toxic substances; under high pressure
- Brood capsules: small cellular masses budding from the germinal layer, each containing future worm heads (protoscoleces)
- Protoscoleces: each has 4 suckers and a double row of hooks; ~400,000 per mL of fluid; can differentiate into adult tapeworms in a definitive host or into new daughter cysts in an intermediate host
- Hydatid sand: the combination of freed brood capsules + protoscoleces + calcareous bodies (appears as echogenic foci on ultrasound)
- Daughter cysts: formed when the endocyst proliferates; replicas of the mother cyst; develop after >6 months of cyst growth
Endogenic vs. Ectogenic vesiculation:
- Endogenic (normal): daughter cysts form within the mother cyst
- Ectogenic: the germinal layer protrudes through a small defect in the laminated membrane to form a satellite cyst - characteristic of E. multilocularis, leading to fulminant multilocular infiltration, necrosis, and hepatic insufficiency - Maingot's
Complications of Untreated Cysts
Complications arise in approximately one-third of patients:
- Rupture into the biliary tree - most common complication (biliary communication occurs in up to 80% of cases from progressive pressure erosion); presents as cholangitis, obstructive jaundice, or biliary colic with passage of membrane fragments
- Secondary infection/superinfection - cyst becomes a pyogenic abscess
- Rupture into the peritoneum - can cause acute abdomen, anaphylactic shock, and catastrophic seeding ("white cancer") - very difficult to treat
- Rupture into the pleural/pulmonary cavity - bronchopleural fistula; "hydatid vomica" (expectoration of salty cyst fluid + white membranes)
- Anaphylaxis - from leak or rupture of cyst antigens into the bloodstream
- Compression of adjacent structures - portal hypertension, IVC obstruction, biliary obstruction
- Cyst calcification and death - benign outcome; but calcification does not guarantee death of the parasite
Part 2 - Classification
WHO-IWGE Classification (2003, Updated) - Gold Standard
The Gharbi ultrasound classification (1981) categorized cysts into 5 types (I-V) based solely on morphology. In 1995-2003, the WHO Informal Working Group on Echinococcosis (WHO-IWGE) published a standardized classification incorporating both functional parasite status (active/transitional/inactive) and ultrasonographic appearance, designated CE1-CE5. This system guides treatment selection. - Current Surgical Therapy 14e, Bailey & Love's
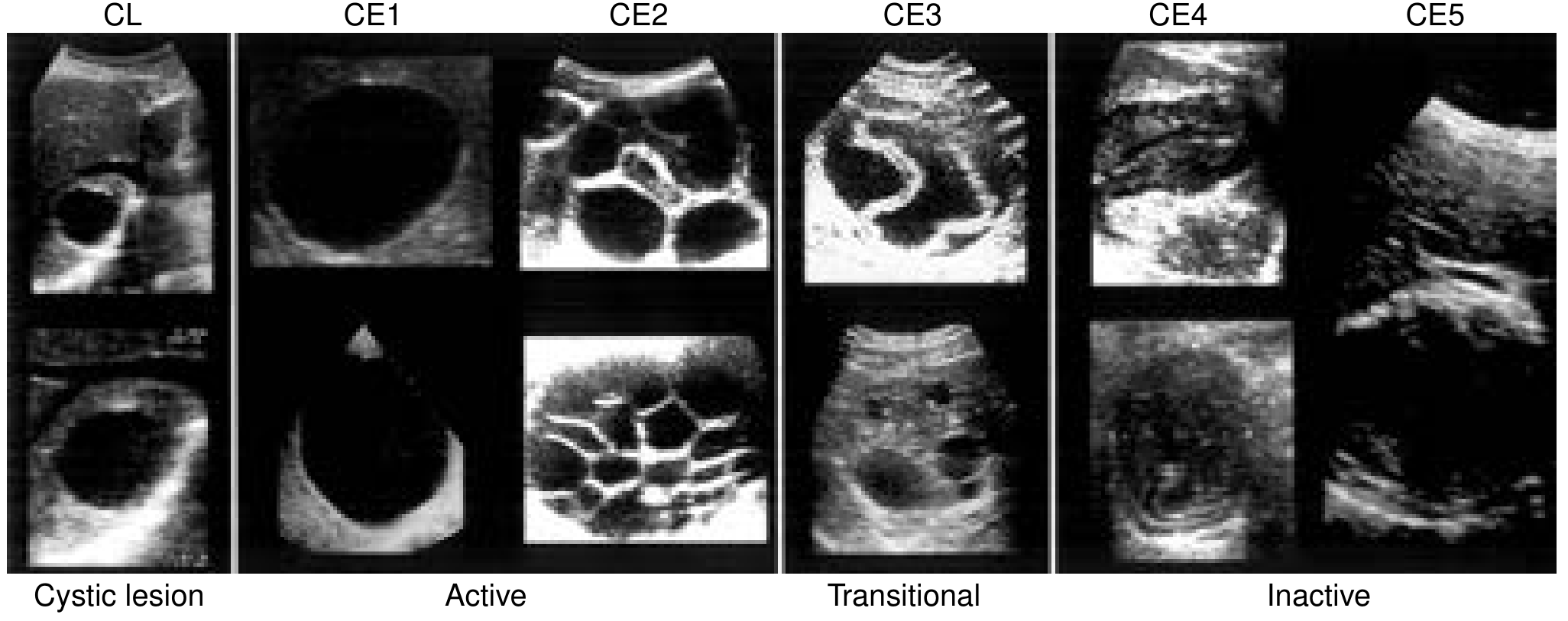
| WHO Stage | Gharbi | Status | Ultrasound Appearance | Biological Features | Treatment |
