Explain the visual pathway. Describe the vision field defects produced by the lesion at various level. With images.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have all the material I need - rich textbook content and multiple high-quality images. Let me compile the comprehensive answer.
The Visual Pathway and Visual Field Defects
Overview of the Visual Pathway
The visual pathway runs from the retina to the primary visual cortex (area 17, striate cortex) in the occipital lobe. It can be divided into six anatomical segments, each with distinct clinical significance.
1. Retina
The retina contains photoreceptors (rods and cones). Signals pass to bipolar cells and then to retinal ganglion cells, whose axons converge at the optic disc (the physiological blind spot - no photoreceptors here). The nasal retina receives light from the temporal visual field; the temporal retina receives light from the nasal field. The upper retina receives light from the inferior visual field and vice versa.
2. Optic Nerve (CN II)
Ganglion cell axons coalesce at the optic disc, acquire a myelin sheath from oligodendrocytes, and are enveloped by cranial meninges - making the optic nerve a true CNS white matter tract rather than a peripheral nerve.
3. Optic Chiasm
The two optic nerves meet anterior to the infundibular stalk at the optic chiasm. Here:
- Nasal retinal fibers decussate to join the contralateral optic tract (carrying temporal field information)
- Temporal retinal fibers stay ipsilateral (carrying nasal field information)
The chiasm lies in close relation to the pituitary gland and floor of the third ventricle - a key anatomical relationship for understanding compressive lesions.
4. Optic Tracts
Each optic tract now carries fibers representing the contralateral visual hemifield from both eyes: the ipsilateral temporal retina + contralateral nasal retina. The tracts course around the midbrain to reach the lateral geniculate nucleus (LGN).
A small number of fibers branch off to the pretectal area and superior colliculus for the pupillary light reflex (not for conscious vision).
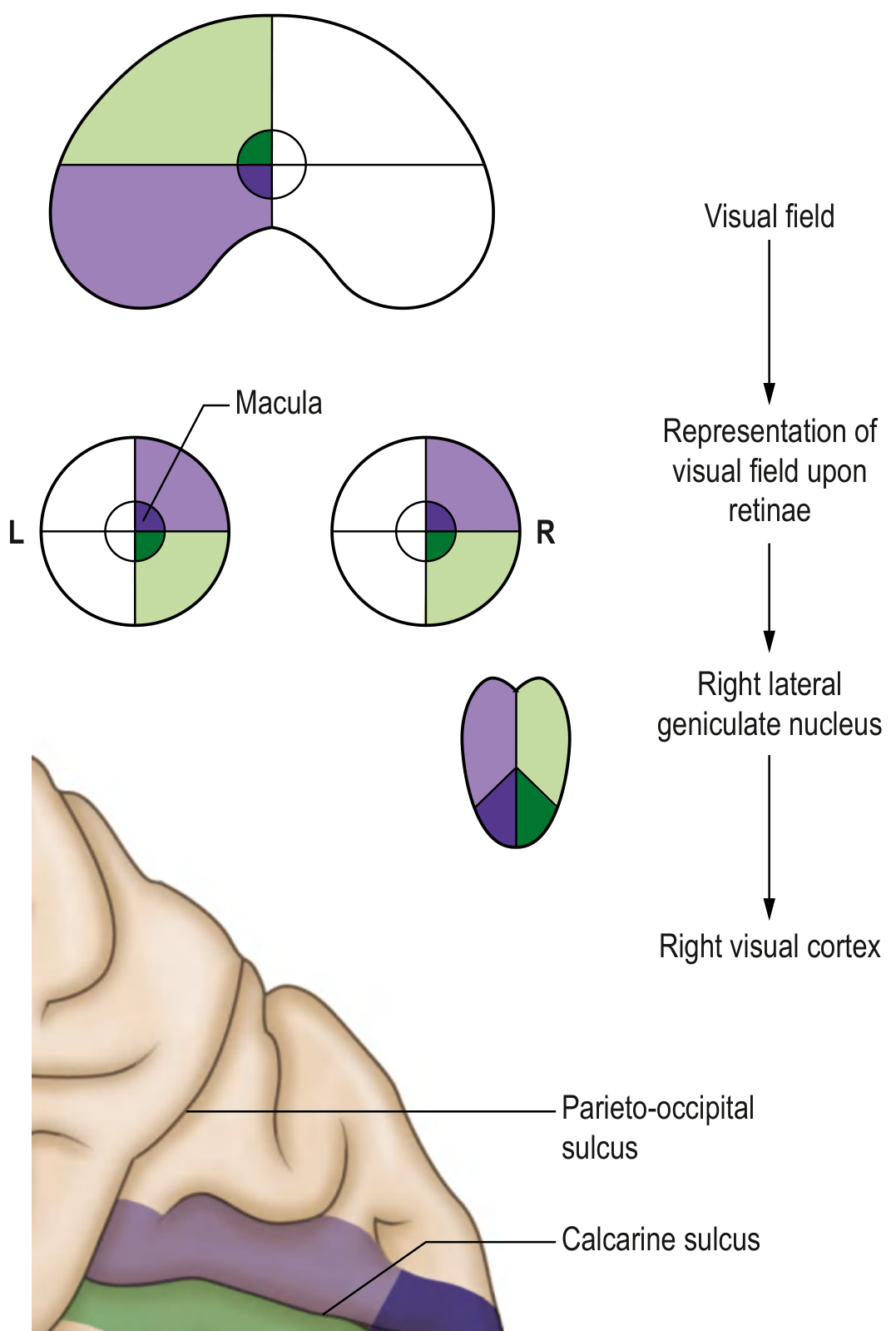
5. Lateral Geniculate Nucleus (LGN) of the Thalamus
The LGN is a 6-layered relay nucleus. The visual field is rotated 90° here: inferior field projects to the medial half; superior field projects to the lateral half. Axons leaving the LGN form the optic radiations (geniculocalcarine tract).
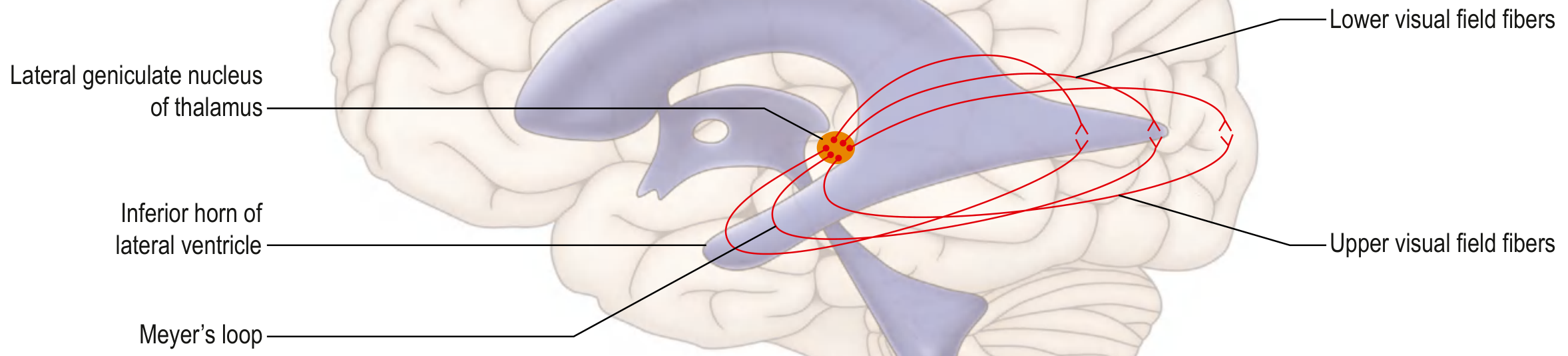
6. Optic Radiations (Geniculocalcarine Tract)
The optic radiations fan out in two divisions - this is clinically the most important segment for quadrantanopias:
- Lower fibers (Meyer's loop): Carry upper visual field signals. They sweep anteriorly into the temporal lobe around the inferior horn of the lateral ventricle before turning posteriorly to the calcarine cortex.
- Upper fibers (parietal pathway): Carry lower visual field signals. They travel more directly through the parietal lobe.