|---|---|---|---|---|---|
| CL (Cystic Lesion) | - | Active | Unilocular, anechoic; cyst wall not visible | Early stage, not yet fertile; requires diagnostic workup to confirm echinococcosis | Needs diagnosis first |
| CE1 | Type I | Active | Unilocular, anechoic, oval/round; cyst wall visible; hydatid sand (snowflake sign) | Pathognomonic; usually fertile | <5 cm: albendazole alone; >5 cm: PAIR + albendazole |
| CE2 | Type III | Active | Multivesicular, septated; rosette/honeycomb/"cartwheel" appearance; daughter cysts present | Pathognomonic; usually fertile | Percutaneous therapy or surgery + albendazole |
| CE3 | Type II | Transitional | Detached, floating laminated membrane (water-lily sign); less round; complex mass; 3A - daughter cysts with detached membrane; 3B - daughter cysts in solid matrix | Starting to degenerate but may still contain viable protoscolices | PAIR, percutaneous therapy, or surgery + albendazole |
| CE4 | Type IV | Inactive | Heterogenous, hypoechoic; degenerating membrane; no daughter cysts; "ball of wool" appearance | Most not fertile; needs serological confirmation | Surgery + albendazole, or watch and wait |
| CE5 | Type V | Inactive | Thick, calcified wall; arch-shaped with cone-shaped posterior acoustic shadow | Highly suggestive of echinococcosis; most not fertile | Watch and wait (if confirmed dead); surgery if uncertain |
Three functional groups (Bailey & Love's):
- Group 1 (Active): CE1, CE2 - cysts >2 cm, often fertile
- Group 2 (Transitional): CE3 - degenerating but may still harbor viable protoscolices
- Group 3 (Inactive): CE4, CE5 - degenerated, partially or totally calcified; unlikely to contain viable protoscolices
Important: Calcification does not always confirm a dead cyst. If an inactive cyst is enlarging on serial imaging, it should be treated. - Bailey & Love's
Part 3 - Investigations
A. Clinical Assessment
- History of exposure: sheep-farming, dog contact, endemic area travel
- 75% of patients are asymptomatic at diagnosis
- When symptomatic: RUQ/epigastric pain (20%), dyspepsia (13%), fever/chills (8%), jaundice (6%)
- Signs: RUQ mass (70%), RUQ tenderness (20%)
B. Laboratory Tests
| Test | Finding | Notes |
|---|---|---|
| Eosinophil count | Elevated in ~35% | Non-specific; absent in ~65% |
| Bilirubin | >2 mg/dL in ~20% | Suggests biliary communication |
| WBC | Usually normal | Leukocytosis if infected |
| LFTs | May be elevated | Non-specific |
C. Serology (Immunodiagnostics)
Serology is confirmatory, not definitive on its own. No single test is pathognomonic.
| Test | Sensitivity | Notes |
|---|---|---|
| ELISA (antigen 5 + antigen B) | >90% | Detects specific antigens/immune complexes; IgE antibodies by ELISA/RAST confirm active disease |
| Arc 5 antibody test (immunoelectrophoresis) | 91% | Precipitation with antigen 5; highly specific |
| Purified antigen fractions (5 + B + glycoproteins) | 95% sensitivity, 100% specificity | Best available serological performance - Maingot's |
| Casoni skin test | Abandoned | Low sensitivity and specificity |
| Weinberg test | Abandoned | Low sensitivity |
Serology may be negative if: the cyst has never leaked, contains no scolices (sterile cyst), or the parasite is no longer viable (calcified, dead cyst). - Schwartz's
D. Imaging
Chest X-Ray
- May show elevated right hemidiaphragm
- Concentric calcifications in cyst wall
- Limited diagnostic value alone
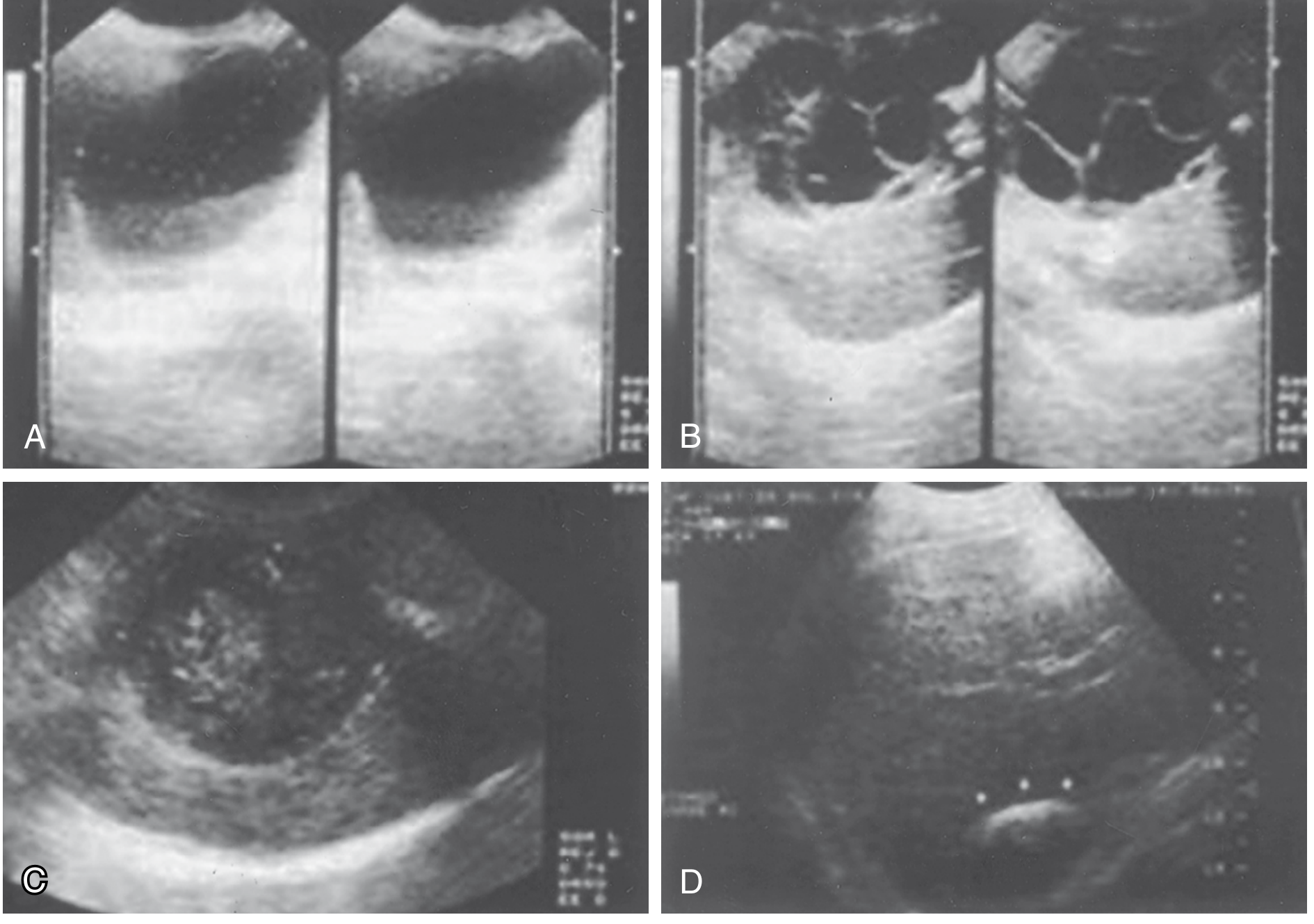
Ultrasound (First-Line Investigation)
- Preferred initial modality - widely available, inexpensive, radiation-free, and can be performed bedside
- Specificity ~90% for hydatid disease
- Defines: internal structure, number and location of cysts, presence of daughter cysts, biliary communication, and complications
- Can detect cysts as small as 1 cm
- Pathognomonic signs: hydatid sand (mobile echogenic foci = "snowflake sign"), floating membrane (water-lily sign), daughter cysts with rosette/honeycomb appearance
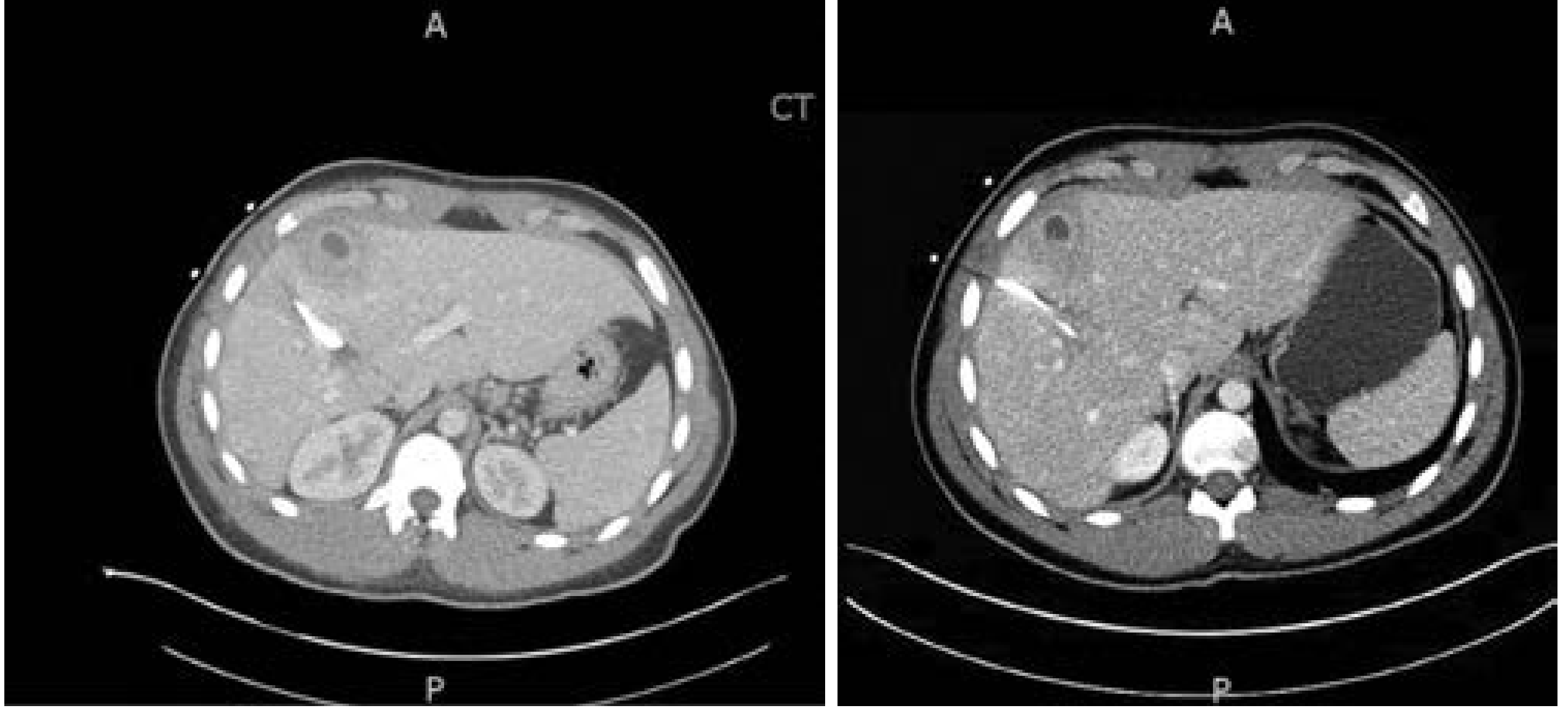
CT Scan
- Most accurate for surgical planning
- Clearly defines: cyst location relative to bile ducts and vascular structures, extent of calcification, biliary communication, and extrahepatic disease