7. Primary Visual Cortex (Area 17, Striate Cortex)
Located along the calcarine fissure of the occipital lobe:
- Upper bank of calcarine fissure receives lower visual field signals
- Lower bank receives upper visual field signals
- The macular (foveal) representation is disproportionately large and occupies the most posterior portion (occipital pole)
Visual Field Defects at Each Level
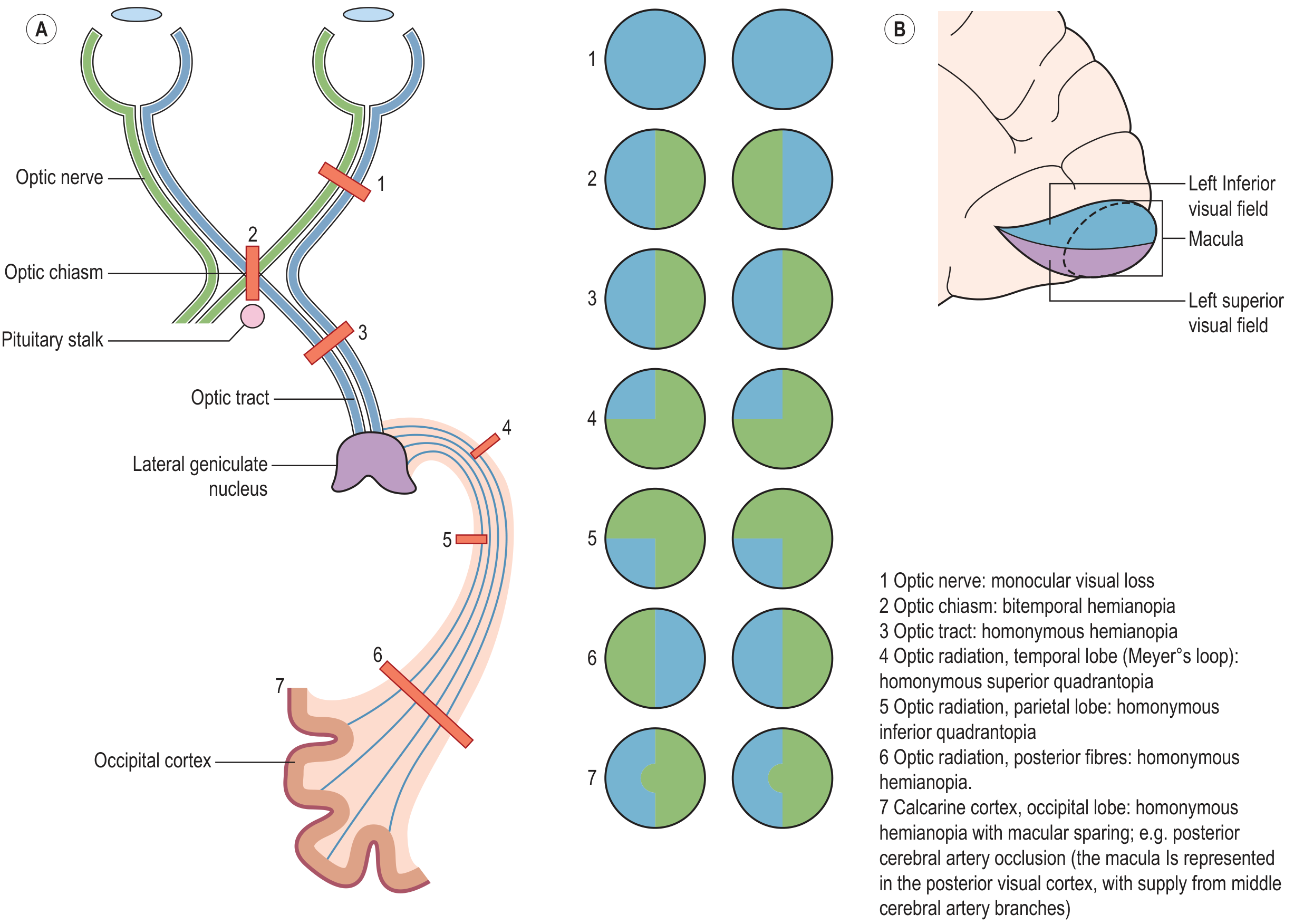
The master diagram below shows lesions A-J and their resulting defects:
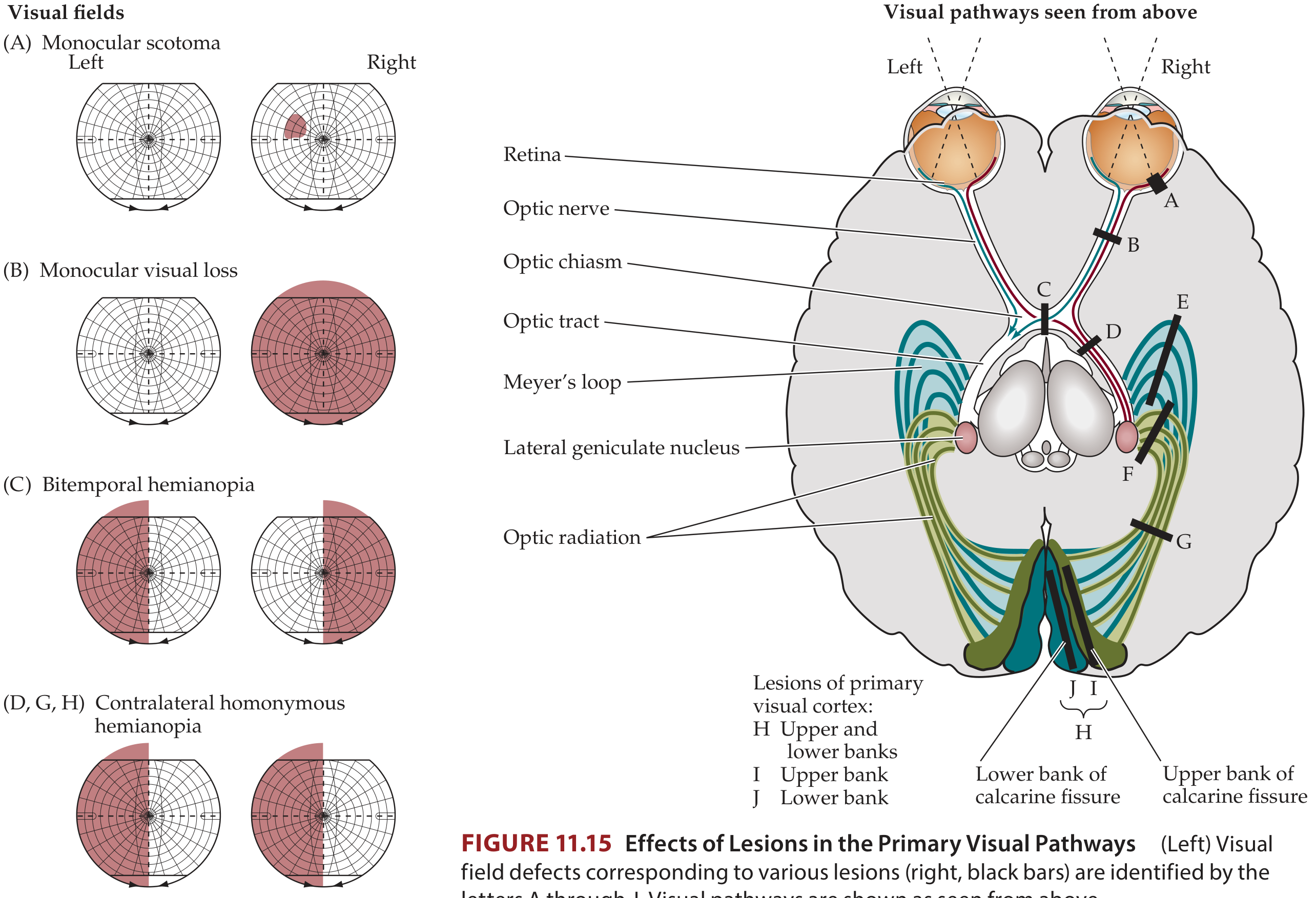
Level 1 - Retina or Optic Nerve (pre-chiasmal)
| Defect | Description |
|---|---|
| Monocular scotoma | Partial loss in one eye only; location/size depends on lesion site on retina or nerve |
| Monocular amaurosis (complete blindness) | Total loss of vision in one eye - the entire optic nerve or retina affected |
- Key rule: Any purely monocular visual loss = lesion at or anterior to the chiasm (retina or optic nerve)
- Causes: Optic neuritis (MS), glaucoma, anterior ischemic optic neuropathy, retinal infarct/detachment, elevated ICP (papilloedema), optic nerve tumors
Level 2 - Optic Chiasm
| Defect | Description |
|---|---|
| Bitemporal hemianopia | Loss of the outer (temporal) half of each eye's visual field |
- Mechanism: Crossing nasal retinal fibers are damaged. Since nasal fibers carry temporal field signals, both temporal fields are lost.