- Ring-like pericyst calcifications present in 20-30% on CT
- Dense total calcification suggests a dead/inactive cyst
- Daughter cysts appear slightly hypodense compared to the mother cyst
MRI
- Best modality for evaluating pericyst characteristics, cyst matrix, and daughter cyst composition
- Useful when CT is equivocal or for central cysts near portal structures
- MRCP can demonstrate biliary communication even before clinical jaundice
ERCP / MRCP
- Indicated when biliary communication is suspected preoperatively (jaundice, cholangitis, elevated ALP)
- Cholangiography or ERCP should be performed before any percutaneous drainage to rule out biliary communication (injection of scolicidal agent into a communicating biliary tree causes sclerosing cholangitis)
Aspiration without preparation is contraindicated - risk of anaphylaxis and peritoneal seeding. - Rosen's Emergency Medicine
Part 4 - Management
Overview: Decision Framework
Treatment is individualized based on:
- Cyst type (WHO-IWGE classification)
- Size, number, and location of cysts
- Presence of complications (biliary communication, rupture, infection)
- Patient factors (fitness for surgery, comorbidities, pregnancy, age)
- Available expertise and infrastructure
Small (<4 cm), deep, asymptomatic, inactive or calcified cysts (CE4/CE5) can be managed conservatively with watchful waiting and serial ultrasound. - Maingot's
Treatment Options Summary
| Modality | Recurrence | Morbidity | Best For |
|---|---|---|---|
| Medical therapy alone | 70-80% | Lowest | Disseminated disease, unfit patients |
| PAIR + albendazole | ~10% | Low (8% major, 13% minor) | CE1, CE3, infected, high-risk patients |
| Open cyst evacuation (conservative) | ~20% | Moderate (5% major) | Peripheral cysts |
| Minimally invasive (laparoscopic) evacuation | ~20% | Moderate | Anterior, peripheral cysts |
| Pericystectomy | ~10% | Higher (20% major) | Peripheral cysts, expert centers |
| Liver resection / transplantation | ~10% | Highest (40% morbidity) | Complex central cysts, E. multilocularis |
A. Medical Therapy (Anthelmintic)
Albendazole - drug of choice
- Dose: 400 mg orally twice daily (in patients ≥60 kg); or 10-15 mg/kg/day divided BD (in patients <60 kg); max 800 mg/day
- Mechanism: absorbed from the GI tract, metabolized by the liver to its active sulfoxide form; concentrates well in cyst fluid
- Mebendazole is inferior: poorly absorbed and inactivated by the liver
- Success rate as monotherapy: ~30% (cyst disappearance in <50% of patients)
- Praziquantel (25 mg/kg/day orally) combined with albendazole is superior to albendazole alone
Role of medical therapy:
- Adjunct to all interventions - given preoperatively (minimum 1 day, ideally ≥3 months) and postoperatively (minimum 1 month if viable scolices present)
- Reduces cyst viability and risk of recurrence after intraoperative spillage
- Alone: only for widely disseminated disease or patients unfit for any intervention; NOT indicated for inactive/calcified cysts (except in complicated disease)
Side effects of albendazole: neutropenia, hepatotoxicity, nausea, alopecia - monitor CBC and LFTs.