- Key rule: Bitemporal hemianopia = chiasmal lesion
- Causes: Pituitary adenoma (most common), craniopharyngioma, meningioma, hypothalamic glioma
- The defect is often asymmetrical in practice
Level 3 - Optic Tract
| Defect | Description |
|---|---|
| Contralateral homonymous hemianopia | Loss of the same hemifield in both eyes (e.g., right optic tract lesion → left homonymous hemianopia) |
- Incongruous (not perfectly matched between the two eyes) because fibers from each eye are not yet fully mingled
- Causes: Tumors, infarct, demyelination (relatively uncommon location)
Level 4 - Lateral Geniculate Nucleus
| Defect | Description |
|---|---|
| Contralateral homonymous hemianopia | Similar to optic tract; occasionally a "keyhole" sectoranopia |
- Causes: Infarct (anterior choroidal or posterior choroidal artery territory), tumor, hemorrhage, toxoplasmosis
Level 5 - Optic Radiations
This level produces quadrantanopias, depending on which part of the radiation is damaged:
| Sub-location | Defect | Mnemonic |
|---|---|---|
| Temporal lobe (Meyer's loop) | Contralateral superior quadrantanopia | "Pie in the sky" |
| Parietal lobe (upper radiation) | Contralateral inferior quadrantanopia | "Pie on the floor" |
| Entire optic radiation | Contralateral homonymous hemianopia |
- Temporal lobe causes: MCA inferior division infarct, temporal lobe tumor, surgery (e.g., temporal lobectomy for epilepsy)
- Parietal lobe causes: MCA superior division infarct, tumor, trauma
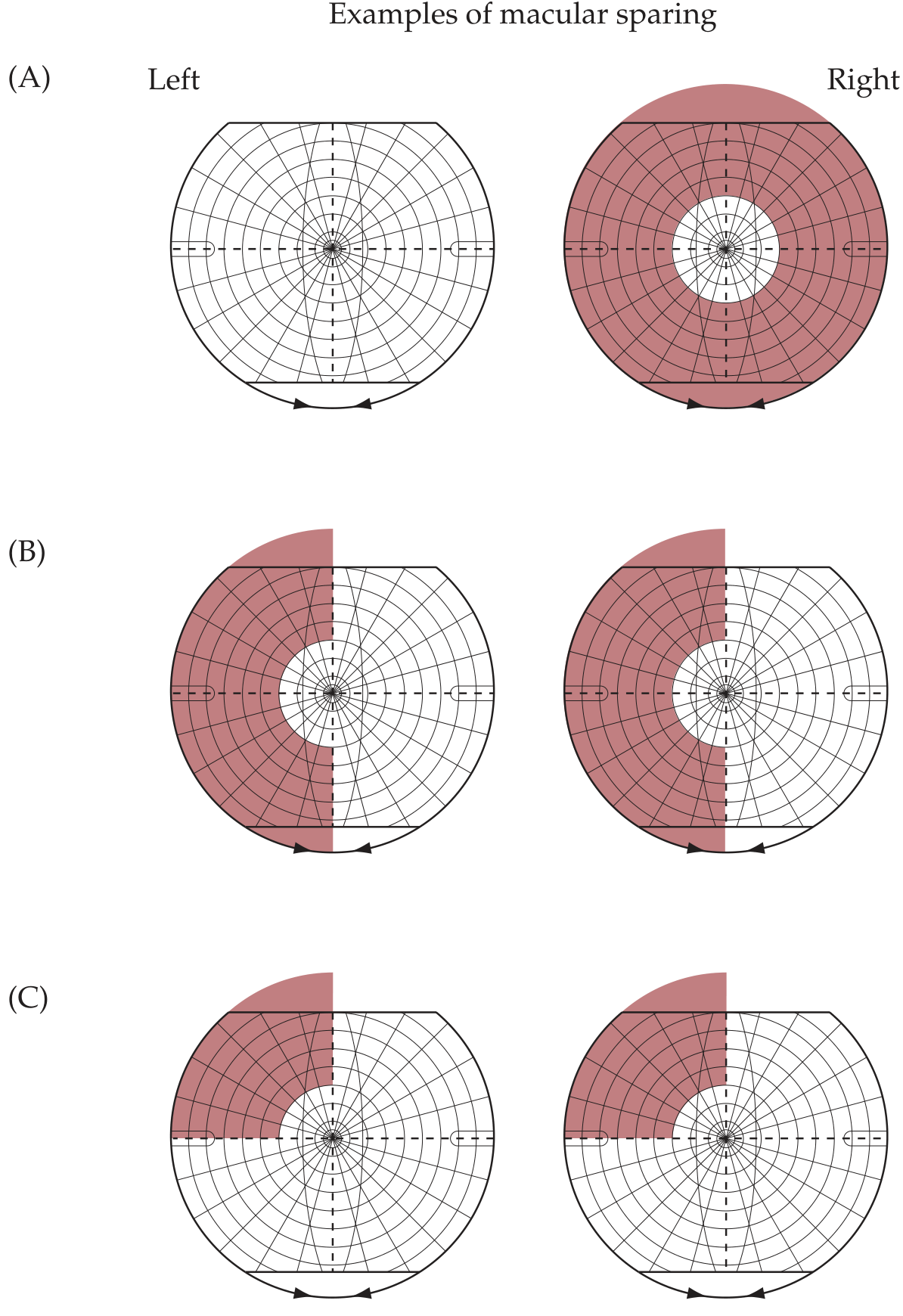
Level 6 - Primary Visual Cortex (Calcarine Cortex, Occipital Lobe)
| Sub-location | Defect |
|---|---|
| Upper bank of calcarine fissure | Contralateral inferior quadrantanopia |
| Lower bank of calcarine fissure | Contralateral superior quadrantanopia |