B. PAIR (Puncture - Aspiration - Injection - Re-aspiration)
The primary percutaneous technique, endorsed by WHO for selected patients.
Technique:
- Albendazole started preoperatively
- Under ultrasound or CT guidance, the cyst is punctured with a fine needle
- Cyst contents are aspirated (clear "hydatid water")
- Contrast is injected to confirm no biliary communication (mandatory before scolicidal instillation)
- Scolicidal agent is instilled and left for 10-30 minutes
- Complete re-aspiration of scolicidal agent and residual contents
- Final irrigation with 0.9% saline
More than 4,000 PAIR interventions have been performed globally, establishing its safety profile.
Scolicidal agents (WHO recommended): 20% hypertonic saline (contact ≥15 minutes); 70-95% ethanol; cetrimide 0.5%. Chlorhexidine gluconate 0.04% is an emerging preferred agent - non-toxic to bile ducts, not diluted by cyst fluid, 100% effective on protoscoleces. Formalin is abandoned (causes sclerosing cholangitis).
Indications:
- CE1 and CE3 cysts >5 cm
- CE2 cysts (multivesicular - may need catheter drainage variant)
- Infected cysts
- Patients refusing or unfit for surgery
- Failure of medical therapy alone
- Post-surgical recurrence
Contraindications:
- Biliary communication (confirmed or suspected)
- Pulmonary communication
- Peritoneal rupture
- CE4 or CE5 (inactive/calcified) cysts
- Inaccessible or superficial cysts at risk of peritoneal leak
- Children <3 years
Results: Recurrence rate 0-4%; PAIR + albendazole shows 70% success rate. Meta-analysis demonstrated PAIR + chemotherapy had higher cure rate, fewer complications, and shorter hospital stay versus historic surgical controls (though methodologic limitations exist). - Current Surgical Therapy 14e
C. Percutaneous Catheter Drainage (Modified PAIR)
An indwelling catheter is left in place rather than performing single-session aspiration. The catheter remains until daily output is <10 mL/day.
Reserved for:
- Giant unilocular cysts (>10 cm)
- Infected cysts (acts like a pyogenic abscess drain)
- CE3B or CE2 cysts with thick, viscous contents requiring multiple sessions
ERCP adjunct: Cyst-biliary complications after PAIR can be managed endoscopically (sphincterotomy + stenting) or with cyanoacrylate infusion into the fistula.