| Entire primary visual cortex | Contralateral homonymous hemianopia |
| Occipital pole (macular area) | Central homonymous scotoma |
- Cortical lesions are typically congruous (nearly identical defect in both eyes) because fibers from both retinae are now fully interdigitated
- Macular sparing: Posterior cerebral artery (PCA) occlusions causing cortical hemianopia often spare central vision because the occipital pole (macular representation) receives collateral supply from the MCA
- Causes: PCA infarct (most common), tumor, trauma to occipital pole, hemorrhage
Macular Sparing
Comprehensive Summary Diagram (Grainger & Allison)
Quick Reference Summary Table
| Lesion Site | Visual Field Defect | Congruity | Key Cause |
|---|---|---|---|
| Retina / Optic nerve | Monocular scotoma or blindness | N/A (one eye only) | Optic neuritis, glaucoma, AION |
| Optic chiasm | Bitemporal hemianopia | Heteronymous | Pituitary adenoma |
| Optic tract | Contralateral homonymous hemianopia | Incongruous | Tumor, infarct |
| LGN | Contralateral homonymous hemianopia | Incongruous | Infarct, tumor |
| Temporal lobe (Meyer's loop) | Contralateral superior quadrantanopia ("pie in the sky") | Congruous | MCA inf. division infarct, temporal tumor |
| Parietal lobe (upper radiation) | Contralateral inferior quadrantanopia ("pie on the floor") | Congruous | MCA sup. division infarct |
| Entire optic radiation | Contralateral homonymous hemianopia | Congruous | Large MCA infarct |
| Visual cortex | Contralateral homonymous hemianopia ± macular sparing | Highly congruous | PCA infarct |
Sources: Neuroanatomy through Clinical Cases, 3rd Ed.; Gray's Anatomy for Students; Goldman-Cecil Medicine; Grainger & Allison's Diagnostic Radiology; Kanski's Clinical Ophthalmology, 10th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.