D. Laparoscopic Surgery
Indications
- CE1, CE2, CE3 cysts: anterior, peripheral, non-calcified
- Cysts in segments VI-VII (right lateral approach)
- 1-3 cysts
- No biliary communication
Not Suitable For
- Posterior/central/deeply buried cysts
-
3 cysts
- Heavy calcification (thick pericyst)
- Biliary communication requiring formal biliary reconstruction
Laparoscopic Marsupialization (Deroofing)
- Hypertonic saline-soaked packs placed around the cyst field
- Cyst aspirated with 14-gauge needle (endocyst shrinks away from pericyst)
- Roof of pericyst excised; daughter cysts and germinal membrane evacuated
- Cavity irrigated with scolicidal agent
- Any biliary communication oversewn
- Omentoplasty - pedicled omentum sutured into the residual cavity to obliterate dead space and reduce bile leak
Laparoscopic Cystopericystectomy (Total Pericystectomy)
- The entire cyst is excised intact without entering it
- Ideal for small, superficial cysts in expert centers
- Lowest recurrence rate among minimally invasive approaches
- Requires advanced laparoscopic hepatobiliary skills
E. Open Surgery
Indications for Open Surgery
- Large CE2-CE3 cysts with multiple daughter cysts
- Cysts at risk of spontaneous rupture (superficial)
- Biliary communication (especially when percutaneous options not available)
- Peritoneal rupture
- Pulmonary/bronchial communication
- Failure of percutaneous approaches
- Mass effect on adjacent vital structures
- Central/posterior/deeply located cysts
Conservative (Partial) Approaches
1. Open Cyst Evacuation (Marsupialization)
- Field packed with 20% hypertonic saline-soaked gauze
- Cyst aspirated via closed high-suction system
- Cyst opened completely; debris meticulously cleared
- Cavity irrigated with scolicidal agent
- Biliary openings identified and oversewn
- Residual cavity managed by omentoplasty
- Recurrence: 10-30%
2. Capitonnage / Introflexion
- The remaining pericyst walls are sutured together (invaginated) to obliterate the residual cavity
- Used when omentoplasty is not feasible
Radical Approaches (Lower Recurrence, Higher Morbidity)
3. Pericystectomy (Total or Subtotal)
- Entire cyst, including the pericyst, is removed intact
- Requires precise knowledge of bile duct and vascular anatomy
- Recurrence: ~10%
- Major morbidity (bile leak, bleeding): ~20%
4. Hepatic Resection (Segmentectomy / Lobectomy)
- For centrally located cysts or those involving major vascular/biliary structures
- Ensures complete removal with lowest recurrence
- Most suitable for large CE2-CE3 cysts, failed pericystectomy, or E. multilocularis
- Morbidity ~40%; formal planning with intraoperative ultrasound essential
- Recurrence: ~10%
5. Liver Transplantation
- Reserved for end-stage E. multilocularis with extensive hepatic destruction
- Rare indication
Principles of Intraoperative Spillage Prevention
- Peritoneal cavity lined with hypertonic saline-soaked packs before cyst opening
- Closed suction aspiration system used
- Scolicidal agent injected after evacuation (never before - high intracyst pressure risks rupture)
- If spillage occurs: peritoneal washout with hypertonic saline + albendazole 3-6 months + praziquantel 7 days
- Scolicidal injection contraindicated if biliary communication is present (sclerosing cholangitis)
F. Management of Specific Complications
| Complication | Management |
|---|---|
| Biliary communication | Open surgery with suture closure of biliary openings; ERCP + sphincterotomy for postoperative biliary fistula; ERCP + stenting for biliary obstruction |
| Cyst infection/superinfection | Antibiotics + percutaneous catheter drainage (treat like pyogenic abscess) |
| Peritoneal rupture | Emergency open surgery; peritoneal washout with hypertonic saline; long-course albendazole |
| Pulmonary/bronchial rupture | Open thoracotomy; suture repair of bronchial fistula |
| Anaphylaxis | IV epinephrine + corticosteroids; surgical team should always have these available intraoperatively |
Summary Decision Algorithm
Hepatic Hydatid Cyst
│
├── Inactive (CE4/CE5) + asymptomatic → Watch and wait
│
├── Small (<4 cm), deep, uncomplicated → Albendazole alone
│
├── CE1 or CE3 (>5 cm), no biliary comms → PAIR + albendazole
│
├── CE2 / giant cysts / infected → Catheter drainage + albendazole
│
├── Anterior/peripheral, 1-3 cysts, no biliary comms → Laparoscopic surgery
│
├── Biliary communication / posterior / multiple / large → Open surgery
│
└── Failed all above / E. multilocularis → Hepatic resection ± transplantation
Sources:
- Maingot's Abdominal Operations - Ch. 43
- Current Surgical Therapy, 14th Ed. - (Hydatid Disease section)
- Sabiston Textbook of Surgery, 21e - Ch. 89
- Bailey & Love's Short Practice of Surgery, 28th Ed. - Ch. 6 & Ch. 69
- Rosen's Emergency Medicine - Ch. 122
- Schwartz's Principles of Surgery, 11th Ed. - Ch. 31
This is a shared conversation. Sign in to Orris to start your own chat.